Hepatitis A and Hepatitis C are distinct viral infections affecting the liver, but they are not prevented by the same vaccine. The Hepatitis A vaccine is specifically designed to protect against the Hepatitis A virus (HAV), which is typically transmitted through contaminated food or water. In contrast, there is currently no vaccine available for Hepatitis C, which is caused by the Hepatitis C virus (HCV) and primarily spreads through contact with infected blood. While both conditions share similarities in symptoms and liver impact, their modes of transmission, prevention strategies, and treatment options differ significantly, highlighting the importance of understanding their unique characteristics.
Explore related products






What You'll Learn
![]()
Hepatitis A vs. Hepatitis C: Different Viruses
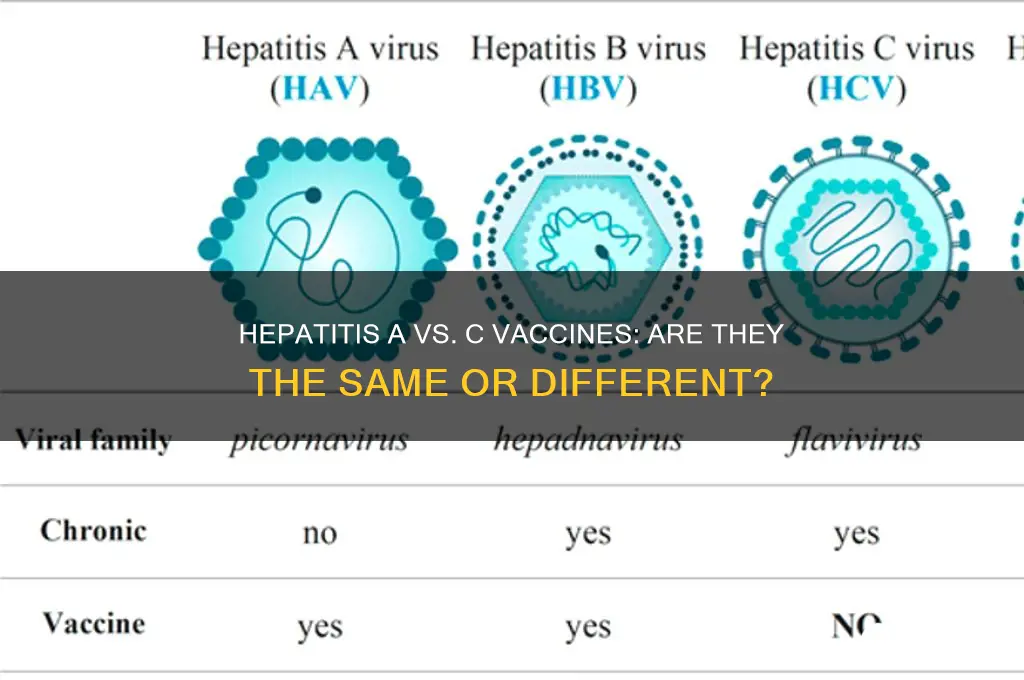
Hepatitis A and Hepatitis C are distinct viral infections that affect the liver, but they are caused by different viruses and have different modes of transmission, symptoms, and prevention strategies. Hepatitis A is caused by the Hepatitis A virus (HAV), which is typically transmitted through ingestion of contaminated food or water or through close contact with an infected person. It is often associated with poor sanitation and hygiene. On the other hand, Hepatitis C is caused by the Hepatitis C virus (HCV), primarily spread through contact with infected blood, most commonly through sharing needles or other drug paraphernalia, or through blood transfusions before widespread screening was implemented.
One of the key differences between Hepatitis A and Hepatitis C is their natural history and outcomes. Hepatitis A is usually an acute, short-term infection that does not become chronic. Most people recover fully within a few weeks to months without any long-term liver damage. In contrast, Hepatitis C often leads to chronic infection, with about 75-85% of cases progressing to long-term liver issues, including cirrhosis and liver cancer, if left untreated. This highlights the importance of early detection and treatment for Hepatitis C, whereas Hepatitis A typically resolves on its own.
Vaccination is another critical area where Hepatitis A and Hepatitis C differ. There is a highly effective vaccine for Hepatitis A, which is recommended for travelers to endemic areas, men who have sex with men, people with chronic liver disease, and those experiencing homelessness, among other risk groups. The Hepatitis A vaccine is administered in two doses and provides long-term immunity. In contrast, there is currently no vaccine available for Hepatitis C. Prevention of Hepatitis C relies on avoiding exposure to infected blood, such as through safe injection practices and using sterile medical equipment.
Symptoms and diagnosis also vary between the two infections. Hepatitis A symptoms include jaundice, fatigue, abdominal pain, and nausea, typically appearing 2 to 6 weeks after exposure. Diagnosis is confirmed through blood tests detecting HAV-specific antibodies. Hepatitis C may cause mild symptoms or none at all in its early stages, making it harder to diagnose without specific testing. Chronic Hepatitis C is diagnosed through blood tests that detect HCV antibodies and viral RNA. Advances in treatment have made Hepatitis C curable with direct-acting antiviral medications, while Hepatitis A treatment focuses on managing symptoms and ensuring adequate rest and hydration.
In summary, while both Hepatitis A and Hepatitis C affect the liver, they are caused by different viruses and have distinct characteristics. Hepatitis A is acute, preventable with a vaccine, and typically resolves without long-term consequences. Hepatitis C, however, often becomes chronic, has no vaccine, and requires specific antiviral treatment to prevent severe liver damage. Understanding these differences is crucial for prevention, diagnosis, and management of these infections.
Puppy Vaccines: 5-in-1 Protection
You may want to see also
Explore related products






![]()
Vaccine Availability: Hep A Has One, Hep C Does Not
The availability of vaccines for Hepatitis A (Hep A) and Hepatitis C (Hep C) highlights a significant difference in preventive measures for these two distinct viral infections. Hepatitis A, caused by the Hep A virus (HAV), has a well-established and widely available vaccine that has been in use for decades. This vaccine is highly effective in preventing Hep A infection and is recommended for various groups, including travelers to endemic areas, men who have sex with men, people with chronic liver disease, and those experiencing homelessness. The Hep A vaccine is typically administered in two doses, providing long-term immunity and significantly reducing the risk of infection. Its availability has played a crucial role in decreasing the incidence of Hep A worldwide, especially in regions with high vaccination coverage.
In contrast, Hepatitis C, caused by the Hep C virus (HCV), does not have an available vaccine despite extensive research efforts. Hep C is primarily transmitted through blood-to-blood contact and is a leading cause of chronic liver disease, cirrhosis, and liver cancer. While direct-acting antiviral medications can cure Hep C in most cases, the lack of a vaccine means that prevention relies heavily on behavioral changes and harm reduction strategies, such as safe injection practices and avoiding needle sharing. The absence of a Hep C vaccine is a major public health challenge, as it limits the ability to prevent new infections on a large scale, particularly in high-risk populations.
The reasons for the disparity in vaccine availability between Hep A and Hep C are rooted in the biological differences between the two viruses. HAV is an RNA virus with a relatively stable structure, making it easier to target with a vaccine. In contrast, HCV is also an RNA virus but exhibits a high degree of genetic diversity and rapid mutation rates, which complicate vaccine development. Researchers have been working on Hep C vaccine candidates for years, but the virus's ability to evade the immune system has made it difficult to create a broadly effective vaccine. Despite these challenges, ongoing research offers hope for future breakthroughs.
From a public health perspective, the availability of a Hep A vaccine underscores the importance of investing in preventive measures for viral hepatitis. It serves as a model for how vaccination can control and potentially eliminate a disease. Conversely, the absence of a Hep C vaccine highlights the need for continued innovation and funding in vaccine research, particularly for complex viruses. Until a Hep C vaccine becomes available, efforts must focus on expanding access to testing, treatment, and harm reduction programs to mitigate the impact of the disease.
In summary, while Hep A benefits from a widely available and effective vaccine, Hep C remains without one, creating a stark contrast in preventive strategies. This difference emphasizes the challenges in vaccine development for certain viruses and the critical role of public health initiatives in managing these infections. Understanding these distinctions is essential for healthcare providers, policymakers, and the public to address the burden of Hep A and Hep C effectively.
Vaccine Safety Concerns: Exploring the Impact on Children's Health
You may want to see also
Explore related products

$24.99





![]()
Transmission Routes: How Hep A and Hep C Spread Differently
Hepatitis A (Hep A) and Hepatitis C (Hep C) are distinct viral infections affecting the liver, but they differ significantly in their transmission routes. Understanding how these viruses spread is crucial for prevention and control. Hep A is primarily transmitted through the fecal-oral route, meaning the virus is ingested after coming into contact with food, water, or objects contaminated by the feces of an infected person. This often occurs in areas with poor sanitation or through close personal contact, such as within households or among sexual partners. Consuming raw or undercooked shellfish from contaminated water is another common mode of transmission. In contrast, Hep C is a blood-borne virus, primarily spreading through direct contact with infected blood. This typically occurs through sharing needles or other drug paraphernalia, receiving blood transfusions or organ transplants before widespread screening (prior to 1992), or less commonly, through sexual contact with an infected person, especially if it involves blood exposure.
The differences in transmission routes highlight the need for targeted prevention strategies. For Hep A, public health efforts focus on improving sanitation, ensuring access to clean water, and promoting vaccination, especially in high-risk populations. The Hep A vaccine is highly effective and is often recommended for travelers to regions with high Hep A prevalence, men who have sex with men, and people with chronic liver disease. On the other hand, Hep C prevention centers on reducing exposure to infected blood. This includes harm reduction programs for people who inject drugs, ensuring safe medical practices, and screening blood donations. While there is no vaccine for Hep C, advancements in antiviral treatments have made it possible to cure the infection in most cases.
Another key difference is the role of sexual transmission. While Hep A can spread through sexual contact, particularly in practices involving oral-anal contact, Hep C is less commonly transmitted sexually. However, individuals with multiple sexual partners, those engaging in rough sex, or people living with HIV are at higher risk for sexual transmission of Hep C. This underscores the importance of safe sexual practices, such as using condoms, in reducing the risk of both infections.
Vertical transmission, or the spread from mother to child, also differs between the two viruses. Hep A is rarely transmitted from an infected mother to her baby during pregnancy or childbirth, and breastfeeding is considered safe. In contrast, Hep C can be transmitted from mother to child, though the risk is relatively low (around 5-6%). Factors such as high viral load in the mother or co-infection with HIV can increase this risk. Screening pregnant women for Hep C and treating those infected can help reduce the likelihood of transmission.
In summary, the transmission routes of Hep A and Hep C are fundamentally different, reflecting their distinct natures as fecal-orally transmitted and blood-borne viruses, respectively. These differences have significant implications for prevention, vaccination, and public health strategies. While Hep A can be prevented with a vaccine, Hep C relies on avoiding blood exposure and early treatment. Recognizing these differences is essential for individuals and healthcare providers to protect against these liver infections effectively.
Illinois Vaccination Progress: Tracking Adult COVID-19 Immunization Rates
You may want to see also
Explore related products






![]()
Symptoms and Severity: Comparing Hep A and Hep C Effects
Hepatitis A (Hep A) and Hepatitis C (Hep C) are distinct viral infections affecting the liver, but they differ significantly in their symptoms, severity, and long-term effects. Understanding these differences is crucial, as there is no combined vaccine for both, and their management approaches vary. While Hep A is typically acute and self-limiting, Hep C often leads to chronic infection with more severe complications if left untreated.
Symptoms of Hep A vs. Hep C: Hep A symptoms usually appear 2 to 6 weeks after exposure and include fatigue, nausea, abdominal pain, jaundice, and dark urine. These symptoms are often acute but resolve within a few weeks to months without causing chronic liver disease. In contrast, Hep C symptoms may not appear for years, making it a "silent" infection. When symptoms do occur, they are similar to Hep A but can also include joint pain, fever, and loss of appetite. However, up to 80% of acute Hep C cases are asymptomatic, increasing the risk of undetected chronic infection.
Severity and Long-Term Effects: Hep A is generally less severe and does not progress to chronic liver disease. Most individuals recover fully without complications. However, in rare cases, acute liver failure can occur, particularly in older adults or those with underlying liver conditions. On the other hand, Hep C is far more severe in the long term. Approximately 75-85% of acute Hep C cases develop into chronic infection, which can lead to cirrhosis, liver cancer, or liver failure over decades. Chronic Hep C is a leading cause of liver transplants worldwide.
Vaccination and Prevention: A key difference between the two is that Hep A has a vaccine, which is highly effective in preventing infection. The Hep A vaccine is often recommended for travelers to endemic areas, men who have sex with men, and individuals with certain medical conditions. In contrast, there is no vaccine for Hep C, making prevention strategies such as avoiding needle sharing and practicing safe sex critical. While direct-acting antiviral medications can cure Hep C, early detection is essential to prevent long-term liver damage.
Impact on Public Health: The distinct nature of Hep A and Hep C underscores the importance of targeted public health strategies. Hep A outbreaks are often linked to contaminated food or water, requiring rapid vaccination campaigns and sanitation improvements. Hep C, however, is primarily spread through blood-to-blood contact, necessitating harm reduction programs for injection drug users and screening for at-risk populations. Recognizing the differences in symptoms, severity, and prevention methods is vital for effective management and control of these hepatitis viruses.
Understanding Your Genetic Risk: Testing for Vaccine Reaction Susceptibility
You may want to see also
Explore related products






![]()
Prevention Strategies: Vaccination for Hep A, Treatment for Hep C
Hepatitis A (Hep A) and Hepatitis C (Hep C) are distinct viral infections affecting the liver, but they require different prevention and treatment approaches. A common question is whether there is a combined vaccine for both, but the answer is no—Hep A and Hep C are not prevented by the same vaccine. Instead, prevention strategies focus on vaccination for Hep A and targeted treatment for Hep C. Understanding these differences is crucial for effective management of both conditions.
Prevention Strategies for Hepatitis A: Vaccination
Hepatitis A is primarily prevented through vaccination, which is highly effective and recommended for specific populations. The Hep A vaccine is typically administered in two doses, 6 to 18 months apart, providing long-term immunity. The Centers for Disease Control and Prevention (CDC) recommends vaccination for all children starting at age 1, travelers to countries with high Hep A prevalence, men who have sex with men, people who use drugs, and individuals with chronic liver disease. Additionally, practicing good hygiene, such as frequent handwashing and avoiding contaminated food or water, complements vaccination efforts to reduce transmission.
Treatment for Hepatitis C: Direct-Acting Antivirals
Unlike Hep A, which often resolves on its own without specific treatment, Hep C requires targeted therapy. The advent of direct-acting antiviral (DAA) medications has revolutionized Hep C treatment, offering cure rates exceeding 95%. These medications work by targeting the virus to stop its replication, typically taken orally for 8 to 12 weeks. Early diagnosis through blood testing is essential, as untreated Hep C can lead to severe liver complications, including cirrhosis and liver cancer. While there is no vaccine for Hep C, prevention focuses on avoiding exposure to infected blood, such as through safe injection practices and avoiding shared needles.
Key Differences in Prevention and Treatment
The primary distinction between Hep A and Hep C lies in their prevention and treatment modalities. Hep A prevention relies on vaccination and hygiene measures, as the infection is usually self-limiting and does not become chronic. In contrast, Hep C treatment involves antiviral medications, and prevention emphasizes risk reduction strategies since no vaccine exists. Both conditions highlight the importance of public health initiatives, including vaccination campaigns for Hep A and screening programs for Hep C, to reduce disease burden.
Integrated Approaches for Liver Health
While Hep A and Hep C differ in their management, both underscore the importance of liver health. Vaccination for Hep A is a proactive measure to prevent liver inflammation, while timely treatment for Hep C can prevent long-term liver damage. Public awareness campaigns, healthcare provider education, and accessible testing and treatment services are vital components of comprehensive prevention strategies. By addressing these infections through targeted interventions, individuals and communities can significantly reduce the impact of hepatitis on global health.
Pneumonia Vaccine and Sulfa: What's the Link?
You may want to see also
Frequently asked questions
No, Hepatitis A and Hepatitis C are caused by different viruses, and there is no combined vaccine for both. Hepatitis A has a vaccine, but Hepatitis C does not.
No, there is currently no vaccine available for Hepatitis C. Vaccination is only possible for Hepatitis A and Hepatitis B.
No, Hepatitis A is typically transmitted through contaminated food or water and often resolves on its own, while Hepatitis C is spread through blood-to-blood contact and can lead to chronic liver disease if untreated.
You only need the Hepatitis A vaccine for travel, as there is no vaccine for Hepatitis C. Consult a healthcare provider for specific travel recommendations.
No, Hepatitis A is usually spread through contaminated food or water, while Hepatitis C is transmitted through blood contact, such as sharing needles or unsanitized medical equipment.