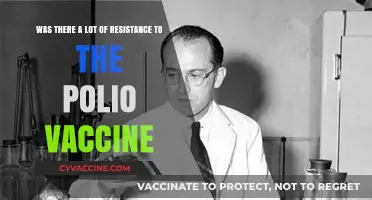
In 2003, the world faced a significant public health challenge with the outbreak of Severe Acute Respiratory Syndrome (SARS), a highly contagious and deadly virus that spread rapidly across multiple countries. Despite intensive research efforts, no vaccine was developed and approved for widespread use during the SARS outbreak, which was eventually contained through strict public health measures such as quarantine, contact tracing, and improved infection control practices. The absence of a SARS vaccine at the time highlighted the complexities and challenges of vaccine development, particularly for novel and rapidly evolving viruses, and underscored the importance of global preparedness and collaboration in responding to emerging infectious diseases.
| Characteristics | Values |
|---|---|
| Existence of SARS Vaccine in 2003 | No vaccine was available or approved for SARS in 2003. |
| SARS Outbreak Period | 2002–2004 |
| Reason for No Vaccine | The outbreak was contained quickly, reducing the urgency for vaccine development. |
| Vaccine Development Efforts | Research began, but clinical trials were not completed due to declining cases. |
| Vaccine Candidates in Trials | Several candidates entered preclinical and early clinical trials. |
| Challenges in Development | Short outbreak duration, lack of funding, and scientific hurdles. |
| Current Status (2023) | No SARS vaccine has been developed or approved post-2003. |
| Legacy Impact | Research on SARS vaccines contributed to COVID-19 vaccine development. |
Explore related products


$9.99 $11.75




What You'll Learn
![]()
SARS Vaccine Development Timeline
The SARS (Severe Acute Respiratory Syndrome) outbreak in 2002-2003 prompted an urgent global effort to understand the virus and develop countermeasures, including vaccines. However, by the time the outbreak was contained in mid-2003, no SARS vaccine had been approved for human use. The timeline of SARS vaccine development reflects the challenges of responding to a novel pathogen and the complexities of vaccine creation. Initial research focused on identifying the SARS-CoV-1 virus as the causative agent, which was achieved within months of the outbreak. Scientists quickly sequenced the virus's genome, laying the groundwork for vaccine development. Early efforts prioritized inactivated virus vaccines and recombinant protein-based approaches, as these were well-established technologies.
Between 2003 and 2006, several vaccine candidates entered preclinical and early clinical trials. For instance, inactivated SARS vaccines developed by Chinese and U.S. researchers showed promise in animal models, inducing neutralizing antibodies and protecting against viral replication. Phase I clinical trials in humans demonstrated safety and immunogenicity, but the studies were limited in scale due to the declining urgency as SARS cases ceased. Recombinant vaccines targeting the spike protein, a key viral component, also progressed to clinical trials, showing potential but requiring further optimization. Despite these advances, the absence of ongoing SARS cases made it difficult to conduct large-scale efficacy trials, slowing development.
By the late 2000s, interest in SARS vaccines waned as the outbreak remained contained and resources shifted to other priorities, such as influenza and emerging pathogens. However, the research was not in vain. The knowledge gained from SARS vaccine development, particularly in understanding coronaviruses and vaccine platforms, proved invaluable during the COVID-19 pandemic. Technologies like mRNA and viral vector vaccines, which were in their infancy during the SARS era, built on this foundation. The SARS experience highlighted the need for rapid, coordinated responses to emerging diseases and the importance of sustained investment in vaccine research, even when immediate threats subside.
In summary, while there was no SARS vaccine available in 2003, significant progress was made in the years following the outbreak. The timeline of SARS vaccine development underscores the challenges of creating vaccines for novel pathogens, from initial research to clinical trials, and the impact of epidemiological context on prioritization. The lessons learned from SARS directly contributed to the unprecedented speed of COVID-19 vaccine development, demonstrating the long-term value of scientific preparedness. Although SARS vaccines never reached widespread use, their development marked a critical step in global health security and pandemic response.
Display Your COVID-19 Vaccine Card on iPhone: A Simple Guide
You may want to see also
Explore related products






![]()
Challenges in SARS Vaccine Creation
The creation of a vaccine for SARS (Severe Acute Respiratory Syndrome) in 2003 faced significant challenges, primarily due to the rapid containment of the outbreak and the limited understanding of the virus at the time. SARS emerged in late 2002 and was contained by mid-2003 through public health measures such as isolation, quarantine, and contact tracing. This swift containment reduced the urgency to develop a vaccine, as the immediate threat subsided before a vaccine could be fully developed and tested. The short duration of the outbreak meant that pharmaceutical companies and research institutions had less incentive to invest in a SARS vaccine, as the potential market for such a vaccine was uncertain.
One of the major scientific challenges in SARS vaccine creation was the novelty of the SARS-CoV virus, which belongs to the coronavirus family. At the time, there was limited knowledge about coronaviruses and their behavior in humans. Researchers had to start from scratch in understanding the virus's structure, its mechanisms of infection, and the immune response it triggered. This lack of foundational knowledge slowed down the initial stages of vaccine development, as scientists needed to identify suitable viral targets and develop methods to elicit an effective immune response.
Another challenge was the potential risk of vaccine-associated enhancement of disease. Some early studies suggested that certain vaccine candidates for SARS might cause immune responses that could worsen the disease upon exposure to the virus, a phenomenon known as antibody-dependent enhancement (ADE). This concern made researchers cautious about moving forward with vaccine trials without robust preclinical data to ensure safety. Balancing the need for speed in vaccine development with the imperative to avoid harmful side effects added complexity to the process.
The logistical and regulatory hurdles also played a significant role in delaying SARS vaccine development. Clinical trials require substantial funding, resources, and collaboration across multiple institutions and countries. In 2003, the global health infrastructure was less prepared for rapid vaccine development compared to the COVID-19 pandemic in 2020. Additionally, regulatory agencies had stricter requirements for approving vaccines, necessitating extensive testing to ensure safety and efficacy. These factors contributed to the slow progress in advancing SARS vaccine candidates through clinical trials.
Finally, the absence of a long-term market for a SARS vaccine discouraged sustained investment. Once the outbreak was contained, the virus disappeared from the human population, and there was no ongoing transmission to justify continued vaccine development. Pharmaceutical companies and research institutions shifted their focus to other priorities, leaving SARS vaccine research largely incomplete. While several vaccine candidates were in preclinical or early clinical stages by 2004, none were fully developed or approved for use in humans. This experience highlighted the challenges of developing vaccines for emerging infectious diseases with unpredictable trajectories and limited commercial viability.
Should You Get a Typhoid Vaccine When Sick? Expert Advice
You may want to see also
Explore related products






![]()
Animal Testing Results for SARS Vaccine
During the 2003 SARS outbreak, efforts to develop a vaccine were initiated, but no vaccine was fully developed, tested, or approved for human use by the time the outbreak was contained. However, animal testing played a crucial role in the early stages of vaccine development. Initial studies focused on understanding the immune response to the SARS-CoV virus and evaluating potential vaccine candidates in animal models. One of the primary animal models used was the non-human primate, particularly macaques, due to their genetic similarity to humans and susceptibility to SARS-CoV infection. These studies demonstrated that vaccinated animals developed neutralizing antibodies and showed reduced viral replication in the lungs compared to unvaccinated controls.
In addition to primates, small animal models such as mice were also employed in SARS vaccine research. Mice were genetically engineered to express the human ACE2 receptor, which allowed the virus to infect them, mimicking human susceptibility. Animal testing results in these models indicated that certain vaccine candidates, including inactivated virus vaccines and recombinant protein-based vaccines, could elicit a robust immune response. For instance, a study published in *Nature* in 2004 reported that vaccinated mice and ferrets showed reduced viral load and milder symptoms upon exposure to SARS-CoV, suggesting the potential efficacy of these vaccines.
Despite promising results in animal models, significant challenges were encountered. One major issue was the phenomenon of immune enhancement, where vaccinated animals exhibited more severe disease upon exposure to the virus. This was observed in some studies involving ferrets and non-human primates, raising concerns about vaccine safety. Researchers identified that certain vaccine formulations, particularly those using whole inactivated virus, might trigger an exaggerated immune response, leading to lung pathology. These findings underscored the need for careful evaluation and optimization of vaccine candidates before advancing to human trials.
Another critical aspect of animal testing was the assessment of long-term immunity and protection. Studies conducted over several months revealed that while vaccinated animals maintained detectable levels of neutralizing antibodies, the durability of protection varied depending on the vaccine platform. For example, viral vector-based vaccines showed more sustained immune responses compared to subunit vaccines in some animal models. These results highlighted the importance of selecting appropriate vaccine technologies to ensure both safety and efficacy in the long term.
In summary, animal testing for SARS vaccines in 2003 provided valuable insights into the potential of various vaccine candidates but also revealed challenges such as immune enhancement. While no SARS vaccine was ultimately deployed during the 2003 outbreak, the knowledge gained from these studies laid the groundwork for future vaccine development, particularly for emerging coronaviruses like SARS-CoV-2. The lessons learned from animal testing during the SARS epidemic emphasized the need for rigorous preclinical evaluation to ensure the safety and efficacy of vaccines before human use.
Is the Coronavirus Vaccine Mandatory for Healthcare Workers?
You may want to see also
Explore related products






![]()
Human Trials Status in 2003
In 2003, during the peak of the SARS (Severe Acute Respiratory Syndrome) outbreak, the global scientific community mobilized rapidly to develop a vaccine. However, by the end of 2003, no SARS vaccine had progressed to large-scale human trials. The urgency of the outbreak prompted researchers to accelerate preclinical studies, but the timeline for vaccine development, from lab to human trials, is inherently lengthy due to safety and efficacy requirements. Initial efforts focused on understanding the SARS-CoV virus, identifying potential antigens, and developing vaccine candidates using traditional and novel platforms. Despite these efforts, the containment of the outbreak by mid-2003 reduced the immediate need for a vaccine, slowing down the push for human trials.
By mid-2003, several vaccine candidates had shown promise in animal models, particularly those using inactivated virus and recombinant protein approaches. For instance, researchers at the National Institute of Allergy and Infectious Diseases (NIAID) in the United States had developed an inactivated SARS vaccine that demonstrated efficacy in monkeys. Similarly, Chinese scientists reported progress with a recombinant protein vaccine. However, these candidates were still in preclinical stages, and transitioning to human trials required rigorous safety assessments and regulatory approvals, which were not completed by the end of 2003.
Human trials for SARS vaccines in 2003 were limited to Phase I studies, which focus on safety and immunogenicity in small groups of healthy volunteers. For example, a Phase I trial of an inactivated SARS vaccine began in December 2003 at the University of Hong Kong, involving fewer than 50 participants. This trial aimed to evaluate the vaccine's safety profile and its ability to induce an immune response. However, such early-phase trials were exploratory and not designed to assess efficacy against the virus in real-world settings. The limited scope and scale of these trials meant that no SARS vaccine was close to widespread use by the end of 2003.
The absence of large-scale human trials in 2003 was partly due to logistical and ethical challenges. The SARS outbreak had been largely contained by July 2003, reducing the availability of infected individuals for efficacy studies. Additionally, the lack of a persistent SARS circulation made it difficult to justify the risks and costs of advancing vaccines to later-stage trials. Regulatory agencies also required robust data from preclinical and early-phase studies before approving larger trials, further delaying progress. As a result, while significant strides were made in vaccine development, human trials remained in their infancy by the end of 2003.
In summary, the status of human trials for a SARS vaccine in 2003 was confined to early-phase studies, with no candidate advancing to large-scale testing. The rapid containment of the outbreak, combined with the time-consuming nature of vaccine development, limited progress to Phase I trials focused on safety and immunogenicity. While these efforts laid the groundwork for future research, they did not yield a vaccine ready for public use in 2003. The experience with SARS vaccine development highlighted the challenges of responding to emerging infectious diseases and informed strategies for subsequent outbreaks, such as COVID-19.
Courts Award $4 Billion in Vaccine Injury Compensation Claims
You may want to see also
Explore related products






![]()
Reasons SARS Vaccine Wasn't Deployed
The SARS outbreak of 2002-2003 was a significant global health crisis, yet no vaccine was deployed during or immediately after the outbreak. One primary reason was the rapid containment of the virus. Public health measures such as contact tracing, quarantine, and travel restrictions effectively curbed the spread of SARS. By July 2003, the World Health Organization (WHO) declared the outbreak contained, reducing the urgency to develop and deploy a vaccine. With only around 8,000 cases and 774 deaths worldwide, the scale of the outbreak did not justify the immediate need for a vaccine, especially given the time and resources required for vaccine development.
Another critical factor was the challenges in vaccine development. While several research institutions began working on SARS vaccine candidates, the process of creating a safe and effective vaccine is complex and time-consuming. Preclinical and clinical trials, manufacturing, and regulatory approvals typically take years. By the time potential vaccines reached early clinical trials, the outbreak had already subsided, diminishing the incentive to expedite the process. Additionally, SARS-CoV, the virus causing SARS, posed specific scientific challenges, such as the risk of immune enhancement, where the vaccine could potentially worsen the disease, as observed in animal studies.
The unpredictability of SARS re-emergence also played a role in the lack of vaccine deployment. After 2003, SARS cases virtually disappeared, and there was no evidence of ongoing circulation of the virus in humans or animal reservoirs. This made it difficult to justify continued investment in vaccine development, as the immediate threat had passed. Public health officials and pharmaceutical companies shifted their focus to more pressing health concerns, such as influenza and HIV, which had a higher global disease burden.
Furthermore, economic and logistical considerations hindered the deployment of a SARS vaccine. Developing a vaccine for a disease that was no longer active was not a priority for pharmaceutical companies, as the return on investment would be uncertain. Governments and funding agencies were also reluctant to allocate resources to a vaccine for a contained outbreak when other diseases required immediate attention. The lack of a sustained market for a SARS vaccine made it financially unviable for companies to pursue large-scale production and distribution.
Lastly, the focus on preparedness rather than immediate deployment influenced the decision not to deploy a SARS vaccine. Instead of developing a vaccine for a virus that was no longer circulating, global health organizations prioritized building infrastructure and systems to respond to future outbreaks. Lessons learned from SARS contributed to the development of platforms and strategies that could be rapidly adapted for emerging pathogens, as seen with the COVID-19 pandemic. This shift in focus ensured that the global health community was better prepared for the next outbreak, rather than investing in a vaccine for a contained threat.
In summary, the reasons a SARS vaccine was not deployed in 2003 include the rapid containment of the outbreak, the complexities and risks of vaccine development, the unpredictability of SARS re-emergence, economic and logistical barriers, and a strategic shift toward preparedness for future pandemics. These factors collectively contributed to the decision to prioritize other health challenges over the deployment of a SARS vaccine.
NBA Players and Vaccination: Who Hasn't Received the COVID-19 Shot?
You may want to see also
Frequently asked questions
No, there was no vaccine developed and approved for SARS (Severe Acute Respiratory Syndrome) during the 2003 outbreak.
The SARS outbreak was contained relatively quickly through public health measures, reducing the urgency for vaccine development. Additionally, the virus disappeared from human populations before a vaccine could be fully developed and tested.
Yes, research efforts began during the outbreak, and several vaccine candidates were in early stages of development. However, none progressed to clinical trials or approval due to the decline in SARS cases.
Yes, the experience with SARS informed strategies for developing vaccines for other coronaviruses, such as MERS and later COVID-19, emphasizing the importance of rapid response and preparedness.
No, there is still no approved vaccine for SARS, as the virus has not re-emerged since 2004. However, research on SARS vaccines contributed to advancements in coronavirus vaccine technology.