The AstraZeneca vaccine, also known as AZD1222 or Vaxzevria, has been a widely discussed COVID-19 vaccine, but it is important to clarify that it is not an mRNA vaccine. Unlike mRNA vaccines such as Pfizer-BioNTech and Moderna, which use messenger RNA to instruct cells to produce a protein that triggers an immune response, AstraZeneca employs a different technology. It is a viral vector-based vaccine, utilizing a modified version of a chimpanzee adenovirus (ChAdOx1) to deliver genetic material encoding the SARS-CoV-2 spike protein into cells, prompting the immune system to recognize and combat the virus. This distinction in technology has implications for efficacy, storage, and potential side effects, making it crucial for individuals to understand the differences when considering vaccination options.
Explore related products


$21.79 $29.95

$2.97 $24.95



What You'll Learn
![]()
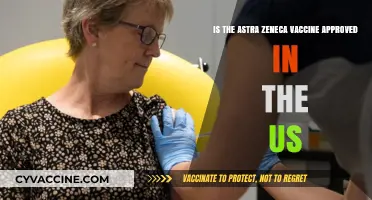
AstraZeneca vaccine type: viral vector, not mRNA technology
The AstraZeneca COVID-19 vaccine, also known as AZD1222 or Vaxzevria, is a pivotal tool in the global fight against the coronavirus pandemic. However, it is essential to clarify that this vaccine does not utilize mRNA technology, which has been a subject of much discussion and interest. Instead, AstraZeneca employs a different approach, known as viral vector technology, to induce an immune response against the SARS-CoV-2 virus. This distinction is crucial for understanding the vaccine's mechanism and addressing any misconceptions.
Viral Vector Technology Explained:
The AstraZeneca vaccine is designed using a modified version of a chimpanzee adenovirus, which is a common cold virus. This adenovirus serves as a vector or carrier, delivering genetic instructions to the cells in our bodies. The vector has been altered to contain the gene for the SARS-CoV-2 spike protein, which is crucial for the virus to enter human cells. When the vaccine is administered, the viral vector enters cells and releases the genetic material, prompting the cells to produce the spike protein. This protein then triggers the immune system to generate antibodies and activate T-cells, preparing the body to fight off the actual coronavirus if exposed.
Differentiating from mRNA Vaccines:
Unlike mRNA vaccines, such as those developed by Pfizer-BioNTech and Moderna, the AstraZeneca vaccine does not introduce mRNA molecules into the body. mRNA vaccines provide the body with genetic instructions in the form of mRNA, which are then used by our cells to produce the viral protein, eliciting an immune response. In contrast, the viral vector approach used by AstraZeneca delivers DNA instructions via the adenovirus vector. This DNA is then converted into mRNA inside the cell, leading to the production of the spike protein. This fundamental difference in delivery mechanisms sets the AstraZeneca vaccine apart from its mRNA counterparts.
The use of viral vectors is a well-established technique in vaccine development, offering several advantages. Firstly, it can induce a robust immune response, including both antibody and T-cell mediated immunity. Secondly, adenoviruses are non-replicating, meaning they cannot cause disease in the vaccinated individual. This feature ensures the vaccine's safety profile. Additionally, viral vector vaccines can be stored and transported under standard refrigeration temperatures, making distribution more feasible, especially in regions with limited access to ultra-cold storage facilities.
In summary, the AstraZeneca COVID-19 vaccine is a viral vector-based vaccine, a technology that has been proven effective and safe. Its mechanism of action involves delivering genetic material using a harmless adenovirus, prompting the body's immune system to recognize and combat the coronavirus. Understanding the distinction between viral vector and mRNA vaccines is essential for public education and addressing any concerns or misconceptions surrounding these life-saving medical advancements. This knowledge empowers individuals to make informed decisions regarding their health and contributes to a more comprehensive understanding of the diverse tools available in the fight against COVID-19.
How to Access Your UK Vaccination Records: A Simple Guide
You may want to see also
Explore related products






![]()
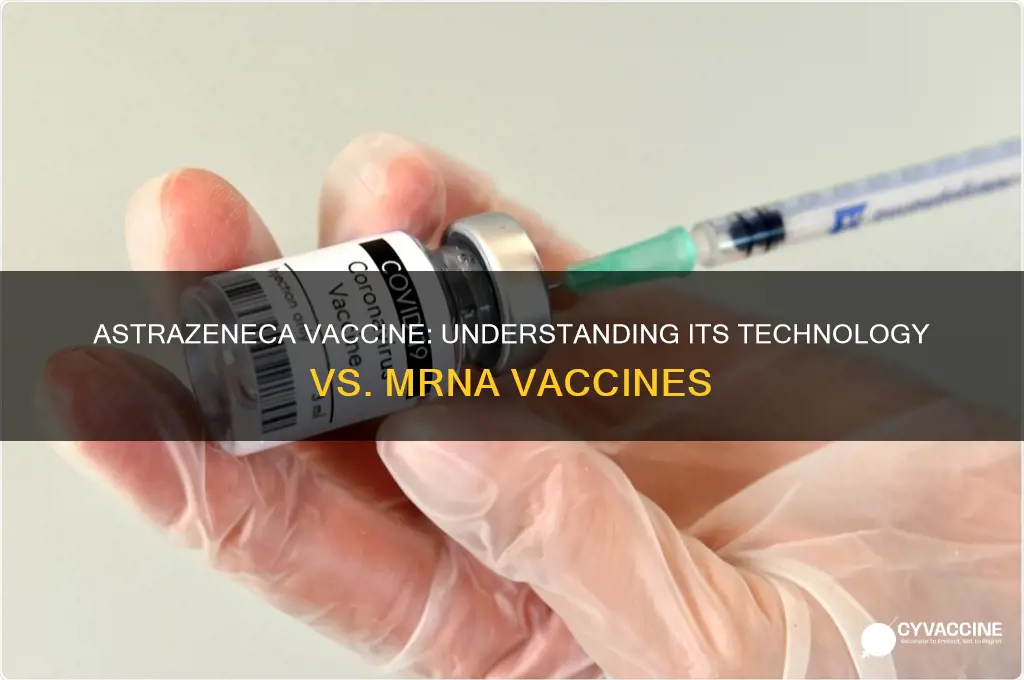
mRNA vaccines vs. AstraZeneca: key differences explained
The AstraZeneca vaccine, also known as ChAdOx1 nCoV-19 or Vaxzevria, is not an mRNA vaccine. Instead, it belongs to a different category of vaccines called viral vector-based vaccines. This fundamental difference in technology is the cornerstone of understanding the contrasts between mRNA vaccines, such as Pfizer-BioNTech and Moderna, and the AstraZeneca vaccine. mRNA vaccines work by introducing a piece of genetic material (mRNA) that instructs cells to produce a harmless protein unique to the virus, triggering an immune response. In contrast, the AstraZeneca vaccine uses a modified version of a chimpanzee adenovirus (ChAdOx1) that delivers genetic material encoding the SARS-CoV-2 spike protein into cells, prompting the immune system to recognize and combat the virus.
One of the key differences between mRNA vaccines and the AstraZeneca vaccine lies in their delivery mechanisms. mRNA vaccines rely on lipid nanoparticles to protect and transport the mRNA into cells, ensuring it reaches the cytoplasm where protein synthesis occurs. The AstraZeneca vaccine, however, employs a viral vector—a harmless adenovirus—to deliver the genetic material. This distinction affects how the vaccines are stored and handled; mRNA vaccines typically require ultra-cold storage (e.g., -70°C for Pfizer), while the AstraZeneca vaccine is stable at standard refrigerator temperatures (2–8°C), making it more accessible in regions with limited cold chain infrastructure.
Another critical difference is the immune response generated. mRNA vaccines primarily stimulate the production of neutralizing antibodies and activate T cells, offering robust protection against symptomatic COVID-19. The AstraZeneca vaccine also induces both antibody and T cell responses but does so through the viral vector mechanism. Additionally, the AstraZeneca vaccine has been associated with a rare side effect known as vaccine-induced immune thrombotic thrombocytopenia (VITT), where the immune system mistakenly attacks platelets, leading to blood clots. This side effect is extremely rare but has influenced its use in certain demographics, particularly younger populations in some countries.
Efficacy and dosing regimens also differ between mRNA vaccines and the AstraZeneca vaccine. Clinical trials have shown that mRNA vaccines have slightly higher efficacy rates against symptomatic COVID-19, often exceeding 90%. The AstraZeneca vaccine has demonstrated efficacy rates around 70–80%, depending on the dosing interval. While mRNA vaccines are typically administered in two doses spaced 3–4 weeks apart, the AstraZeneca vaccine’s optimal dosing interval has been a subject of debate, with studies suggesting longer intervals (e.g., 8–12 weeks) may enhance efficacy.
Finally, public perception and regulatory approvals have played a role in the adoption of these vaccines. mRNA vaccines were the first to receive emergency use authorization in many countries, contributing to their widespread use. The AstraZeneca vaccine faced initial challenges due to concerns over rare side effects and varying trial results, leading to shifting recommendations in some regions. However, it remains a vital tool in global vaccination efforts, particularly in low- and middle-income countries, due to its ease of distribution and lower cost compared to mRNA vaccines. Understanding these differences is essential for informed decision-making and addressing vaccine hesitancy.
Add Your Vaccine Certificate to Service NSW App: Easy Steps
You may want to see also
Explore related products


$20.99 $25.48




![]()
How AstraZeneca’s viral vector approach works
The AstraZeneca COVID-19 vaccine, also known as AZD1222 or Vaxzevria, is not an mRNA vaccine. Instead, it utilizes a different technology called a viral vector-based approach. This method involves using a harmless virus (the vector) to deliver genetic instructions to our cells, prompting them to produce a specific protein that triggers an immune response. In the case of AstraZeneca's vaccine, the vector is a modified version of a chimpanzee adenovirus (ChAdOx1), which cannot cause disease in humans.
The process begins with the creation of the viral vector. Scientists modify the chimpanzee adenovirus by removing its ability to replicate, ensuring it cannot cause illness. They then insert a piece of genetic material encoding the SARS-CoV-2 spike protein—the protein found on the surface of the coronavirus—into the adenovirus's genome. This modified adenovirus becomes the delivery vehicle, or vector, for the genetic instructions. When the vaccine is administered, typically through an intramuscular injection, the viral vector enters cells in the body.
Once inside the cells, the adenovirus releases the genetic material it carries. This genetic material contains the blueprint for the SARS-CoV-2 spike protein. The cell's machinery then reads these instructions and begins producing the spike protein. Importantly, the genetic material does not integrate into the cell's DNA; it simply serves as a temporary template for protein production. The spike proteins produced by the cells are then displayed on their surface or released into the surrounding tissue.
The immune system recognizes these spike proteins as foreign, prompting an immune response. Antigen-presenting cells (APCs) engulf the spike proteins and present fragments of them (antigens) to T cells, activating both helper T cells and killer T cells. Helper T cells stimulate B cells to produce antibodies specific to the spike protein, while killer T cells target and destroy any cells displaying the spike protein. This dual response—antibody production and cellular immunity—prepares the body to recognize and combat the actual SARS-CoV-2 virus if exposure occurs.
One advantage of the viral vector approach is its stability and ease of storage compared to mRNA vaccines, which often require ultra-cold temperatures. AstraZeneca's vaccine can be stored at refrigerator temperatures (2–8°C), making it more accessible for distribution, especially in regions with limited infrastructure. However, unlike mRNA vaccines that teach cells to produce the spike protein directly, the viral vector approach relies on the delivery of genetic material via a modified virus, which can sometimes lead to reduced efficacy if the immune system recognizes and neutralizes the vector before it delivers its payload. Despite this, AstraZeneca's vaccine has proven effective in preventing severe COVID-19 disease and hospitalization.
Blue Cross Blue Shield: Pneumonia Vaccine Coverage
You may want to see also
Explore related products






![]()
Comparing AstraZeneca to Pfizer and Moderna mRNA vaccines
The AstraZeneca vaccine, developed in collaboration with the University of Oxford, is not an mRNA vaccine, unlike the Pfizer-BioNTech and Moderna vaccines. Instead, AstraZeneca uses a viral vector-based technology. This fundamental difference in design is crucial when comparing these vaccines. mRNA vaccines, such as Pfizer and Moderna, work by delivering genetic material (mRNA) that instructs cells to produce a harmless piece of the SARS-CoV-2 spike protein, triggering an immune response. In contrast, the AstraZeneca vaccine uses a modified version of a chimpanzee adenovirus (ChAdOx1) to deliver the genetic code for the spike protein into cells, prompting a similar immune reaction.
One key distinction in efficacy is the reported effectiveness against symptomatic COVID-19. Pfizer and Moderna vaccines have consistently shown higher efficacy rates in clinical trials, with Pfizer reporting around 95% and Moderna around 94%. AstraZeneca's efficacy rate varies more widely, typically ranging from 60% to 90% depending on the dosing regimen and population studied. However, all three vaccines have proven highly effective in preventing severe disease, hospitalization, and death, which remains their primary goal.
Another important comparison is the storage and distribution requirements. AstraZeneca's vaccine offers a significant advantage in this area, as it can be stored at standard refrigerator temperatures (2°C to 8°C) for up to six months. This makes it more accessible for low- and middle-income countries with limited cold chain infrastructure. In contrast, Pfizer's mRNA vaccine requires ultra-cold storage (-70°C) and Moderna's requires cold storage (-20°C), though both can be stored at refrigerator temperatures for a limited time after thawing.
Side effects and safety profiles also differ among the vaccines. Common side effects for all three include pain at the injection site, fatigue, headache, and muscle pain. However, AstraZeneca has been associated with rare but serious side effects, such as thrombosis with thrombocytopenia syndrome (TTS), particularly in younger populations. This has led some countries to restrict its use in certain age groups. Pfizer and Moderna have also reported rare cases of myocarditis and pericarditis, primarily in young males after the second dose.
Lastly, the dosing regimens vary. Pfizer and Moderna require two doses, typically administered 3 to 4 weeks apart for Pfizer and 4 weeks apart for Moderna. AstraZeneca also requires two doses, but the interval can range from 4 to 12 weeks, with some studies suggesting a longer interval may enhance efficacy. This flexibility can be advantageous in vaccine rollout strategies, particularly in regions with supply constraints.
In summary, while AstraZeneca, Pfizer, and Moderna vaccines all effectively protect against severe COVID-19, they differ in technology, efficacy rates, storage requirements, side effect profiles, and dosing regimens. The choice of vaccine often depends on availability, logistical considerations, and individual health factors, highlighting the importance of having multiple vaccine options in the global fight against the pandemic.
Vaccines and Antibiotics: Safe to Combine or Risky Interaction?
You may want to see also
Explore related products



![]()
Efficacy and safety: AstraZeneca vs. mRNA vaccines
The AstraZeneca vaccine, also known as ChAdOx1 nCoV-19 or Vaxzevria, is not an mRNA vaccine. Instead, it is a viral vector-based vaccine, which uses a modified version of a chimpanzee adenovirus to deliver genetic material encoding the SARS-CoV-2 spike protein into human cells. This approach differs fundamentally from mRNA vaccines like Pfizer-BioNTech and Moderna, which use messenger RNA to instruct cells to produce the spike protein directly. Understanding these differences is crucial when comparing their efficacy and safety profiles.
In terms of efficacy, clinical trials have shown that both AstraZeneca and mRNA vaccines provide robust protection against severe COVID-19, hospitalization, and death. However, mRNA vaccines have demonstrated slightly higher efficacy rates in preventing symptomatic infection. For instance, Pfizer-BioNTech and Moderna vaccines reported efficacy rates of around 94-95% in their initial trials, whereas AstraZeneca's vaccine showed an average efficacy of approximately 70-80%, depending on the dosing regimen. Despite this difference, AstraZeneca's vaccine remains highly effective in preventing severe outcomes, making it a valuable tool in global vaccination efforts, particularly in low- and middle-income countries due to its lower cost and easier storage requirements.
Regarding safety, both vaccine types have been extensively studied and approved by regulatory bodies worldwide. However, rare side effects have been reported for each. AstraZeneca's vaccine has been associated with a very rare risk of thrombosis with thrombocytopenia syndrome (TTS), a condition involving blood clots combined with low platelet levels. This has led some countries to restrict its use in younger populations. On the other hand, mRNA vaccines have been linked to rare cases of myocarditis and pericarditis, primarily in young males after the second dose. These risks are extremely low for both vaccine types, and the benefits of vaccination far outweigh the potential risks for the vast majority of individuals.
Another important consideration is the duration of protection. Studies suggest that mRNA vaccines may provide longer-lasting immunity compared to AstraZeneca's vaccine, with some data indicating a faster waning of efficacy over time for the latter. However, booster doses have proven effective in restoring and extending protection for both vaccine types. The choice between AstraZeneca and mRNA vaccines often depends on availability, local health guidelines, and individual risk factors, such as age and medical history.
In summary, while AstraZeneca's vaccine is not an mRNA vaccine, both types have played critical roles in the global fight against COVID-19. mRNA vaccines offer slightly higher efficacy against symptomatic infection and may provide longer-lasting immunity, but AstraZeneca's vaccine remains highly effective in preventing severe disease and is more accessible in many regions. Safety profiles differ slightly, with rare but distinct side effects associated with each. Ultimately, the decision to use one over the other should be guided by scientific evidence, public health priorities, and individual circumstances.
Is Yellow Fever Vaccination Required for Ghana Travel?
You may want to see also
Frequently asked questions
No, the AstraZeneca vaccine is not an mRNA vaccine. It is a viral vector-based vaccine that uses a modified version of a chimpanzee adenovirus to deliver genetic material encoding the SARS-CoV-2 spike protein.
The AstraZeneca vaccine differs from mRNA vaccines in its technology. Instead of using mRNA to instruct cells to produce the spike protein, it employs a harmless adenovirus to transport the genetic code for the spike protein into cells, triggering an immune response.
The side effects of the AstraZeneca vaccine are generally similar to those of mRNA vaccines, including pain at the injection site, fatigue, headache, and muscle pain. However, rare side effects, such as thrombosis with thrombocytopenia syndrome (TTS), are more specifically associated with the AstraZeneca vaccine.