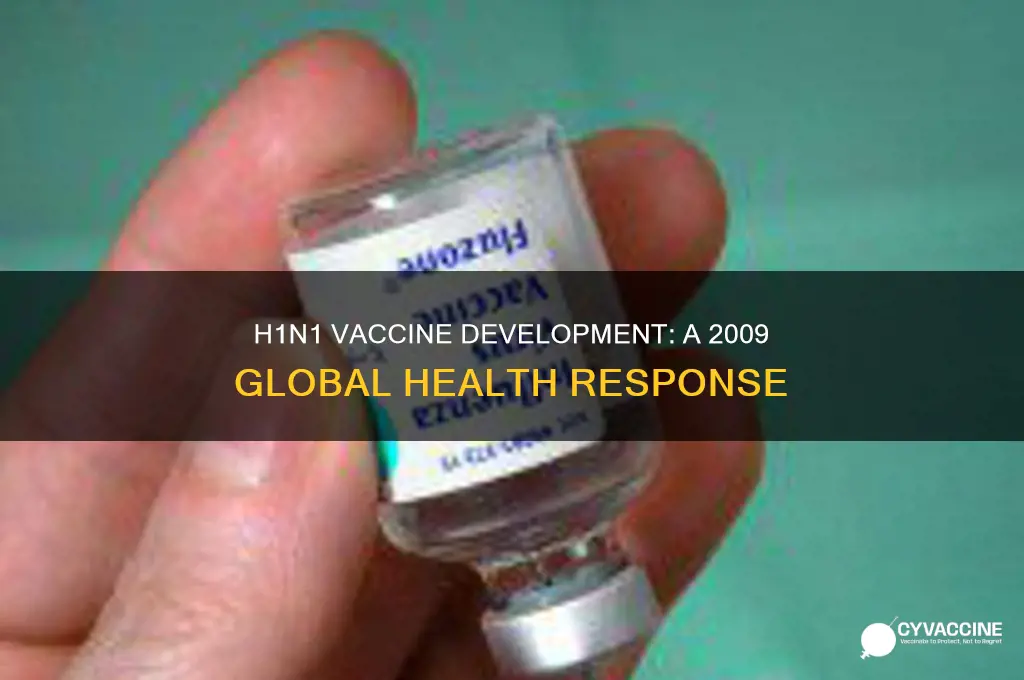
The 2009 H1N1 influenza pandemic, often referred to as the swine flu, emerged as a global health crisis, prompting an urgent need for effective prevention measures. Amid widespread concern and rapid transmission, the development of a vaccine became a critical priority for health authorities worldwide. By the latter half of 2009, several countries had successfully produced and begun distributing H1N1 vaccines, aiming to curb the pandemic's spread and protect vulnerable populations. This swift response highlighted the advancements in vaccine technology and international collaboration, though challenges in distribution and public hesitancy also underscored the complexities of managing a global health emergency.
| Characteristics | Values |
|---|---|
| Existence of H1N1 Vaccine in 2009 | Yes, vaccines were developed and deployed in response to the pandemic. |
| First Vaccine Approval | October 2009 (U.S. FDA approved multiple vaccines). |
| Vaccine Types | Inactivated influenza vaccines, live attenuated influenza vaccine. |
| Global Distribution | Over 80 countries received vaccines through WHO initiatives. |
| Vaccine Effectiveness | 70-90% effectiveness in preventing H1N1 infection. |
| Target Population | Initially prioritized for high-risk groups (pregnant women, healthcare workers, children). |
| Manufacturers | Sanofi Pasteur, GlaxoSmithKline, Novartis, CSL, others. |
| Dose Requirements | Typically 1-2 doses depending on age and prior immunity. |
| Adverse Effects | Mild (soreness, fever) to rare severe cases (e.g., Guillain-Barré syndrome). |
| Global Vaccination Coverage | Over 300 million doses administered worldwide by 2010. |
| Pandemic End Declaration | August 2010 (WHO declared post-pandemic phase). |
Explore related products






What You'll Learn
- Development Timeline: How quickly was the H1N1 vaccine developed and approved in 2009
- Global Distribution: Which countries received the H1N1 vaccine first and why
- Vaccine Effectiveness: How effective was the 2009 H1N1 vaccine in preventing infections
- Public Hesitancy: What were the main reasons for vaccine hesitancy during the H1N1 pandemic
- Side Effects: Were there significant side effects reported from the 2009 H1N1 vaccine
![]()
Development Timeline: How quickly was the H1N1 vaccine developed and approved in 2009?
The development and approval of the H1N1 vaccine in 2009 were marked by an unprecedented speed and global collaboration, driven by the urgent need to address the rapidly spreading pandemic. The H1N1 virus, also known as swine flu, was first detected in April 2009, and by June, the World Health Organization (WHO) had declared it a pandemic. This declaration triggered an immediate response from health authorities, pharmaceutical companies, and regulatory bodies to develop a vaccine as quickly as possible. The timeline for the H1N1 vaccine development began with the isolation of the virus strain, which was completed within weeks of the outbreak. By mid-May 2009, the Centers for Disease Control and Prevention (CDC) and WHO had shared the virus samples with manufacturers, enabling them to start the vaccine production process.
The next critical phase involved the development of vaccine candidates. Manufacturers utilized established influenza vaccine production methods, including egg-based and cell-based technologies, to create H1N1-specific vaccines. Clinical trials began in July 2009, with thousands of volunteers participating in studies to assess the vaccine's safety and efficacy. These trials were conducted in multiple countries simultaneously, ensuring a diverse dataset and expediting the process. The results showed that the vaccine was safe and effective, producing a robust immune response similar to that of seasonal flu vaccines. This rapid progression from virus isolation to clinical trials was made possible by leveraging existing infrastructure and knowledge from seasonal flu vaccine development.
Regulatory approval followed swiftly after the completion of clinical trials. In the United States, the Food and Drug Administration (FDA) granted approval for the H1N1 vaccine in September 2009, just five months after the virus was first identified. Similarly, the European Medicines Agency (EMA) and other regulatory bodies worldwide approved the vaccine within a comparable timeframe. This expedited approval process was facilitated by emergency protocols and continuous communication between manufacturers and regulators. The FDA, for instance, utilized its Emergency Use Authorization (EUA) mechanism to accelerate the availability of the vaccine while ensuring safety and efficacy standards were met.
Mass production and distribution of the H1N1 vaccine began immediately after regulatory approvals. By early October 2009, the first doses were being administered in high-risk populations, including healthcare workers, pregnant women, and individuals with underlying health conditions. The global production capacity was scaled up rapidly, with manufacturers producing millions of doses weekly. This effort was supported by governments and international organizations, which funded vaccine procurement and distribution programs. Despite logistical challenges, such as prioritizing populations and managing supply chains, the vaccine rollout was one of the fastest in history.
In summary, the H1N1 vaccine was developed and approved in an astonishingly short timeframe, from virus identification in April 2009 to widespread vaccination by October 2009. This achievement was the result of global cooperation, the use of existing vaccine technologies, expedited clinical trials, and streamlined regulatory processes. The H1N1 pandemic response set a benchmark for how quickly vaccines could be developed and deployed during a public health emergency, lessons that would later prove invaluable during the COVID-19 pandemic.
Immune System's Defense: Responding to Vaccine Toxins and Ensuring Safety
You may want to see also
Explore related products






![]()
Global Distribution: Which countries received the H1N1 vaccine first and why?
The distribution of the H1N1 vaccine in 2009 was a complex process influenced by global health priorities, manufacturing capacities, and strategic planning. When the H1N1 pandemic was declared by the World Health Organization (WHO) in June 2009, efforts to develop a vaccine began immediately. By September 2009, several countries had secured vaccine supplies, but the initial distribution was not uniform. Wealthier nations, particularly those with advanced healthcare systems and pre-existing contracts with vaccine manufacturers, were among the first to receive doses. The United States, for example, began administering the H1N1 vaccine in early October 2009, prioritizing high-risk groups such as healthcare workers, pregnant women, and young children. This early access was largely due to the country's ability to invest in vaccine development and secure large orders from manufacturers.
European countries also played a significant role in the initial distribution of the H1N1 vaccine. Nations like the United Kingdom, France, and Germany started vaccination campaigns in late 2009, focusing on vulnerable populations. These countries had the financial resources and infrastructure to negotiate early delivery schedules with pharmaceutical companies. Additionally, the European Medicines Agency (EMA) expedited the approval process for the H1N1 vaccine, enabling quicker distribution across the continent. Australia and Canada were other early recipients, with both countries launching vaccination programs in October 2009. Their success was attributed to strong public health systems and proactive government responses to the pandemic.
In contrast, many low- and middle-income countries faced significant delays in accessing the H1N1 vaccine. The WHO coordinated efforts to ensure equitable distribution through the Pandemic Influenza Preparedness (PIP) Framework, but initial supplies were limited. Wealthier nations had already secured the majority of available doses through advance purchase agreements, leaving fewer options for developing countries. For instance, many African and Southeast Asian nations did not begin receiving substantial vaccine supplies until early 2010. This disparity highlighted the challenges of global vaccine equity during a pandemic.
The prioritization of certain countries in the initial distribution was driven by several factors. Firstly, nations with the financial means to invest in vaccine development and procurement naturally gained early access. Secondly, countries with robust healthcare systems were better equipped to handle the logistics of mass vaccination campaigns. Lastly, strategic considerations, such as protecting global travel hubs and densely populated areas, influenced distribution decisions. The WHO and other international organizations worked to address these imbalances, but the early phase of H1N1 vaccine distribution underscored the need for more equitable global health strategies.
Efforts to improve global access to the H1N1 vaccine gained momentum in 2010. The WHO facilitated donations from wealthier countries and collaborated with manufacturers to increase production. Initiatives like the Advance Market Commitment (AMC) aimed to incentivize vaccine production for developing nations. Despite these efforts, the initial distribution disparities remained a critical lesson for future pandemic responses. The H1N1 vaccine rollout in 2009 demonstrated that global health security requires not only rapid vaccine development but also fair and inclusive distribution mechanisms.
Super Bowl LVI: Vaccination Status of Attendees
You may want to see also
Explore related products




$15.95


![]()
Vaccine Effectiveness: How effective was the 2009 H1N1 vaccine in preventing infections?
The 2009 H1N1 influenza pandemic, often referred to as the swine flu, prompted a rapid global response to develop and distribute a vaccine. By late 2009, several H1N1 vaccines were authorized for use, marking a significant milestone in pandemic control efforts. The effectiveness of these vaccines in preventing infections was a critical question for public health officials and the general population. Studies conducted during and after the pandemic provided valuable insights into how well the vaccine worked in real-world scenarios.
Clinical trials and observational studies consistently showed that the 2009 H1N1 vaccine was highly effective in preventing infections. The vaccine’s efficacy ranged from 70% to 90% in healthy adults, depending on the population and the specific vaccine formulation used. This effectiveness was comparable to that of seasonal influenza vaccines, which typically range from 40% to 60% in efficacy. The higher effectiveness of the H1N1 vaccine was partly due to the novelty of the virus strain, as most individuals had no pre-existing immunity, allowing the vaccine to elicit a robust immune response.
However, vaccine effectiveness varied across different age groups and populations. In children and young adults, the vaccine was particularly effective, with studies showing protection rates above 80%. In contrast, older adults, especially those over 65, experienced slightly lower effectiveness, likely due to age-related immune system changes. Pregnant women, a high-risk group during the pandemic, also benefited significantly from the vaccine, with studies demonstrating reduced infection rates and severe outcomes in vaccinated individuals.
One of the challenges in assessing vaccine effectiveness was the timing of vaccination relative to the pandemic’s peak. In some regions, vaccine distribution began after the initial wave of infections had already subsided, limiting the vaccine’s overall impact on infection rates. Despite this, the vaccine played a crucial role in preventing a second wave of infections and reducing the burden on healthcare systems. Post-vaccination surveillance data confirmed that vaccinated individuals were substantially less likely to contract H1N1 compared to unvaccinated individuals.
In conclusion, the 2009 H1N1 vaccine was a highly effective tool in preventing infections during the pandemic. Its success underscored the importance of rapid vaccine development and distribution in controlling emerging infectious diseases. While effectiveness varied across populations, the vaccine’s overall impact was undeniable, saving lives and mitigating the pandemic’s severity. The lessons learned from the H1N1 vaccine continue to inform global strategies for pandemic preparedness and response.
Should You Apply Ice to Your Vaccine Site? Expert Advice
You may want to see also
Explore related products



![Pandemic [DVD]](https://m.media-amazon.com/images/I/51vChb09XaL._AC_UL320_.jpg)

![]()
Public Hesitancy: What were the main reasons for vaccine hesitancy during the H1N1 pandemic?
The 2009 H1N1 pandemic, often referred to as the swine flu pandemic, saw the rapid development and distribution of vaccines to combat the spread of the virus. Despite the availability of these vaccines, public hesitancy posed a significant challenge to vaccination efforts. One of the primary reasons for vaccine hesitancy during this period was mistrust in the rapid development and approval of the vaccine. Many people were skeptical about the safety and efficacy of a vaccine that was developed and approved in a relatively short timeframe. This skepticism was fueled by concerns that corners may have been cut during the testing and approval process, potentially compromising the vaccine's safety.
Another major factor contributing to hesitancy was misinformation and conspiracy theories. The rise of social media and the internet allowed false information about the H1N1 vaccine to spread rapidly. Claims that the vaccine was part of a government plot, contained harmful ingredients like mercury, or caused severe side effects, including neurological disorders, were widespread. These unfounded fears eroded public confidence in the vaccine, leading many to avoid vaccination altogether. Public health officials struggled to counteract this misinformation effectively, as it often resonated more strongly with people than evidence-based messaging.
Previous vaccine controversies also played a role in shaping public attitudes during the H1N1 pandemic. For instance, debates surrounding the safety of vaccines, such as those related to autism (a debunked claim), had already sown seeds of doubt in some communities. This pre-existing skepticism made it easier for individuals to question the H1N1 vaccine's safety and necessity. Additionally, historical instances of medical mistrust, particularly among marginalized communities, further exacerbated hesitancy, as these groups often had valid reasons to be wary of government-led health initiatives.
A lack of perceived risk from the H1N1 virus itself was another reason for vaccine hesitancy. Many people believed that the pandemic was overhyped by the media and that the virus was no more dangerous than seasonal flu. This perception of low risk led individuals to question the need for vaccination, especially when weighed against potential (albeit unfounded) risks associated with the vaccine. Public health messaging often struggled to communicate the actual risks of H1N1 effectively, particularly among younger, healthier populations who felt less vulnerable.
Finally, logistical and accessibility issues contributed to hesitancy in some regions. In certain areas, vaccine distribution was uneven, and access was limited, particularly for underserved populations. This lack of accessibility reinforced the perception that the vaccine was not a priority or was being unfairly allocated. Additionally, some individuals were deterred by the requirement for multiple doses or by concerns about out-of-pocket costs, even though many vaccination programs were offered free of charge. These practical barriers, combined with the aforementioned factors, created a complex landscape of hesitancy that public health officials had to navigate during the H1N1 pandemic.
MMR Vaccines: Protecting Babies Through Moms
You may want to see also
Explore related products


![Pandemic [DVD]](https://m.media-amazon.com/images/I/81G1z+AOoNL._AC_UL320_.jpg)
![Pandemic Pandemic [DVD]](https://m.media-amazon.com/images/I/81dZDU9gUpL._AC_UL320_.jpg)

![Pandemic [DVD] [UK Import]](https://m.media-amazon.com/images/I/61az7jpPZ+L._AC_UL320_.jpg)
![]()
Side Effects: Were there significant side effects reported from the 2009 H1N1 vaccine?
The 2009 H1N1 influenza pandemic prompted a rapid global response, including the development and distribution of vaccines to curb the spread of the virus. As with any vaccine, concerns about potential side effects were closely monitored by health authorities. The H1N1 vaccine, which became available in late 2009, was administered to millions of people worldwide. While vaccines are rigorously tested for safety, real-world use can sometimes reveal additional insights into side effects. The majority of reported side effects from the 2009 H1N1 vaccine were mild and similar to those associated with seasonal flu vaccines, such as soreness at the injection site, mild fever, and fatigue. These symptoms were generally short-lived and resolved without medical intervention.
One of the most scrutinized aspects of the H1N1 vaccine was its association with rare but serious side effects. One such concern was the potential link to Guillain-Barré syndrome (GBS), a rare neurological disorder that can cause muscle weakness and, in severe cases, paralysis. Historical data from the 1976 swine flu vaccination campaign had shown a small increased risk of GBS, raising questions about the 2009 vaccine. However, studies conducted during and after the 2009 pandemic found that the risk of GBS from the H1N1 vaccine was extremely low, estimated at approximately 1 to 2 additional cases per million vaccinated individuals. This risk was considered minimal compared to the benefits of vaccination in preventing severe illness and death from H1N1.
Another area of focus was the use of adjuvants in some versions of the H1N1 vaccine, particularly in Europe. Adjuvants are substances added to vaccines to enhance the immune response, allowing for the use of smaller amounts of antigen. While adjuvanted vaccines were deemed safe by regulatory agencies, some individuals reported localized reactions, such as redness, swelling, and pain at the injection site. Systemic reactions, including headache, muscle pain, and fatigue, were also noted but were generally mild and transient. No significant long-term adverse effects were attributed to the use of adjuvants in the H1N1 vaccine.
Post-vaccination surveillance systems played a crucial role in monitoring side effects. In the United States, the Vaccine Adverse Event Reporting System (VAERS) and the Vaccine Safety Datalink (VSD) were used to track adverse events following H1N1 vaccination. These systems identified a small number of serious adverse events, such as severe allergic reactions (anaphylaxis), but these occurred at rates comparable to those seen with seasonal flu vaccines. The overall safety profile of the H1N1 vaccine was consistent with that of other influenza vaccines, reinforcing public health confidence in its use.
In conclusion, while no medical intervention is entirely without risk, the 2009 H1N1 vaccine was found to have a favorable safety profile. The reported side effects were predominantly mild and transient, with rare serious events occurring at very low rates. The benefits of vaccination in preventing H1N1-related morbidity and mortality far outweighed the minimal risks associated with the vaccine. The experience with the 2009 H1N1 vaccine provided valuable lessons for future pandemic responses, emphasizing the importance of robust surveillance and transparent communication about vaccine safety.
Louisiana's Vaccine Laws: Your Rights and Legal Obligations for Children
You may want to see also
Frequently asked questions
Yes, a vaccine for the H1N1 influenza virus, commonly known as the swine flu, was developed and distributed globally in 2009.
The H1N1 vaccine became available in the United States and other countries in October 2009, following its approval by health authorities.
The 2009 H1N1 vaccine was highly effective in preventing infection and reducing the severity of symptoms in those who contracted the virus. Studies showed it provided strong immunity in most recipients.
Priority groups for the H1N1 vaccine included pregnant women, healthcare workers, children and young adults, and individuals with underlying health conditions, as they were at higher risk of severe complications.
The 2009 H1N1 vaccine had side effects similar to those of seasonal flu vaccines, such as soreness at the injection site, mild fever, and fatigue. Serious adverse reactions were rare.



![PANDEMIC [Blu-ray]](https://m.media-amazon.com/images/I/71xlZkgPU4L._AC_UL320_.jpg)





![Pandemic [Blu-ray]](https://m.media-amazon.com/images/I/61EbhmkB1tS._AC_UL320_.jpg)
![Pandemic [ NON-USA FORMAT, PAL, Reg.2 Import - Netherlands ]](https://m.media-amazon.com/images/I/51diyJBw2mS._AC_UL320_.jpg)