The question of whether polio was already on the decline before the introduction of the vaccine in 1955 is a topic of historical and epidemiological interest. While some argue that improved sanitation, hygiene, and living conditions may have contributed to a natural decrease in polio cases, evidence suggests that the disease remained a significant public health threat in the early 20th century. Polio outbreaks were frequent, causing widespread fear and disability, particularly among children. The development and widespread distribution of the polio vaccine, pioneered by Jonas Salk and later enhanced by Albert Sabin, played a pivotal role in drastically reducing the incidence of the disease. However, examining pre-vaccine trends and societal changes provides valuable context for understanding the full impact of vaccination efforts on polio eradication.
| Characteristics | Values |
|---|---|
| Trend Before Vaccine (1950s) | Polio cases were not consistently declining before the vaccine. Data shows fluctuations, with some years having higher incidence than others. |
| Sanitation & Hygiene Improvements | Improved sanitation and hygiene practices likely contributed to a gradual reduction in some regions, but this was not universal and did not eliminate the disease. |
| Seasonal Patterns | Polio exhibited seasonal peaks, typically in summer months, which remained consistent before vaccination. |
| Global Incidence | Polio was endemic worldwide before the vaccine, affecting millions annually, particularly children. |
| Mortality Rate | While survival rates improved slightly due to better medical care, mortality remained significant, especially in severe cases. |
| Impact of Vaccine Introduction | The introduction of the polio vaccine in the mid-1950s led to a dramatic and sustained decline in cases globally, ultimately leading to near eradication in most countries. |
| Conclusion | Polio was not on a consistent decline before the vaccine. The vaccine was the primary factor in reducing and nearly eradicating the disease. |
Explore related products






What You'll Learn
![]()
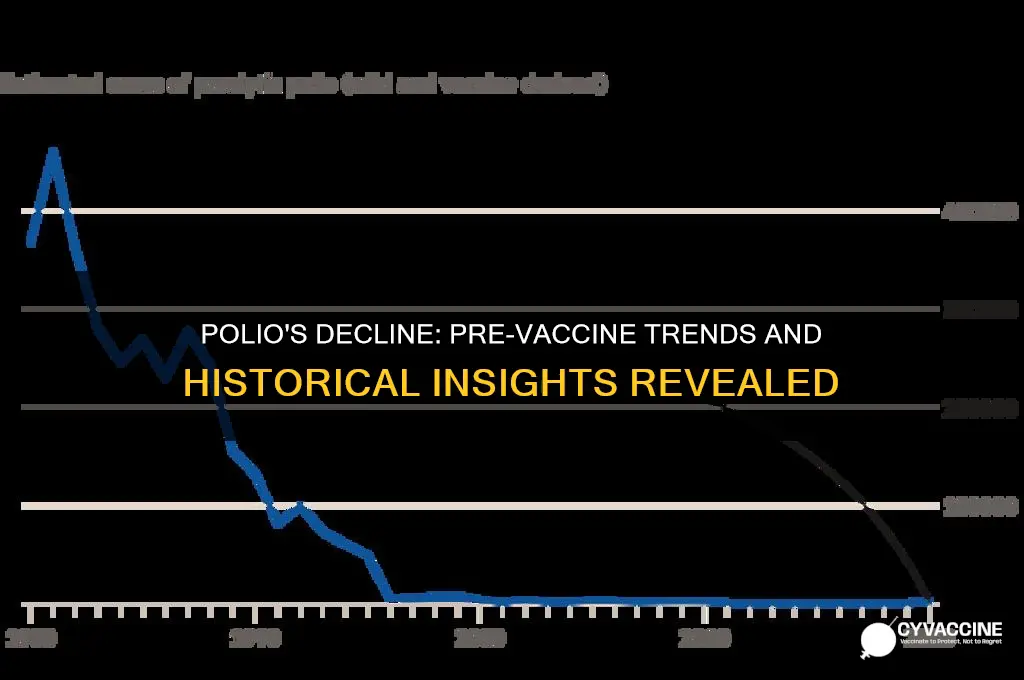
Historical Polio Incidence Trends
The historical incidence of polio, a devastating viral disease, has been a subject of significant interest, particularly in the context of the introduction of the polio vaccine in the mid-20th century. Before the vaccine became widely available in the 1950s, polio outbreaks were a recurring public health crisis, especially in industrialized countries. The disease primarily affected young children, causing paralysis and, in severe cases, death. Historical data from the United States, the United Kingdom, and other developed nations show that polio incidence was highly seasonal, with peaks during the summer months, earning it the moniker "summer plague." However, the question of whether polio was already on the decline before the vaccine’s introduction has sparked considerable debate among historians and epidemiologists.
Examination of polio incidence trends in the early to mid-20th century reveals a complex pattern. In the United States, for instance, polio cases began to be systematically recorded in the late 19th century, with major epidemics occurring in the early 1900s. By the 1940s and early 1950s, some data suggest a slight decrease in the number of reported cases. For example, the annual incidence rate in the U.S. dropped from a peak of around 25 cases per 100,000 population in the late 1940s to approximately 15 cases per 100,000 by 1952. Similar trends were observed in other countries, such as Sweden and Denmark, where polio cases appeared to plateau or marginally decline before the vaccine era. These observations have led some researchers to argue that improved sanitation, hygiene, and living conditions may have contributed to a natural decline in polio transmission.
However, the interpretation of these trends is not without controversy. Critics argue that the apparent decline in polio cases before the vaccine could be attributed to changes in reporting practices, diagnostic criteria, or public awareness rather than a true reduction in incidence. For example, the introduction of more accurate diagnostic tools in the mid-20th century may have led to underreporting of milder cases in earlier decades. Additionally, the cyclical nature of polio outbreaks, with periodic peaks and troughs, makes it challenging to discern a clear downward trend without long-term, standardized data. Furthermore, while sanitation improvements may have reduced exposure to the poliovirus, the virus remained endemic, and the risk of large-scale outbreaks persisted until the vaccine was introduced.
The introduction of the inactivated polio vaccine (IPV) by Jonas Salk in 1955 and the oral polio vaccine (OPV) by Albert Sabin in 1961 marked a turning point in the fight against the disease. Following widespread vaccination campaigns, polio incidence plummeted dramatically. In the United States, for example, annual cases dropped from over 20,000 in the early 1950s to fewer than 100 by the mid-1960s. This rapid decline strongly suggests that the vaccine played a pivotal role in controlling the disease, rather than a pre-existing downward trend. Similar results were observed globally, with many countries experiencing a sharp reduction in polio cases within a few years of vaccine introduction.
In conclusion, while there is evidence of a slight decline in polio incidence in some regions before the vaccine era, the data are ambiguous and subject to various interpretations. Factors such as improved sanitation, changes in reporting, and the cyclical nature of outbreaks complicate efforts to attribute the decline solely to non-vaccine factors. The dramatic reduction in polio cases following vaccination campaigns underscores the critical role of immunization in controlling the disease. Thus, while pre-vaccine trends may have shown modest improvements, the polio vaccine remains the decisive factor in the near-eradication of this once-feared disease.
Vaccination Requirements for Visiting New Orleans
You may want to see also
![]()
Sanitation Improvements Impact
The role of sanitation improvements in the decline of polio cases before the advent of the vaccine is a critical aspect of understanding the disease's history. Polio, a highly infectious viral disease, thrives in areas with poor hygiene and sanitation. In the early 20th century, many developed countries began implementing significant sanitation reforms, which had a profound impact on public health. These improvements included the development of modern sewage systems, clean water supplies, and better waste management practices. As a result, the transmission of various waterborne and fecal-oral diseases, including polio, was significantly reduced. This period marked a turning point in the battle against infectious diseases, setting the stage for a decline in polio cases even before the vaccine became widely available.
Sanitation Infrastructure Development: The construction of comprehensive sewage systems in urban areas played a pivotal role in breaking the chain of polio transmission. Before these advancements, human waste often contaminated water sources, providing an ideal environment for the poliovirus to spread. By separating wastewater from clean water supplies, the risk of infection decreased dramatically. This was particularly evident in cities where sanitation projects were prioritized, leading to a noticeable drop in polio incidence rates. The impact of such infrastructure improvements cannot be overstated, as they directly targeted the primary routes of polio transmission.
Clean Water Initiatives: Access to clean drinking water is another critical factor in the decline of polio. Many countries launched campaigns to ensure safe water supplies for their populations, which involved treating water to eliminate pathogens, including the poliovirus. This was achieved through chlorination, filtration, and other purification methods. As clean water became more accessible, the oral-fecal route of polio transmission was disrupted, contributing to a decrease in new infections. The correlation between improved water quality and reduced polio cases is well-documented, highlighting the importance of sanitation in disease prevention.
Public Health Education and Hygiene Practices: Sanitation improvements were often accompanied by public health campaigns promoting better personal hygiene. Educating communities about the importance of handwashing, proper waste disposal, and food hygiene further reduced the spread of polio. These measures empowered individuals to take an active role in protecting themselves and their families from the disease. The combined effect of improved sanitation infrastructure and heightened public awareness created an environment less conducive to polio transmission, thereby accelerating its decline.
The impact of sanitation improvements on polio cannot be viewed in isolation, as these advancements also contributed to the overall reduction of various other infectious diseases. This multi-faceted approach to public health laid the groundwork for the successful introduction of the polio vaccine, which ultimately led to the near eradication of the disease. Understanding the historical context and the role of sanitation provides valuable insights into the complex interplay between public health measures and disease control. It serves as a reminder that comprehensive strategies, addressing both environmental and individual factors, are essential in the fight against infectious diseases.
Yellow Fever Vaccine: Essential for Kenya Travel?
You may want to see also
![]()
Pre-Vaccine Medical Interventions
Before the introduction of the polio vaccine in the mid-20th century, medical interventions to combat the disease were limited and primarily focused on managing symptoms and preventing complications. Polio, caused by the poliovirus, often resulted in paralysis, respiratory failure, and death, particularly among children. In the absence of a cure or vaccine, healthcare systems relied on a combination of isolation, supportive care, and experimental treatments to address the growing public health crisis. These pre-vaccine interventions were reactive rather than preventive, and their effectiveness varied widely.
One of the earliest and most widespread interventions was the use of iron lung machines to assist patients with respiratory paralysis. Polio often affected the muscles responsible for breathing, leading to acute respiratory distress. The iron lung, a large, tank-like device, used negative pressure to facilitate breathing in paralyzed patients. While it saved countless lives, it was a temporary solution and did not address the underlying viral infection. Hospitals and clinics invested heavily in these machines during polio outbreaks, but their use was cumbersome and required constant medical supervision.
Another key pre-vaccine intervention was physical therapy to manage muscle weakness and paralysis. Therapists employed exercises, massages, and splints to prevent deformities and maintain muscle function in affected individuals. This approach aimed to improve patients' quality of life and mobility, but it was not a cure. Physical therapy became a cornerstone of polio aftercare, particularly for survivors left with long-term disabilities. However, its success depended on the severity of the infection and the timing of intervention.
Isolation and quarantine measures were also implemented to control the spread of polio. Public health officials closed schools, swimming pools, and other public spaces during outbreaks to limit exposure, especially during the summer months when cases peaked. While these measures reduced transmission to some extent, they were disruptive and economically burdensome. Additionally, they did not address the root cause of the disease, and polio continued to resurge periodically.
Experimental treatments, such as antibiotics, blood transfusions, and even surgery, were occasionally used to combat polio, though their efficacy was unproven. Antibiotics, for example, were ineffective against the virus but were sometimes prescribed to prevent secondary bacterial infections. Similarly, surgeries like tendon releases were performed to alleviate muscle contractures, but these procedures were invasive and not universally successful. These interventions highlighted the desperation of the medical community in the face of a devastating and incurable disease.
In conclusion, pre-vaccine medical interventions for polio were largely symptomatic and focused on managing complications rather than eradicating the virus. While innovations like the iron lung and physical therapy provided critical support to patients, they did not halt the disease's spread or reduce its incidence. The decline in polio cases observed in some regions before the vaccine's introduction is often attributed to improved sanitation, hygiene, and public health measures rather than medical treatments. The development of the polio vaccine in the 1950s marked a turning point, offering a proactive and effective solution to a disease that had long evaded control.
Is Hepatitis A Vaccine Included in Childhood Immunization Schedules?
You may want to see also
![]()
Diagnostic Criteria Changes
The question of whether polio was on the decline before the introduction of the vaccine is a complex one, and it involves examining various factors, including diagnostic criteria changes. In the early 20th century, the diagnosis of polio was primarily based on clinical symptoms, such as paralysis, muscle weakness, and meningitis. However, as medical understanding evolved, so did the diagnostic criteria for polio. This evolution in criteria played a significant role in shaping the perceived incidence and prevalence of the disease.
One major change in diagnostic criteria occurred in the 1950s, around the time the polio vaccine was being developed. Prior to this, the diagnosis of polio was often made based on a combination of clinical symptoms and laboratory tests, such as the detection of poliovirus in stool samples or cerebrospinal fluid. However, in 1954, the World Health Organization (WHO) introduced new diagnostic criteria that narrowed the definition of polio. Under these new criteria, a case of polio required not only the presence of clinical symptoms but also laboratory confirmation of poliovirus infection. This change effectively excluded many cases that would have previously been classified as polio, leading to a apparent decline in reported cases.
The impact of these diagnostic criteria changes on the perceived incidence of polio cannot be overstated. By narrowing the definition of the disease, the number of reported cases decreased significantly, even if the actual number of individuals experiencing poliovirus infection remained constant. This phenomenon, known as "diagnostic substitution," can create the illusion of a decline in disease incidence, when in reality, the decline is largely due to changes in diagnostic practices. In the case of polio, this shift in diagnostic criteria coincided with the introduction of the vaccine, making it difficult to disentangle the effects of the vaccine from the effects of diagnostic changes on the observed decline in cases.
Furthermore, the diagnostic criteria changes also affected the classification of non-paralytic polio cases. Before the 1950s, many individuals with mild or asymptomatic poliovirus infections would have been classified as having non-paralytic polio. However, under the new criteria, these cases were often reclassified as aseptic meningitis or other non-polio conditions. This reclassification further contributed to the apparent decline in polio cases, as many individuals who would have previously been counted as polio cases were now being diagnosed with other conditions. As a result, it is essential to consider these diagnostic criteria changes when evaluating the historical trends in polio incidence and assessing the impact of the vaccine on disease decline.
In addition to the WHO's diagnostic criteria changes, there were also variations in diagnostic practices across different regions and countries. Some areas may have had more stringent diagnostic criteria, requiring more extensive laboratory testing or more severe clinical symptoms for a confirmed polio diagnosis. These regional differences in diagnostic practices can further complicate the interpretation of historical polio data and make it challenging to compare trends across different locations. To accurately assess the decline of polio before the vaccine, it is crucial to account for these regional variations in diagnostic criteria and practices, as well as the broader changes in diagnostic standards over time.
Lastly, the diagnostic criteria changes highlight the importance of considering the social and historical context in which disease trends are observed. The introduction of new diagnostic criteria, changes in surveillance systems, and shifts in public health priorities can all influence the perceived incidence of a disease. In the case of polio, the diagnostic criteria changes coincided with a period of intense public health efforts to eradicate the disease, including the development and distribution of the vaccine. While the vaccine undoubtedly played a significant role in reducing polio incidence, it is essential to recognize the complex interplay between diagnostic criteria changes, public health interventions, and disease trends when evaluating the historical decline of polio. By carefully considering these factors, researchers can gain a more nuanced understanding of the decline of polio before the vaccine and the multifaceted efforts that contributed to its eventual eradication.
Proving Teacher Status for Vaccine Access: A Step-by-Step Guide
You may want to see also
![]()
Socioeconomic Factors Influence
The role of socioeconomic factors in the decline of polio before the vaccine is a critical aspect often overshadowed by the medical breakthrough of vaccination. Improved sanitation and hygiene practices played a significant role in reducing the transmission of the poliovirus. In the early 20th century, many developed countries began investing in better sewage systems, clean water supplies, and public health education. These advancements minimized the presence of the virus in the environment, thereby decreasing the likelihood of infection, especially in urban areas. For instance, the implementation of chlorination in drinking water and the construction of modern sewage treatment plants in the United States during the 1930s and 1940s significantly curtailed waterborne transmission of the disease.
Economic development and urbanization also contributed to the decline of polio. As societies became more affluent, living conditions improved, reducing overcrowding and improving access to healthcare. Urbanization, while initially linked to higher disease rates due to close living quarters, eventually led to better infrastructure and public health measures. In contrast, rural areas often lacked these advancements, making them more susceptible to outbreaks. The disparity highlights how socioeconomic progress in urban centers inadvertently contributed to the overall decline in polio cases before the vaccine became widely available.
Education and public health campaigns were another critical socioeconomic factor. As literacy rates increased, so did the public's understanding of disease prevention. Governments and health organizations launched campaigns promoting personal hygiene, such as handwashing and proper waste disposal, which further reduced the spread of the virus. These initiatives were particularly effective in middle- and high-income countries, where resources were available to disseminate information and enforce health standards. The combination of education and improved public health measures created a societal shift toward better hygiene practices, which played a pivotal role in decreasing polio incidence.
Occupational changes and labor policies also influenced polio's decline. The shift from agrarian to industrial economies reduced exposure to the virus in certain populations. Industrial jobs often provided better working conditions and access to healthcare, while labor laws mandated cleaner environments and shorter working hours, indirectly supporting health improvements. Additionally, the rise of the middle class meant that more families could afford medical care and were less likely to live in conditions conducive to disease spread. These socioeconomic shifts collectively created an environment less favorable for polio transmission.
Lastly, the impact of socioeconomic inequality cannot be overlooked. While polio was declining in wealthier nations, it remained prevalent in poorer regions with limited access to clean water, sanitation, and healthcare. This disparity underscores how socioeconomic factors were not uniformly beneficial across the globe. The decline in polio before the vaccine was thus a phenomenon largely confined to countries with the resources to implement widespread public health improvements. Understanding this context is essential for appreciating the multifaceted nature of disease control and the limitations of socioeconomic progress in addressing global health challenges.
Understanding the Multiple Phases of Vaccine Testing and Development
You may want to see also
Frequently asked questions
Yes, polio incidence was already declining in many countries before the vaccine was widely used, due to improved sanitation, hygiene, and reporting methods.
Better public health measures, such as cleaner water supplies, improved sewage systems, and increased awareness of hygiene, played a significant role in reducing polio cases.
No, polio remained a significant threat despite the decline, as outbreaks still occurred, and the virus could spread rapidly in susceptible populations.
The polio vaccine accelerated the decline of the disease, leading to its near eradication globally, whereas the pre-vaccine decline was slower and less consistent.
Yes, some skeptics initially questioned the need for the vaccine, but the dramatic reduction in cases post-vaccination proved its critical importance in controlling the disease.