Guillain-Barré syndrome (GBS), a rare neurological disorder causing muscle weakness and sometimes paralysis, has been documented long before the advent of modern vaccinations. Historically, GBS has been associated with various infections, particularly those caused by Campylobacter jejuni, influenza, and other pathogens. While vaccines, such as the 1976 swine flu vaccine, have been linked to a slight increase in GBS cases, the incidence remains extremely low compared to the risks posed by the diseases the vaccines prevent. The question of whether GBS was a significant problem prior to vaccinations is complex, as its rarity and underreporting in earlier medical records make it difficult to establish a clear baseline. However, evidence suggests that GBS has always existed, with infections being the primary trigger, and vaccines have not fundamentally altered its overall prevalence.
| Characteristics | Values |
|---|---|
| Pre-Vaccination Incidence | Guillain-Barré Syndrome (GBS) was recognized as a rare neurological disorder prior to widespread vaccination programs. It has been documented in medical literature since the late 19th century. |
| Annual Incidence Rate | Approximately 1-2 cases per 100,000 people annually, regardless of vaccination status. |
| Known Triggers (Pre-Vaccination) | Infections such as Campylobacter jejuni, influenza, cytomegalovirus (CMV), and Epstein-Barr virus (EBV) were identified as common triggers. |
| Association with Vaccines | Rare cases of GBS have been temporally associated with certain vaccines (e.g., 1976 swine flu vaccine), but the baseline risk of GBS remained consistent with pre-vaccination rates. |
| Historical Perspective | GBS was described in medical literature long before modern vaccination programs, indicating it was not a new phenomenon. |
| Risk Comparison | The risk of developing GBS from infections (e.g., influenza) is generally higher than the rare risk associated with vaccines. |
| Conclusion | GBS was a recognized medical condition prior to vaccinations, and its incidence has remained relatively stable over time. Vaccines have not been shown to significantly increase the overall risk of GBS beyond baseline rates. |
Explore related products






What You'll Learn
- Historical incidence of Guillain-Barré syndrome before widespread vaccination programs
- Pre-vaccine era Guillain-Barré syndrome diagnosis and reporting accuracy
- Natural causes of Guillain-Barré syndrome unrelated to vaccinations
- Epidemiological data on Guillain-Barré syndrome prior to 1900s
- Comparison of Guillain-Barré syndrome rates before and after vaccine introduction
![]()
Historical incidence of Guillain-Barré syndrome before widespread vaccination programs
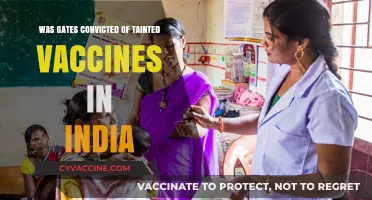
Guillain-Barré syndrome (GBS) is a rare neurological disorder in which the body's immune system mistakenly attacks the peripheral nervous system, leading to muscle weakness, paralysis, and sometimes respiratory failure. Understanding the historical incidence of GBS before widespread vaccination programs is crucial for contextualizing its prevalence and potential causes. Historical records and medical literature from the early 20th century provide insights into the occurrence of GBS prior to the introduction of modern vaccines. The syndrome was first described in detail by Georges Guillain, Jean Alexandre Barré, and André Strohl in 1916, following their observation of two soldiers with ascending paralysis and albuminocytological dissociation in their cerebrospinal fluid. However, retrospective analyses suggest that similar conditions were likely present long before this formal description.
Before the mid-20th century, GBS was considered an extremely rare condition, with only sporadic case reports in medical literature. The lack of widespread diagnostic tools and standardized criteria made it difficult to accurately identify and document cases. However, it is clear that GBS existed prior to the advent of vaccination programs. For instance, some historians and medical researchers speculate that the 1916 description of GBS might have been influenced by a post-infectious complication of Campylobacter jejuni or other pathogens, which are now known to be common triggers of the syndrome. This suggests that GBS was likely associated with natural infections rather than vaccinations during this period.
The incidence of GBS before mass vaccination programs is challenging to quantify due to limited data and underreporting. However, studies from the pre-vaccine era indicate that the annual incidence of GBS was estimated to be around 1 to 2 cases per 100,000 population. This baseline rate is important for comparison with post-vaccination data, as it helps distinguish between the natural occurrence of GBS and any potential vaccine-related increases. Notably, the rarity of GBS in historical populations underscores that it was not a widespread public health concern prior to vaccinations, though it did pose a significant risk to those affected.
One key aspect of pre-vaccination GBS is its association with preceding infections, particularly respiratory or gastrointestinal illnesses. Pathogens such as influenza, cytomegalovirus, and Campylobacter jejuni were recognized as triggers long before vaccines became a focus of discussion. These infections were common in the absence of modern vaccines, and their role in causing GBS highlights the syndrome's infectious etiology. This historical context is essential for understanding that GBS was not a "problem" in the sense of being widespread, but rather a rare complication of natural infections.
In summary, Guillain-Barré syndrome was indeed present before widespread vaccination programs, with a baseline incidence of approximately 1 to 2 cases per 100,000 population annually. Its rarity and association with natural infections indicate that GBS was not a significant public health issue prior to vaccinations. The historical data emphasize that GBS has always been a post-infectious condition, with triggers unrelated to vaccines. This understanding is vital for accurately assessing the risks and benefits of vaccination programs and addressing concerns about vaccine safety.
Vaccine Refusal and Child Neglect Laws in Oklahoma: What Parents Need to Know
You may want to see also
Explore related products




![A History of Violence (The Criterion Collection) [4K UHD]](https://m.media-amazon.com/images/I/71lqpbUFtWL._AC_UY218_.jpg)
![]()
Pre-vaccine era Guillain-Barré syndrome diagnosis and reporting accuracy
In the pre-vaccine era, Guillain-Barré syndrome (GBS) was indeed recognized as a clinical entity, though its diagnosis and reporting accuracy were significantly limited by the medical knowledge and tools available at the time. GBS, first described in 1916 by Georges Guillain, Jean Alexandre, and André Strohl, was initially identified based on clinical observations of acute-onset muscle weakness and areflexia. However, without advanced diagnostic techniques, such as cerebrospinal fluid analysis and electrodiagnostic studies, early cases were often misdiagnosed or underreported. The syndrome’s rarity and the lack of standardized diagnostic criteria further complicated accurate identification, leading to inconsistencies in medical literature and public health records.
The absence of widespread vaccination programs in the early 20th century eliminates the possibility of vaccine-related GBS cases, but it also means that baseline incidence rates were not well-established. Physicians relied heavily on clinical presentation, which could mimic other neurological conditions like poliomyelitis, myasthenia gravis, or botulism. This overlap in symptoms frequently resulted in misclassification, particularly in regions with high poliovirus prevalence. Additionally, the lack of standardized reporting systems and limited global communication hindered the accumulation of reliable epidemiological data, making it difficult to assess the true burden of GBS prior to the vaccine era.
Diagnostic accuracy was further constrained by the unavailability of key laboratory tests. Elevated protein levels in cerebrospinal fluid without pleocytosis, a hallmark of GBS, were not consistently measured until the mid-20th century. Electromyography and nerve conduction studies, essential for confirming demyelinating or axonal subtypes of GBS, were not widely used until the 1950s and 1960s. Without these tools, clinicians often relied on exclusion diagnoses, which were prone to error. This reliance on clinical judgment alone likely led to both overdiagnosis and underdiagnosis, skewing the perceived prevalence of GBS.
Reporting accuracy was also influenced by regional variations in medical infrastructure and awareness. In developed countries with better access to healthcare, GBS cases were more likely to be documented, albeit with varying degrees of precision. In contrast, resource-limited settings often lacked the capacity to diagnose or report such cases, leading to underrepresentation in global health statistics. The absence of a centralized database or international collaboration further exacerbated these discrepancies, making it challenging to draw definitive conclusions about the syndrome’s pre-vaccine prevalence.
Despite these limitations, historical case series and retrospective studies provide valuable insights into the natural history of GBS. Early descriptions highlight the syndrome’s association with antecedent infections, particularly gastrointestinal and respiratory illnesses, which remain established triggers today. These observations underscore the infectious etiology of GBS and suggest that its incidence was likely consistent with background infection rates. However, without rigorous diagnostic and reporting frameworks, the pre-vaccine era data remain insufficient to establish a precise baseline for comparison with post-vaccine periods.
In summary, while Guillain-Barré syndrome was recognized before the advent of vaccinations, its diagnosis and reporting accuracy were hampered by limited diagnostic tools, overlapping clinical presentations, and inadequate surveillance systems. These factors collectively contributed to an incomplete understanding of GBS in the pre-vaccine era, making it challenging to assess whether the syndrome was a more significant problem then compared to later periods. Modern advancements in diagnostics and epidemiology have since improved our ability to study GBS, but historical data must be interpreted with caution due to these inherent limitations.
Vaccines: The Unsung Heroes Saving Millions of Lives
You may want to see also
Explore related products



![]()
Natural causes of Guillain-Barré syndrome unrelated to vaccinations
Guillain-Barré syndrome (GBS) is a rare neurological disorder in which the body's immune system mistakenly attacks the peripheral nervous system, leading to muscle weakness, numbness, and sometimes paralysis. While vaccinations have been associated with a small increased risk of GBS in specific cases, it is crucial to recognize that the majority of GBS cases occur due to natural causes unrelated to vaccinations. Historical records and medical literature indicate that GBS was indeed a recognized problem long before the widespread use of vaccines, suggesting that the syndrome has natural origins.
One of the primary natural causes of GBS is infection by certain pathogens. Viral and bacterial infections are known to trigger the immune response that can lead to GBS. For example, Campylobacter jejuni, a bacterium commonly associated with foodborne illnesses, is the most frequent antecedent infection linked to GBS. Studies have shown that approximately 30% of GBS cases are preceded by a Campylobacter infection. Other pathogens, such as cytomegalovirus (CMV), Epstein-Barr virus (EBV), and influenza virus, have also been identified as triggers for GBS. These infections can prompt the immune system to produce antibodies that cross-react with nerve tissues, leading to the characteristic symptoms of GBS.
In addition to infections, autoimmune disorders can contribute to the development of GBS independently of vaccinations. Conditions such as lupus, rheumatoid arthritis, and HIV/AIDS can dysregulate the immune system, making it more likely to attack the peripheral nerves. The underlying mechanisms in these cases involve molecular mimicry, where the immune system mistakenly targets nerve components due to their similarity to certain antigens. This autoimmune response is a natural process that occurs in susceptible individuals, highlighting that GBS can arise from intrinsic biological factors rather than external interventions like vaccines.
Environmental factors and genetic predispositions also play a role in the natural occurrence of GBS. Some individuals may have a genetic susceptibility that increases their risk of developing the syndrome when exposed to certain triggers. Additionally, environmental factors such as exposure to toxins or other stressors can potentially contribute to the onset of GBS. These factors underscore the complexity of GBS etiology and reinforce the idea that the syndrome has existed and will continue to occur regardless of vaccination practices.
Lastly, it is important to note that GBS is a rare condition, and its incidence rate has remained relatively stable over time, even before the introduction of modern vaccines. Historical medical reports describe cases of GBS-like illnesses dating back to the late 19th century, long before many vaccines were developed. This historical context provides strong evidence that GBS is primarily a naturally occurring disorder, with infections, autoimmune processes, genetic factors, and environmental influences being the key drivers of its development. Understanding these natural causes is essential for accurately assessing the risks and benefits of vaccinations and for addressing misconceptions about their role in GBS.
Varicella Vaccine Vesicles: Are Post-Vaccination Blisters Normal?
You may want to see also
![]()
Epidemiological data on Guillain-Barré syndrome prior to 1900s
Guillain-Barré syndrome (GBS) is a rare neurological disorder characterized by rapid-onset muscle weakness caused by the immune system damaging the peripheral nervous system. While the syndrome is well-documented in modern medical literature, its historical prevalence and incidence prior to the 1900s are less clear. Epidemiological data from this period is limited due to the lack of standardized medical records, diagnostic tools, and awareness of the condition. However, historical accounts and retrospective analyses provide some insights into the existence and recognition of GBS-like illnesses before the 20th century.
Before the 1900s, descriptions of illnesses resembling GBS were scattered across medical literature, often under different names or misdiagnosed as other conditions. For instance, in the 18th and 19th centuries, physicians documented cases of acute flaccid paralysis with ascending symptoms, which align with the clinical presentation of GBS. These early reports were frequently attributed to "landry's paralysis" or "acute idiopathic polyneuritis," terms that predated the formal identification of GBS. The lack of a unified diagnostic framework made it difficult to distinguish GBS from similar conditions, such as poliomyelitis or other infectious neuropathies, further complicating epidemiological assessments.
The first detailed clinical descriptions that closely match GBS were published in the late 19th century. In 1859, French physician Jean-Baptiste Octave Landry described a condition characterized by ascending paralysis, which he termed "ascending paralysis with respiratory arrest." Similarly, in 1876, French neurologists Georges Guillain, Jean-Alexandre Barré, and André Strohl reported a series of cases involving progressive muscle weakness and areflexia, though their work gained prominence only in the early 20th century. These early observations suggest that GBS was present but not systematically recognized or studied before the 1900s.
Epidemiological data from this era is largely anecdotal, as population-level studies did not exist. However, it is inferred that GBS was rare, as it was not described as a widespread or epidemic condition. The absence of vaccination programs prior to the 1900s eliminates the possibility of linking GBS to vaccines, a topic of modern debate. Instead, historical cases were likely associated with infectious triggers, such as Campylobacter jejuni or cytomegalovirus infections, which are now known to precede GBS in many instances.
In conclusion, while Guillain-Barré syndrome was not formally identified until the early 20th century, historical medical literature indicates that GBS-like illnesses existed prior to the 1900s. The lack of standardized diagnostics and epidemiological methods makes it challenging to determine the exact prevalence or incidence of the syndrome during this period. However, the rarity of documented cases suggests that GBS was not a major public health concern before the advent of modern medicine and vaccination programs. Understanding this historical context is crucial for addressing misconceptions about the relationship between GBS and vaccinations.
Safe Toddler Detox: Supporting Vaccine Recovery Naturally and Gently
You may want to see also
![]()
Comparison of Guillain-Barré syndrome rates before and after vaccine introduction
Guillain-Barré syndrome (GBS) is a rare neurological disorder in which the body's immune system mistakenly attacks the peripheral nervous system, leading to muscle weakness and sometimes paralysis. The question of whether GBS was a significant problem before the introduction of vaccines is crucial for understanding the syndrome's historical context and its association with immunization programs. Historical medical records indicate that GBS has been recognized as a distinct clinical entity since the early 20th century, well before the widespread use of vaccines. The first detailed description of the condition was provided by Georges Guillain, Jean Alexandre Barré, and André Strohl in 1916, based on observations of patients with ascending paralysis and albuminocytological dissociation in cerebrospinal fluid. This suggests that GBS was already a recognized medical issue, albeit rare, prior to the development of modern vaccines.
Before the introduction of vaccines, the incidence of GBS was estimated to be approximately 1 to 2 cases per 100,000 people annually. This baseline rate is considered the natural occurrence of the syndrome in the absence of external triggers. The rarity of GBS made it challenging to study extensively, but its existence was well-documented in medical literature. Notably, GBS has been associated with various infections, including Campylobacter jejuni, cytomegalovirus, and influenza, which were common triggers even before vaccines became widespread. This highlights that GBS was not solely a post-vaccination phenomenon but rather a condition with multiple potential causes.
The introduction of vaccines, particularly the 1976 swine influenza vaccine in the United States, brought GBS into the spotlight due to a reported increase in cases among vaccinated individuals. Studies conducted during and after the 1976 vaccination campaign found a small but statistically significant elevated risk of GBS, estimated at approximately 1 additional case per 100,000 vaccinated individuals. This incident raised concerns about a potential causal link between vaccines and GBS. However, it is essential to note that subsequent vaccines, including those for influenza, have been associated with much lower risks of GBS, typically ranging from 0 to 1 additional case per million doses administered.
Comparing GBS rates before and after vaccine introduction reveals that while the syndrome was present before vaccines, the risk of developing GBS post-vaccination remains extremely low. Modern surveillance systems, such as the Vaccine Adverse Event Reporting System (VAERS) and the Global Advisory Committee on Vaccine Safety, continuously monitor GBS cases to ensure vaccine safety. These systems have confirmed that the baseline incidence of GBS has not significantly changed since the pre-vaccine era, except for rare instances of slight increases following specific vaccination campaigns. This comparison underscores that GBS, while a serious condition, is not predominantly a vaccine-induced problem but rather a rare disorder with multifactorial origins.
In conclusion, Guillain-Barré syndrome was indeed a recognized medical issue prior to the introduction of vaccines, with a baseline incidence of 1 to 2 cases per 100,000 people annually. The association between GBS and vaccines emerged primarily after the 1976 swine flu vaccination campaign, which led to heightened scrutiny and improved monitoring of vaccine safety. However, the overall risk of GBS post-vaccination remains minimal, and the syndrome's occurrence is largely consistent with pre-vaccine rates. This comparison emphasizes the importance of balancing the rare risks of vaccination against the substantial benefits of preventing infectious diseases, while also acknowledging the historical presence of GBS as a naturally occurring condition.
Fully Vaccinated Deaths: Unraveling the Facts and Figures
You may want to see also
Frequently asked questions
Yes, Guillain-Barré Syndrome was first described in the medical literature in 1859 by Jean-Baptiste Octave Landry, long before modern vaccinations were developed.
While rare cases of GBS have been temporally associated with certain vaccines, the overall incidence of GBS has not significantly increased due to vaccinations. The condition is primarily linked to infections, not vaccines.
GBS is not primarily caused by vaccinations. It is an autoimmune disorder often triggered by infections, such as those caused by Campylobacter jejuni or the flu virus. Vaccines are rarely associated with GBS and the risk is extremely low.
Yes, there are historical records of GBS-like symptoms dating back to the 19th century, well before the development of modern vaccines.
No, the risk of developing GBS from vaccines is significantly lower than the risk associated with natural infections, such as influenza or bacterial infections, which are known triggers of the condition.