Scalded Skin Syndrome (SSS), also known as Staphylococcal Scalded Skin Syndrome, is a serious but rare skin condition primarily affecting infants and young children, caused by toxins produced by certain strains of Staphylococcus aureus bacteria. It is characterized by widespread blistering and peeling of the skin, resembling a burn or scald. While SSS is typically treated with antibiotics to combat the bacterial infection, there is currently no specific vaccine available to prevent it. Prevention strategies focus on reducing the risk of staphylococcal infections through good hygiene practices and prompt treatment of skin infections. Research into vaccines targeting Staphylococcus aureus is ongoing, but as of now, no vaccine has been developed specifically for Scalded Skin Syndrome.
| Characteristics | Values |
|---|---|
| Disease Name | Scalded Skin Syndrome (SSS) |
| Also Known As | Staphylococcal Scalded Skin Syndrome (SSSS), Ritter’s Disease |
| Cause | Toxins (exfoliative toxins A and B) produced by Staphylococcus aureus bacteria |
| Affected Population | Primarily infants and young children (under 5 years), occasionally adults with renal failure or immunodeficiency |
| Symptoms | Widespread painful skin peeling, resembling a burn; fever, redness, tenderness, and fluid-filled blisters |
| Vaccine Availability | No specific vaccine currently available |
| Prevention Methods | Good hygiene, prompt treatment of staphylococcal infections, avoiding close contact with infected individuals |
| Treatment | Antibiotics (e.g., penicillinase-resistant penicillins, cephalosporins), supportive care (fluid management, wound care) |
| Prognosis | Generally good with early treatment; rare complications include dehydration, sepsis, or death |
| Research Status | No active vaccine development reported; focus remains on antibiotic treatment and prevention strategies |
Explore related products






What You'll Learn
- Vaccine Development Status: Current research and progress on a potential vaccine for scalded skin syndrome
- Causes and Prevention: Understanding the bacterial origins and preventive measures to avoid scalded skin syndrome
- Treatment Alternatives: Existing therapies and medications used in place of a vaccine for management
- Risk Factors: Identifying populations most vulnerable to scalded skin syndrome and why
- Symptoms and Diagnosis: Key indicators of scalded skin syndrome and methods for accurate diagnosis
![]()
Vaccine Development Status: Current research and progress on a potential vaccine for scalded skin syndrome
Scalded Skin Syndrome (SSS), primarily caused by *Staphylococcus aureus* bacteria, is a toxin-mediated condition that predominantly affects infants and young children. Despite its severity, there is currently no licensed vaccine specifically for SSS. However, ongoing research and advancements in vaccine development offer hope for future prevention strategies. The focus of current efforts is on targeting the exfoliative toxins (ETs) A and B, which are the primary virulence factors responsible for the characteristic skin detachment in SSS.
Recent studies have explored the potential of toxoid vaccines that neutralize ETs. Researchers have engineered recombinant forms of these toxins to create non-toxic variants that can elicit a protective immune response. Preclinical trials in animal models have shown promising results, with vaccinated subjects demonstrating reduced skin damage and toxin activity when exposed to *S. aureus*. These findings suggest that a toxoid-based vaccine could be a viable approach to preventing SSS, though further testing is required to ensure safety and efficacy in humans.
Another avenue of research involves conjugate vaccines, which combine toxin components with carrier proteins to enhance immune recognition. This strategy has been successful in vaccines for other bacterial infections, such as diphtheria and tetanus. Early-stage investigations into conjugate vaccines for SSS are underway, with researchers optimizing formulations to maximize immunogenicity while minimizing adverse reactions. Collaborative efforts between academic institutions and pharmaceutical companies are accelerating progress in this area.
Additionally, the rise of genomics and bioinformatics has enabled the identification of novel vaccine candidates through reverse vaccinology. By analyzing the *S. aureus* genome, scientists have identified potential surface proteins and antigens that could be targeted in vaccine development. This approach has led to the discovery of several candidate antigens, some of which are currently being evaluated in preclinical studies. These advancements highlight the potential for a multi-antigen vaccine that could provide broader protection against SSS and other staphylococcal infections.
While significant progress has been made, several challenges remain in the development of an SSS vaccine. These include ensuring long-term immunity, addressing the diversity of *S. aureus* strains, and overcoming regulatory hurdles for pediatric vaccines. Clinical trials will be crucial to validate the safety and efficacy of candidate vaccines, particularly in vulnerable populations such as infants. Despite these challenges, the current research landscape indicates that a vaccine for SSS is a feasible goal, with ongoing efforts likely to yield breakthroughs in the coming years.
Vaccination Requirements for Entry into New Zealand
You may want to see also
Explore related products






![]()
Causes and Prevention: Understanding the bacterial origins and preventive measures to avoid scalded skin syndrome
Scalded Skin Syndrome (SSS), also known as Staphylococcal Scalded Skin Syndrome (SSSS), is primarily caused by toxins produced by certain strains of *Staphylococcus aureus* bacteria. These toxins, specifically exfoliative toxins A and B, target the skin’s outermost layer, causing it to separate and peel, resembling a burn or scald. The bacteria often enter the body through minor skin injuries, such as cuts, insect bites, or surgical wounds, or through the respiratory tract. SSS is more commonly seen in children under the age of 5, as their immune systems are still developing and their skin is more susceptible to the effects of these toxins. In rare cases, adults with compromised immune systems or kidney failure may also be affected.
The bacterial origins of SSS highlight the importance of understanding *Staphylococcus aureus* as a common pathogen. This bacterium is often found on the skin and in the nasal passages of healthy individuals without causing harm. However, when it multiplies and releases exfoliative toxins, it can lead to SSS. The condition is not directly contagious, but the bacteria can spread through close contact, shared items, or poor hygiene practices. Therefore, preventing SSS involves minimizing the risk of *Staphylococcus aureus* infections and reducing toxin exposure.
Preventive measures for SSS focus on maintaining good hygiene and reducing bacterial colonization. Regular handwashing with soap and water is essential, especially after contact with individuals who have skin infections or open wounds. Keeping skin clean and moisturized can also prevent minor injuries that allow bacteria to enter. For children, ensuring that cuts, scrapes, and insect bites are promptly cleaned and covered can reduce the risk of infection. Additionally, avoiding sharing personal items like towels, clothing, or bedding can limit the spread of *Staphylococcus aureus*.
In healthcare settings, infection control practices are critical to preventing SSS, particularly in vulnerable populations such as newborns and immunocompromised patients. Healthcare providers should adhere to strict hand hygiene protocols and use sterile techniques during procedures. Early identification and treatment of *Staphylococcus aureus* infections, such as impetigo or cellulitis, can prevent the progression to SSS. Antibiotics may be prescribed to eradicate the bacteria and stop toxin production, but they do not directly neutralize the toxins already present.
Currently, there is no specific vaccine available for SSS or the exfoliative toxins produced by *Staphylococcus aureus*. However, research into vaccines targeting *Staphylococcus aureus* is ongoing, with some candidates focusing on preventing invasive infections caused by the bacterium. While a vaccine for SSS remains a future possibility, the most effective approach today is prevention through hygiene, early treatment of infections, and minimizing bacterial colonization. By understanding the bacterial origins of SSS and implementing these preventive measures, the risk of developing this painful and distressing condition can be significantly reduced.
Canadian Border Reopens: Vaccinated US Citizens Welcome Again
You may want to see also
Explore related products






![]()
Treatment Alternatives: Existing therapies and medications used in place of a vaccine for management
Scalded Skin Syndrome (SSS), also known as Staphylococcal Scalded Skin Syndrome (SSSS), is primarily caused by toxins produced by *Staphylococcus aureus* bacteria. While there is no specific vaccine for SSS, the condition is managed through a combination of supportive care, antimicrobial therapy, and targeted treatments to alleviate symptoms and prevent complications. Below are detailed treatment alternatives and medications used in the absence of a vaccine.
Antimicrobial Therapy: The cornerstone of SSS management is the prompt administration of antibiotics to eradicate the causative *S. aureus* bacteria. Intravenous antibiotics such as flucloxacillin, cefazolin, or clindamycin are commonly used, depending on the patient’s age and the susceptibility of the bacterial strain. Oral antibiotics may be considered for mild cases, but severe infections require systemic treatment. Early initiation of antibiotics is critical to prevent toxin production and further skin damage.
Supportive Skin Care: Gentle skin care is essential to manage the characteristic skin sloughing and discomfort associated with SSS. Affected areas should be kept clean and dry, with regular application of emollients or bland creams to soothe the skin. Avoidance of aggressive scrubbing or peeling is crucial to prevent secondary infections. In severe cases, hospitalization may be required for wound care and monitoring of fluid and electrolyte balance, as extensive skin loss can lead to dehydration and electrolyte imbalances.
Pain Management and Symptomatic Relief: Patients with SSS often experience significant pain and itching due to skin inflammation and peeling. Topical analgesics, such as lidocaine or calamine lotion, can provide localized relief. Oral antihistamines may be prescribed to reduce itching and improve comfort. For severe pain, systemic analgesics like acetaminophen or opioids may be necessary, particularly in pediatric patients who are more commonly affected by SSS.
Fluid and Electrolyte Replacement: Extensive skin involvement in SSS can lead to fluid and electrolyte loss, similar to that seen in burns. Intravenous fluids are often administered to maintain hydration and correct imbalances, especially in children and immunocompromised individuals. Close monitoring of renal function is also important, as toxin-mediated damage can occasionally lead to acute kidney injury.
Prevention of Secondary Infections: The compromised skin barrier in SSS patients makes them susceptible to secondary bacterial or fungal infections. Topical antiseptics or antifungal agents may be applied to at-risk areas. In some cases, prophylactic antibiotics may be considered, particularly if the patient is at high risk for complications. Maintaining a clean environment and minimizing exposure to potential pathogens are also important preventive measures.
In summary, while there is no vaccine for Scalded Skin Syndrome, effective management relies on a combination of antimicrobial therapy, supportive skin care, pain management, fluid replacement, and prevention of secondary infections. Early intervention and comprehensive care are key to achieving positive outcomes and minimizing long-term complications.
Late-Night Vaccine Availability at Alexandria, Minnesota Pharmacies: What to Know
You may want to see also
Explore related products






![]()
Risk Factors: Identifying populations most vulnerable to scalded skin syndrome and why
Scalded Skin Syndrome (SSS), also known as Staphylococcal Scalded Skin Syndrome (SSSS), is a serious skin condition primarily caused by toxins produced by *Staphylococcus aureus* bacteria. While there is no specific vaccine for SSS, understanding the risk factors and vulnerable populations is crucial for prevention and early intervention. The condition predominantly affects specific demographic groups due to their immune status, skin barrier integrity, and exposure to the causative bacteria.
Infants and Young Children: The population most vulnerable to SSS is infants and young children, particularly those under the age of 5. This susceptibility is primarily due to their immature immune systems, which are less capable of neutralizing the exfoliative toxins (ETs) produced by *S. aureus*. Additionally, the skin barrier in young children is less developed, allowing the toxins to penetrate more easily and cause widespread skin damage. Poor hygiene practices and close contact in daycare settings can also increase the risk of bacterial colonization and infection.
Immunocompromised Individuals: People with weakened immune systems, such as those undergoing chemotherapy, living with HIV/AIDS, or taking immunosuppressive medications, are at higher risk of developing SSS. Their reduced ability to combat *S. aureus* infections allows the bacteria to proliferate and produce toxins unchecked. Chronic skin conditions like eczema or psoriasis can further compromise the skin barrier, making it easier for toxins to cause damage.
Elderly Populations: Older adults, particularly those in long-term care facilities, are another at-risk group. Aging skin becomes thinner and more fragile, reducing its ability to act as an effective barrier against bacterial toxins. Additionally, the elderly often have comorbidities and may be on medications that weaken their immune responses, increasing susceptibility to *S. aureus* infections and subsequent SSS. Poor hygiene and close living conditions in care facilities can also contribute to bacterial spread.
Individuals with Pre-existing Skin Conditions: People with pre-existing skin conditions, such as eczema, atopic dermatitis, or impetigo, are more vulnerable to SSS. These conditions compromise the skin’s integrity, providing entry points for *S. aureus* and allowing toxins to cause widespread damage. Scratching or open lesions associated with these conditions can further facilitate bacterial colonization and toxin production.
Healthcare and Institutional Settings: Patients in hospitals, especially those with surgical wounds, catheters, or other invasive devices, are at increased risk due to the higher likelihood of *S. aureus* colonization. Similarly, individuals in crowded institutional settings, such as prisons or military barracks, face elevated risks due to close contact and potential lapses in hygiene. These environments facilitate the spread of *S. aureus*, increasing the likelihood of toxin-mediated SSS.
Identifying these vulnerable populations is essential for targeted prevention strategies, such as improved hygiene, infection control measures, and prompt treatment of *S. aureus* infections. While a vaccine for SSS does not currently exist, addressing these risk factors can significantly reduce the incidence and severity of the condition.
Jane Goodall's Polio Vaccine Drive for Chimps
You may want to see also
Explore related products






![]()
Symptoms and Diagnosis: Key indicators of scalded skin syndrome and methods for accurate diagnosis
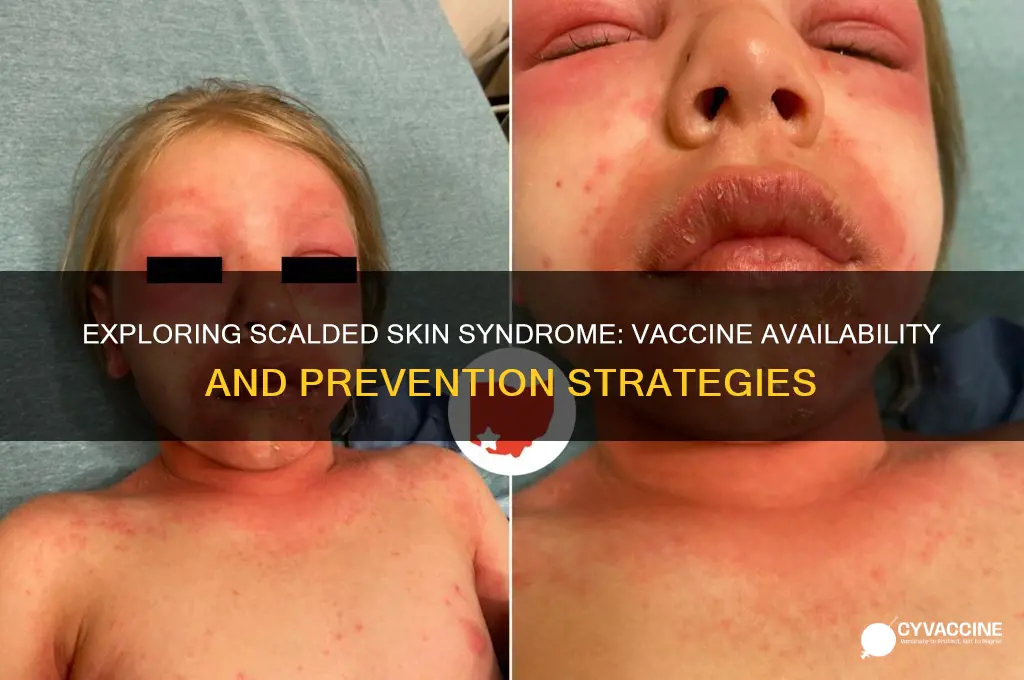
Scalded Skin Syndrome (SSS), also known as Staphylococcal Scalded Skin Syndrome (SSSS), is a serious skin condition primarily affecting infants and young children, though it can occasionally occur in adults with compromised immune systems. The condition is caused by toxins produced by certain strains of *Staphylococcus aureus* bacteria. Recognizing the symptoms and ensuring accurate diagnosis are crucial for prompt treatment and prevention of complications.
Symptoms of Scalded Skin Syndrome
The hallmark symptom of SSS is widespread skin pain and redness, resembling a scald burn, hence the name. Initially, the affected individual may experience fever, irritability, and malaise. Within 24 to 48 hours, a distinctive rash develops, starting as small, red patches that rapidly spread across the body. The skin then becomes tender, swollen, and may develop fluid-filled blisters. A key indicator is the "positive Nikolsky sign," where gentle pressure or rubbing causes the top layer of the skin to peel away easily, leaving a raw, moist surface. This peeling resembles a second-degree burn but is caused by the bacterial toxin damaging the skin’s cohesion. In severe cases, the condition can lead to dehydration, sepsis, or other systemic complications if left untreated.
Diagnosis of Scalded Skin Syndrome
Diagnosis of SSS is primarily clinical, based on the characteristic symptoms and physical examination. Healthcare providers look for the typical rash, skin tenderness, and the positive Nikolsky sign. Laboratory tests, such as blood cultures or skin swabs, may be performed to confirm the presence of *Staphylococcus aureus* and rule out other conditions like bullous impetigo or toxic epidermal necrolysis. In some cases, a biopsy of the affected skin may be taken to examine the tissue under a microscope, though this is less common. Early diagnosis is essential to prevent the condition from worsening and to initiate appropriate treatment, which typically involves antibiotics and supportive care.
Differential Diagnosis
It is important to differentiate SSS from other conditions with similar presentations. For instance, toxic epidermal necrolysis (TEN) also causes skin peeling but is usually associated with medication use and involves deeper layers of the skin. Bullous impetigo, another staphylococcal infection, presents with localized blisters rather than widespread skin detachment. Accurate diagnosis relies on the clinician’s ability to recognize the unique features of SSS and consider the patient’s age, medical history, and risk factors.
Role of Vaccination in Prevention
As of current medical knowledge, there is no specific vaccine available for Scalded Skin Syndrome. However, preventing *Staphylococcus aureus* infections through good hygiene practices, prompt treatment of skin infections, and avoiding close contact with infected individuals can reduce the risk of SSS. Research into vaccines targeting *S. aureus* is ongoing, but no vaccine has been approved specifically for SSS. Until such a vaccine is developed, early recognition and treatment remain the cornerstone of managing this condition.
Scalded Skin Syndrome is a toxin-mediated skin condition with distinct symptoms that require prompt diagnosis and treatment. Key indicators include widespread redness, skin tenderness, and the Nikolsky sign. Diagnosis is primarily clinical, supported by laboratory tests when necessary. While there is no vaccine for SSS, preventive measures against *S. aureus* infections are vital. Awareness of the symptoms and timely medical intervention are critical to managing this potentially severe condition effectively.
J&J Vaccine Deaths: Separating Fact from Fiction and Misinformation
You may want to see also
Frequently asked questions
No, there is no specific vaccine for scalded skin syndrome. SSS is caused by toxins produced by certain bacteria, primarily *Staphylococcus aureus*, and prevention focuses on managing bacterial infections rather than vaccination.
Currently, there are no vaccines available to prevent *Staphylococcus aureus* infections, which are the primary cause of SSS. However, good hygiene, wound care, and prompt treatment of bacterial infections can reduce the risk.
Research is ongoing to develop vaccines against *Staphylococcus aureus*, which could indirectly reduce the risk of SSS. However, no such vaccine is currently available or approved for use. Prevention remains focused on infection control measures.