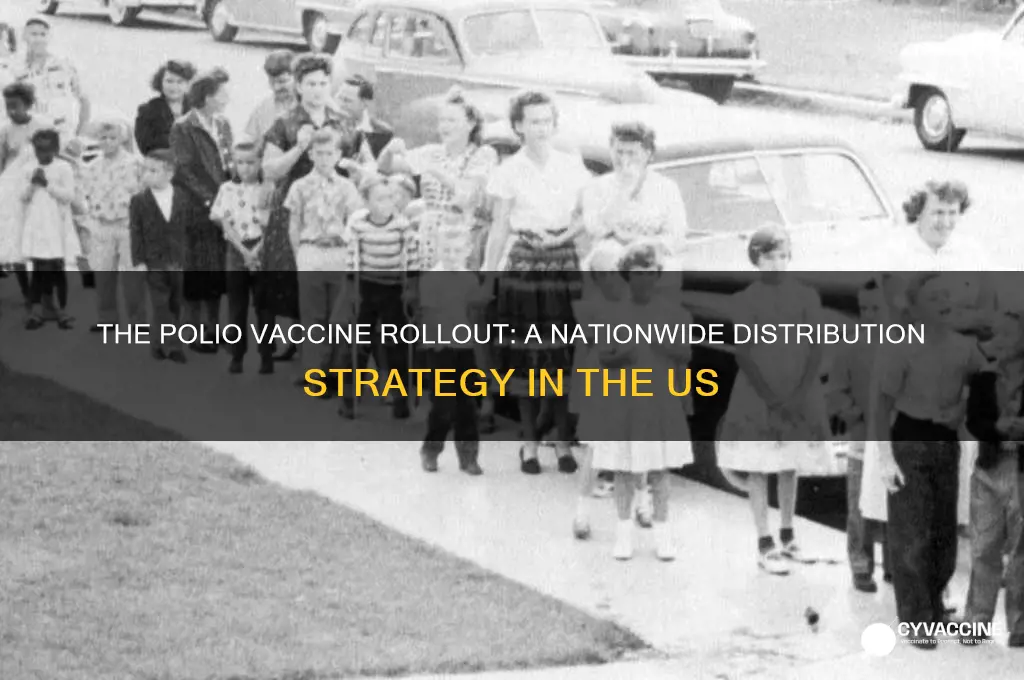
The distribution of the polio vaccine in the United States marked a pivotal moment in public health history, following the successful development of the inactivated polio vaccine (IPV) by Jonas Salk in 1955. Initially, the vaccine was prioritized for high-risk groups, including children and pregnant women, due to the devastating impact of polio outbreaks. The U.S. government, in collaboration with the March of Dimes and local health departments, launched a massive immunization campaign, utilizing schools, clinics, and community centers as vaccination sites. By 1957, the vaccine was widely available to the general public, and mass vaccination drives significantly reduced polio cases, leading to its near eradication in the U.S. by the late 1970s. This effort showcased the power of coordinated public health initiatives and set a precedent for future vaccine distribution strategies.
| Characteristics | Values |
|---|---|
| Vaccine Type | Inactivated Polio Vaccine (IPV) and Oral Polio Vaccine (OPV), though IPV is exclusively used in the U.S. since 2000 due to safety concerns with OPV. |
| Distribution Channels | Primarily through healthcare providers, clinics, schools, and public health departments. |
| Target Population | Infants, children, and adults at risk (e.g., travelers to polio-endemic regions). Routine vaccination schedule starts at 2 months of age. |
| Vaccination Schedule | 4-dose series: at 2 months, 4 months, 6-18 months, and 4-6 years of age. |
| Funding and Accessibility | Supported by the Vaccines for Children (VFC) program for eligible children. Most insurance plans cover the vaccine; uninsured individuals can access it through public health clinics. |
| Cold Chain Requirements | Stored between 2°C and 8°C (36°F and 46°F) to maintain efficacy. |
| Public Awareness Campaigns | Historical campaigns (e.g., March of Dimes) played a key role in the 1950s-60s. Modern efforts focus on maintaining high vaccination rates and addressing hesitancy. |
| Surveillance and Monitoring | Active surveillance by the CDC and state health departments to monitor vaccine coverage and detect potential cases. |
| Eradication Status in the U.S. | Polio eradicated in the U.S. since 1979, with ongoing vaccination to prevent reintroduction. |
| Global Context | The U.S. supports global polio eradication efforts through the Global Polio Eradication Initiative (GPEI) and international vaccine distribution programs. |
| Recent Challenges | Addressing vaccine hesitancy and ensuring equitable access in underserved communities. |
Explore related products


$24.17 $25.99




What You'll Learn
- Early Trials and Approval: Testing phases, safety checks, and FDA approval process for the polio vaccine
- National Immunization Campaigns: Mass vaccination drives, public awareness, and community involvement in distribution
- School-Based Vaccinations: Programs targeting children through schools, clinics, and local health departments
- Logistics and Supply Chain: Cold storage, transportation, and distribution networks to ensure vaccine availability
- Public and Private Partnerships: Collaboration between government, NGOs, and pharmaceutical companies for widespread access
![]()
Early Trials and Approval: Testing phases, safety checks, and FDA approval process for the polio vaccine
The development and approval of the polio vaccine in the United States involved rigorous testing phases, stringent safety checks, and a meticulous FDA approval process to ensure its efficacy and safety before widespread distribution. The journey began in the early 1950s, led by Dr. Jonas Salk, whose inactivated polio vaccine (IPV) became the cornerstone of polio eradication efforts. The first phase of testing involved laboratory and animal studies to establish the vaccine's basic safety and immunogenicity. These preliminary trials demonstrated that the vaccine could induce immunity without causing the disease, paving the way for human trials.
The clinical trials for the Salk vaccine were conducted in three phases, starting with small-scale tests on adults and children to assess safety and dosage. Phase I trials focused on healthy adult volunteers, while Phase II expanded to include children, who were the primary targets of the polio virus. These early trials confirmed the vaccine's safety profile and its ability to stimulate antibody production. The most critical phase, however, was the large-scale field trial in 1954, which involved 1.8 million children across the U.S., Canada, and Finland. This Phase III trial, known as the Francis Field Trial, was a double-blind, placebo-controlled study that rigorously evaluated the vaccine's effectiveness in preventing polio. The results were groundbreaking, showing the vaccine was 80-90% effective in preventing paralytic polio, a milestone in medical history.
Safety checks were integral to each testing phase, with researchers closely monitoring participants for adverse reactions. The vaccine's inactivated form, created using formaldehyde to kill the virus, was designed to eliminate the risk of vaccine-induced polio, a concern with earlier live-virus vaccines. Independent review boards and medical experts scrutinized the data at every stage to ensure transparency and integrity. The absence of serious side effects and the vaccine's proven efficacy bolstered public and scientific confidence in its safety.
The FDA approval process for the polio vaccine was expedited due to the urgency of the polio epidemic, but it did not compromise on standards. On April 12, 1955, the FDA granted approval for the Salk vaccine after thoroughly reviewing the data from the clinical trials. This approval was announced during a press conference at the University of Michigan, an event that marked a turning point in public health. The FDA's endorsement was based on the vaccine's demonstrated safety, efficacy, and manufacturing consistency, ensuring that every dose met strict quality standards.
Following FDA approval, the vaccine was rapidly distributed across the U.S., with mass vaccination campaigns targeting schoolchildren and high-risk populations. The approval process also included post-marketing surveillance to monitor long-term effects and rare adverse events. This comprehensive approach to testing, safety checks, and regulatory approval not only validated the polio vaccine but also set a precedent for the development and distribution of future vaccines, emphasizing the importance of scientific rigor and public trust.
Traveling to Rome: Vaccine Requirements for Entry
You may want to see also
Explore related products






![]()
National Immunization Campaigns: Mass vaccination drives, public awareness, and community involvement in distribution
The distribution of the polio vaccine in the United States during the mid-20th century serves as a landmark example of successful national immunization campaigns. Mass vaccination drives were the cornerstone of this effort, leveraging schools, clinics, and public spaces as vaccination sites. The Sabin oral vaccine, introduced in 1961, was particularly advantageous for mass distribution due to its ease of administration—requiring only a few drops on a sugar cube. These drives were meticulously organized, often targeting entire communities at once to ensure widespread immunity. Mobile clinics and temporary vaccination stations were set up in rural and urban areas alike, making the vaccine accessible to all demographics. The goal was clear: to vaccinate as many people as possible in the shortest time frame to halt the spread of polio.
Public awareness played a pivotal role in the success of these campaigns. The March of Dimes, a nonprofit organization, spearheaded a massive publicity effort to educate the public about the importance of vaccination. Through radio, television, newspapers, and community events, the campaign disseminated information about polio's dangers and the vaccine's safety and efficacy. Celebrities, politicians, and even President Franklin D. Roosevelt, who himself had polio, endorsed the vaccine, boosting public trust. Posters, pamphlets, and public service announcements emphasized the slogan "Polio can be prevented—get vaccinated now!" This widespread awareness ensured high turnout at vaccination sites and encouraged parents to bring their children for immunization.
Community involvement was another critical component of the polio vaccine distribution strategy. Local governments, schools, churches, and civic organizations collaborated to organize vaccination events. Volunteers, including nurses, teachers, and community leaders, were trained to administer the vaccine and manage crowds. In some cases, door-to-door campaigns were conducted to reach individuals who could not attend mass vaccination sites. This grassroots approach fostered a sense of collective responsibility and ensured that even marginalized or hard-to-reach populations were included in the immunization effort. Community involvement also helped address hesitancy by allowing trusted local figures to advocate for vaccination.
The logistical coordination behind these campaigns was immense. Millions of doses needed to be stored, transported, and distributed efficiently, often under time-sensitive conditions. The federal government, in partnership with state and local health departments, established a robust supply chain to ensure vaccines reached every corner of the country. Refrigerated trucks and storage facilities were utilized to maintain the vaccine's potency. Detailed record-keeping systems tracked vaccination rates and identified areas needing additional outreach. This level of organization was essential to achieving the high coverage rates necessary for herd immunity.
Finally, the polio vaccination campaign set a precedent for future national immunization efforts by demonstrating the power of mass drives, public awareness, and community engagement. Its success was measured not only in the dramatic decline of polio cases but also in the framework it established for addressing other vaccine-preventable diseases. The lessons learned—such as the importance of accessibility, trust-building, and collaboration—continue to inform public health strategies today. The polio campaign remains a testament to what can be achieved when governments, organizations, and communities unite toward a common goal: protecting public health through immunization.
MMR Vaccine: Understanding Your Immunity After the First Dose
You may want to see also
Explore related products






![]()
School-Based Vaccinations: Programs targeting children through schools, clinics, and local health departments
The distribution of the polio vaccine in the United States during the mid-20th century was a monumental public health effort, and school-based vaccination programs played a pivotal role in its success. These initiatives targeted children, who were the most vulnerable population to poliomyelitis, by leveraging the existing infrastructure of schools, clinics, and local health departments. Schools were ideal settings for mass vaccination campaigns due to their centralized locations and the ability to reach large numbers of children in a structured environment. Local health departments coordinated with school administrators to organize vaccination drives, ensuring that the process was efficient and accessible. Clinics often served as supplementary sites for children who missed school-based vaccinations or required follow-up doses, creating a comprehensive network of immunization services.
School-based vaccination programs were meticulously planned to minimize disruption to the academic schedule while maximizing participation. Health officials would visit schools on designated days, often setting up temporary clinics in gymnasiums or auditoriums. Parents were notified in advance through letters, community announcements, and local media, emphasizing the importance of vaccinating their children. Consent forms were distributed and collected to ensure compliance with legal and ethical standards. Nurses and trained volunteers administered the vaccine, typically the oral polio vaccine (OPV) developed by Albert Sabin, which was easy to distribute and required no needles, making it more acceptable to children and parents alike. This approach not only facilitated rapid immunization but also helped alleviate public fears about polio through education and direct engagement.
Local health departments were instrumental in the logistical and administrative aspects of school-based vaccination programs. They procured and distributed vaccine supplies, trained personnel, and maintained records of immunized children to track progress and identify gaps. Health departments also collaborated with community leaders and organizations to promote awareness and encourage participation. Mobile clinics were deployed in underserved or rural areas to ensure equitable access to the vaccine. By integrating school-based efforts with broader public health strategies, these programs achieved high vaccination rates, significantly reducing the incidence of polio across the nation.
Clinics played a complementary role in the distribution of the polio vaccine, particularly for children who could not participate in school-based programs. Local clinics offered flexible hours and walk-in services, accommodating families with varying schedules or those who preferred a healthcare setting. They also provided follow-up doses, as the polio vaccine required multiple administrations for full immunity. Clinics served as hubs for addressing parental concerns, offering medical advice, and dispelling myths about vaccine safety. This dual approach—school-based mass vaccination and clinic-based individual care—ensured that the polio vaccine reached as many children as possible, contributing to the eventual eradication of the disease in the U.S.
The success of school-based vaccination programs during the polio era established a model for future public health initiatives, including routine childhood immunizations and pandemic response efforts. These programs demonstrated the effectiveness of leveraging educational institutions as platforms for health interventions, fostering partnerships between schools, health departments, and communities. The lessons learned from polio vaccination campaigns continue to inform strategies for addressing vaccine-preventable diseases today, highlighting the importance of accessibility, education, and collaboration in achieving public health goals.
Vaccine Reactions: Do Combined Vaccines Cause More?
You may want to see also
Explore related products






![]()
Logistics and Supply Chain: Cold storage, transportation, and distribution networks to ensure vaccine availability
The distribution of the polio vaccine in the United States during the mid-20th century required a robust logistics and supply chain framework to ensure widespread availability. Cold storage was a critical component, as the vaccine needed to be maintained at specific temperatures to remain effective. The Sabin oral polio vaccine (OPV), which became the primary vaccine used in the U.S. after 1961, was more heat-stable than the earlier inactivated polio vaccine (IPV), but still required refrigeration between 2°C and 8°C (36°F and 46°F). To address this, the government and pharmaceutical companies established a network of cold storage facilities across the country. These facilities were equipped with reliable refrigeration units and backup power systems to prevent temperature fluctuations during power outages, ensuring the vaccine's potency throughout the supply chain.
Transportation played a pivotal role in the polio vaccine distribution process, particularly given the vast geography of the United States. Vaccines were transported from manufacturing plants to regional distribution centers using refrigerated trucks, often referred to as "reefers," which maintained the required temperature range. For rural and remote areas, smaller, insulated containers with cold packs were used to ensure the vaccine remained viable during the "last mile" of delivery. The U.S. Public Health Service (PHS) and state health departments coordinated these efforts, working closely with private carriers to establish efficient routes and schedules. Air transportation was also utilized for rapid delivery to distant or hard-to-reach locations, ensuring timely availability of the vaccine nationwide.
Distribution networks were designed to reach every corner of the country, from densely populated urban centers to isolated rural communities. Local health departments, schools, and community centers served as vaccination sites, with each location receiving vaccine shipments based on population size and demand. The PHS and the Centers for Disease Control and Prevention (CDC) developed a tiered distribution system, where vaccines were first delivered to state-level warehouses and then redistributed to county or city health departments. This hierarchical approach minimized handling and reduced the risk of temperature exposure, ensuring the vaccine's integrity. Public awareness campaigns were also critical in driving demand and ensuring that distribution efforts were met with high vaccination turnout.
To maintain the cold chain, strict monitoring and quality control measures were implemented. Temperature loggers and data recorders were used to track conditions during storage and transportation, with real-time monitoring systems becoming more prevalent as technology advanced. Health officials conducted regular inspections of storage facilities and transportation vehicles to ensure compliance with temperature requirements. In cases where the cold chain was compromised, vaccines were immediately quarantined and tested for efficacy before being administered to the public. This meticulous approach was essential to prevent wastage and maintain public trust in the vaccination program.
Collaboration between federal, state, and local agencies, as well as private sector partners, was key to the success of the polio vaccine distribution. The March of Dimes, a nonprofit organization, played a significant role in funding research and raising awareness, while pharmaceutical companies scaled up production to meet demand. The military also assisted in transporting vaccines to remote areas and overseas territories. This coordinated effort ensured that the polio vaccine was distributed efficiently, contributing to the near eradication of the disease in the United States by the late 1970s. The lessons learned from this campaign laid the foundation for modern vaccine logistics and supply chain management, influencing subsequent immunization programs such as those for measles, mumps, and COVID-19.
Personalized Cancer Vaccines: A Revolutionary Approach to Prevent Tumor Recurrence
You may want to see also
Explore related products






![]()
Public and Private Partnerships: Collaboration between government, NGOs, and pharmaceutical companies for widespread access
The successful distribution of the polio vaccine in the United States during the mid-20th century serves as a landmark example of effective public and private partnerships. The U.S. government, through agencies like the Public Health Service and the Centers for Disease Control and Prevention (CDC), played a pivotal role in coordinating vaccination efforts. These agencies established guidelines, funded vaccination programs, and ensured the equitable distribution of the vaccine across states. Simultaneously, the March of Dimes, a leading non-governmental organization (NGO), provided critical financial and logistical support. Their fundraising campaigns not only financed the research and development of the vaccine but also helped create public awareness, fostering widespread acceptance of the immunization program.
Pharmaceutical companies, particularly Eli Lilly, Parke-Davis, and Wyeth, were essential partners in this endeavor. These companies scaled up production to meet the unprecedented demand for the polio vaccine, ensuring millions of doses were available within a short timeframe. The government facilitated this process by granting licenses and providing regulatory support, while NGOs like the March of Dimes acted as intermediaries, bridging the gap between manufacturers and public health initiatives. This collaboration ensured that the vaccine was produced efficiently and distributed effectively, reaching even remote areas of the country.
Local health departments and community organizations were another critical component of this partnership. They organized vaccination clinics, administered doses, and maintained records, often with support from federal and state governments. Schools, churches, and public spaces were transformed into vaccination sites, making the vaccine accessible to all age groups. NGOs provided volunteers and resources, while pharmaceutical companies ensured a steady supply of vaccines. This grassroots-level collaboration was instrumental in achieving high vaccination rates and eradicating polio as a public health threat in the U.S.
The role of public awareness campaigns cannot be overstated. NGOs and government agencies worked together to educate the public about the importance of vaccination, addressing skepticism and misinformation. Pharmaceutical companies contributed by providing educational materials and ensuring the vaccine's safety and efficacy. This coordinated effort built trust and encouraged widespread participation in the vaccination program. The success of these campaigns highlights the importance of clear communication and community engagement in public health initiatives.
Finally, the polio vaccine distribution model demonstrated the value of sustained partnerships. After the initial rollout, the government, NGOs, and pharmaceutical companies continued to collaborate on booster shots, surveillance, and global eradication efforts. This long-term commitment ensured that polio remained under control in the U.S. and laid the foundation for similar partnerships in addressing other public health challenges. The polio vaccine distribution stands as a testament to what can be achieved when public and private sectors work together toward a common goal, offering valuable lessons for future health initiatives.
Vaccine Myth: Cancer Risk or Cancer Prevention?
You may want to see also
Frequently asked questions
The polio vaccine, developed by Dr. Jonas Salk, was first distributed in the United States in 1955, following successful large-scale field trials.
The initial distribution of the polio vaccine was prioritized for children and pregnant women, with schools and clinics serving as primary vaccination sites.
The distribution of the polio vaccine was largely funded by the U.S. government, in collaboration with the March of Dimes, a nonprofit organization that played a key role in polio research and vaccination efforts.
Yes, challenges included ensuring equitable access across rural and urban areas, managing vaccine supply shortages, and addressing public skepticism about the vaccine's safety and efficacy.
The widespread distribution of the polio vaccine led to a dramatic decline in polio cases, reducing the annual number from over 20,000 in the early 1950s to fewer than 100 by the mid-1960s.