Improving vaccination rates among the homeless population is a critical public health challenge that requires targeted, compassionate, and accessible strategies. Homeless individuals often face significant barriers to healthcare, including lack of stable housing, limited access to medical facilities, and systemic distrust of institutions. To address these challenges, initiatives must focus on mobile vaccination clinics that bring services directly to shelters, encampments, and community hubs. Building trust through partnerships with local outreach workers and organizations familiar to the homeless community is essential, as is offering incentives such as food, hygiene kits, or transportation assistance. Additionally, simplifying the vaccination process by removing bureaucratic hurdles and providing clear, culturally sensitive information can encourage participation. By combining these approaches, public health efforts can bridge the gap in healthcare access and protect this vulnerable population from preventable diseases.
Explore related products

$16.86 $16.95





What You'll Learn
- Mobile Clinics Accessibility: Deploy mobile clinics to shelters, soup kitchens, and high-traffic homeless areas for easy access
- Trust-Building Strategies: Train healthcare workers to build trust through consistent presence, empathy, and culturally sensitive communication
- Incentives and Support: Offer food, hygiene kits, or transportation vouchers to encourage vaccination participation among the homeless
- Partnerships with Shelters: Collaborate with shelters to integrate vaccination drives into existing health services
- Education and Outreach: Use peer educators and simple, clear messaging to dispel myths and promote vaccine benefits
![]()
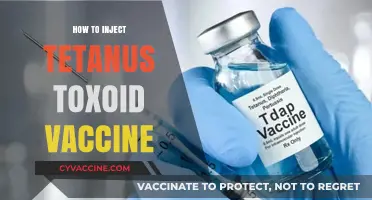
Mobile Clinics Accessibility: Deploy mobile clinics to shelters, soup kitchens, and high-traffic homeless areas for easy access
Homeless individuals often face significant barriers to healthcare, including transportation challenges, lack of identification, and distrust of traditional medical systems. Mobile clinics address these hurdles by bringing services directly to where people are, eliminating the need for them to navigate complex systems or travel long distances. Deploying these clinics to shelters, soup kitchens, and high-traffic homeless areas ensures accessibility while leveraging existing community touchpoints. For instance, a study in San Francisco found that mobile clinics increased vaccination rates among the homeless population by 40% compared to stationary clinics, demonstrating their effectiveness in reaching underserved groups.
To implement this strategy, start by identifying high-need locations through collaboration with local shelters, outreach workers, and community organizations. Equip mobile clinics with essential supplies, including vaccines, refrigeration units, and trained staff capable of administering doses (typically 0.5 mL for intramuscular vaccines like the flu shot). Ensure staff are trained in culturally sensitive communication to build trust with clients, many of whom may have experienced trauma or marginalization. For example, offering vaccines during meal times at soup kitchens or during evening hours at shelters can maximize turnout by aligning with clients’ daily routines.
One critical consideration is the logistical challenge of maintaining vaccine efficacy. Vaccines like the MMR (measles, mumps, rubella) require strict temperature control, typically between 2°C and 8°C. Mobile clinics must invest in portable refrigeration and backup power sources to prevent spoilage. Additionally, offering on-site follow-up appointments for multi-dose vaccines (e.g., hepatitis B requires three doses over six months) can improve completion rates. A successful example is the Boston Healthcare for the Homeless Program, which uses mobile units to provide not only vaccinations but also primary care, mental health services, and substance use treatment, creating a holistic approach to care.
Despite their benefits, mobile clinics face challenges such as funding constraints and staffing shortages. To overcome these, seek partnerships with local health departments, nonprofits, and private donors. For instance, the CDC’s Vaccines for Children program provides free vaccines for eligible populations, reducing financial barriers. Another strategy is to integrate mobile clinics into broader homelessness initiatives, such as Housing First programs, to address health needs alongside housing instability. By combining accessibility with comprehensive care, mobile clinics can serve as a cornerstone of vaccination efforts for homeless populations.
Challenges in Creating a Vaccine for Neisseria Gonorrhea: Unraveling the Complexity
You may want to see also
Explore related products






![]()
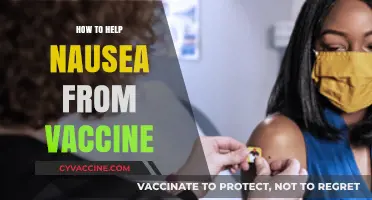
Trust-Building Strategies: Train healthcare workers to build trust through consistent presence, empathy, and culturally sensitive communication
Homeless individuals often face systemic barriers to healthcare, including vaccination, due to mistrust rooted in past experiences of marginalization and inconsistent care. Building trust requires more than a single interaction; it demands a sustained, empathetic approach tailored to their unique needs. Training healthcare workers to establish consistent presence, demonstrate genuine empathy, and communicate in a culturally sensitive manner can bridge this trust gap, making vaccination efforts more effective and humane.
Consider the steps involved in implementing this strategy. First, healthcare workers must commit to regular, predictable visits to shelters, drop-in centers, or encampments. Consistency signals reliability, a rare commodity in the lives of many homeless individuals. For example, a weekly vaccination clinic at a shelter, staffed by the same team, fosters familiarity and reduces anxiety. Pair this with clear, accessible communication about vaccine benefits, potential side effects, and follow-up care. Use plain language and visual aids, avoiding medical jargon that can alienate or confuse. For instance, explain that the COVID-19 vaccine reduces severe illness risk by 90% and that mild side effects like fatigue typically resolve within 48 hours.
Empathy is equally critical. Healthcare workers should be trained to listen actively, acknowledge the challenges faced by homeless individuals, and validate their concerns without judgment. For example, if someone expresses fear of vaccines due to past medical mistreatment, respond with phrases like, “I understand your hesitation. Many people feel that way. Let’s talk about what’s worrying you.” This approach humanizes the interaction and builds rapport. Additionally, incorporate harm reduction principles by offering vaccines without requiring identification or insurance, removing barriers that often deter this population.
Culturally sensitive communication is the final pillar. Recognize that homeless populations are diverse, with varying backgrounds, languages, and beliefs. Train healthcare workers to adapt their approach accordingly. For instance, in communities with high Indigenous representation, incorporate traditional healing practices or involve cultural liaisons to enhance trust. In multilingual populations, provide translated materials and interpreters. For example, a Spanish-speaking healthcare worker explaining the flu vaccine’s 40-60% efficacy rate in preventing illness can make the information more relatable and actionable.
In conclusion, trust-building strategies for vaccinating homeless individuals require intentionality, humility, and adaptability. By training healthcare workers to maintain a consistent presence, practice empathy, and communicate culturally sensitively, we can dismantle barriers to care and improve health outcomes. This approach not only increases vaccination rates but also restores dignity and trust in a system that has often failed this vulnerable population.
Does Walgreens Offer the RSV Vaccine? Availability and Details
You may want to see also
Explore related products






![]()
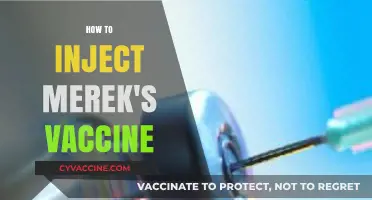
Incentives and Support: Offer food, hygiene kits, or transportation vouchers to encourage vaccination participation among the homeless
Homeless individuals often face barriers to accessing healthcare, including vaccinations, due to logistical challenges, lack of trust, and immediate survival needs. Offering tangible incentives like food, hygiene kits, or transportation vouchers can address these barriers by meeting basic needs while encouraging vaccination participation. For instance, a hot meal or a hygiene kit containing essentials like soap, toothpaste, and a toothbrush can provide immediate relief, making the vaccination process more appealing. Similarly, transportation vouchers can help overcome mobility issues, ensuring individuals can reach vaccination sites without added stress.
Analyzing the effectiveness of these incentives reveals their dual purpose: they not only motivate participation but also build trust and rapport with the homeless community. Studies show that when healthcare services are paired with immediate, practical support, individuals are more likely to engage. For example, a program in San Francisco distributed hygiene kits alongside COVID-19 vaccines, resulting in a 30% increase in vaccination rates among the homeless population. This approach acknowledges the reality that for many, the decision to get vaccinated is secondary to securing food or shelter, making incentives a critical bridge to healthcare access.
Implementing such programs requires careful planning. First, partner with local shelters, food banks, or outreach organizations to distribute incentives during vaccination drives. Ensure the items offered are culturally appropriate and meet real needs—for example, providing non-perishable food items or gender-specific hygiene products. Transportation vouchers should be flexible, covering public transit or ride-sharing services, and clearly explain how to use them. Additionally, train staff to communicate the value of vaccination in a non-judgmental, empathetic manner, emphasizing that the incentives are a token of support, not a bribe.
A comparative look at successful programs highlights the importance of tailoring incentives to local contexts. In cities with harsh winters, adding warm clothing or blankets to hygiene kits can increase participation. In rural areas, where transportation is a significant barrier, offering gas vouchers or arranging shuttle services may be more effective. The key is to listen to the community’s needs and adapt accordingly. For instance, a program in Seattle found that offering bus passes alongside flu vaccines increased uptake by 25%, while another in Houston saw greater success with food vouchers.
In conclusion, incentives like food, hygiene kits, and transportation vouchers are not just rewards—they are tools of empowerment. By addressing immediate needs, they remove barriers to vaccination and foster a sense of dignity and care. For healthcare providers and policymakers, the takeaway is clear: investing in these small but impactful supports can yield significant returns in public health, particularly for marginalized populations. Practical, compassionate strategies like these are essential to ensuring equitable access to life-saving vaccines.
Hepatitis A Vaccinations: Avoiding Neosporin
You may want to see also
Explore related products





![]()
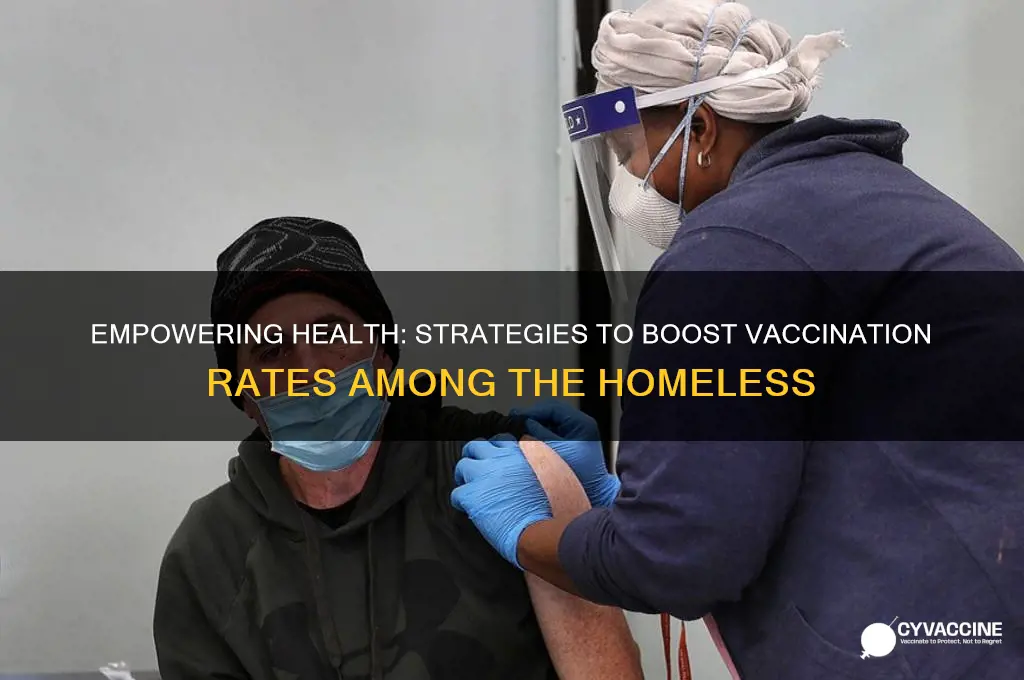
Partnerships with Shelters: Collaborate with shelters to integrate vaccination drives into existing health services
Shelters often serve as a critical lifeline for homeless individuals, providing not only shelter but also access to essential health services. By integrating vaccination drives into these existing frameworks, shelters can become hubs for preventive care, addressing a gap in healthcare access for this vulnerable population. This approach leverages the trust and familiarity homeless individuals may already have with shelter staff, making vaccination more approachable and less intimidating.
For instance, a shelter in Seattle partnered with a local health department to offer flu shots during their weekly medical clinics. Nurses administered the vaccine alongside routine check-ups, ensuring a seamless and non-disruptive experience for residents. This model, which can be replicated for other vaccines like COVID-19 or Hepatitis A, highlights the importance of embedding vaccination within established routines.
However, successful integration requires careful planning. Shelters must ensure sufficient staffing and resources to handle the additional workload. Training shelter staff to address common concerns and misconceptions about vaccines is crucial. Offering incentives like small gifts or snacks can further encourage participation. Additionally, shelters should collaborate with healthcare providers to ensure proper storage and handling of vaccines, especially those requiring refrigeration.
A key advantage of this approach is its ability to reach a concentrated population. Shelters often house individuals with higher risk factors for vaccine-preventable diseases due to crowded living conditions and limited access to hygiene facilities. By targeting these settings, vaccination drives can have a significant impact on disease prevention within the homeless community.
Ultimately, partnering with shelters to integrate vaccination drives into existing health services offers a practical and effective strategy for improving vaccination rates among the homeless. This model capitalizes on existing infrastructure, builds on established trust, and addresses logistical challenges associated with reaching this population. By working collaboratively, shelters and healthcare providers can create a more equitable and accessible healthcare system, protecting the health and well-being of those most in need.
Did Pasteur Invent the Term 'Vaccine'? Unraveling the Origins
You may want to see also
Explore related products






![]()
Education and Outreach: Use peer educators and simple, clear messaging to dispel myths and promote vaccine benefits
Homeless individuals often face barriers to vaccination due to misinformation, distrust of institutions, and lack of accessible health education. Peer educators—individuals with lived experience of homelessness—can bridge this gap by delivering messages in a relatable, empathetic manner. For instance, a peer educator might share their own decision-making process about getting vaccinated, addressing common fears like side effects or government tracking. This approach humanizes the conversation, making it more likely to resonate with the target audience. Pairing peer educators with simple, clear messaging ensures that vaccine benefits are communicated effectively, without overwhelming or alienating those who may have limited health literacy.
Consider the following steps to implement this strategy: first, recruit and train peer educators from within the homeless community, focusing on active listening, myth-busting techniques, and concise communication. Provide them with key talking points, such as the fact that COVID-19 vaccines reduce severe illness by over 90% and that side effects like fatigue or soreness typically last only 1–2 days. Second, equip these educators with visual aids, such as infographics or short videos, that use plain language and avoid medical jargon. For example, a poster could compare the risk of blood clots from COVID-19 (1 in 1,000) to the risk from vaccines (1 in 1 million), making the benefits clear. Third, deploy peer educators to shelters, soup kitchens, and street outreach programs, where they can engage in one-on-one or small group conversations.
One caution: while peer educators are powerful messengers, they must be supported with accurate, up-to-date information. Regular training sessions with healthcare professionals can ensure they stay informed about vaccine efficacy, safety, and evolving guidelines. Additionally, avoid overloading them with complex data; instead, focus on 2–3 core messages, such as "Vaccines save lives," "Side effects are temporary," and "Getting vaccinated protects your community." This approach prevents confusion and keeps the message actionable.
A compelling example of this strategy in action is the San Francisco Department of Public Health’s partnership with homeless advocacy groups. Peer educators distributed vaccine information alongside hygiene kits, using conversations about health to naturally introduce the topic of vaccination. By framing vaccines as a tool for personal and communal resilience, they achieved a 20% increase in vaccination rates among homeless adults within six months. This model demonstrates that combining trusted messengers with clear, tailored messaging can overcome hesitancy and build confidence in vaccines.
In conclusion, education and outreach through peer educators and simple messaging are not just theoretical solutions—they are proven strategies for improving vaccination rates among homeless populations. By leveraging shared experiences and straightforward communication, these efforts dismantle barriers and empower individuals to make informed choices. For organizations looking to implement this approach, start small: train 2–3 peer educators, focus on high-traffic areas, and measure success through surveys or vaccination data. With persistence and adaptability, this method can transform skepticism into trust, one conversation at a time.
Orthodox Jewish Vaccine Hesitancy: Exploring Cultural and Religious Perspectives
You may want to see also
Frequently asked questions
Effective strategies include mobile vaccination clinics, partnerships with shelters and outreach programs, offering incentives like food or hygiene kits, and training staff to address vaccine hesitancy with empathy and culturally sensitive communication.
Building trust involves consistent presence from trusted community organizations, involving peer advocates who have experienced homelessness, providing clear and transparent information, and ensuring services are non-judgmental and respectful.
Shelters and service providers can host on-site vaccination clinics, educate residents about vaccine benefits, assist with scheduling and transportation, and integrate vaccination into existing health services to make it more accessible.
Addressing hesitancy requires understanding specific concerns, providing accurate information in simple language, debunking myths, and offering one-on-one counseling with healthcare workers or peer educators to build confidence in vaccines.