The rollout of COVID-19 vaccines has been a critical aspect of global efforts to combat the pandemic, but the pace and efficiency of distribution have varied significantly across states and countries. Factors such as supply chain logistics, healthcare infrastructure, public trust, and policy decisions have played pivotal roles in determining how quickly and effectively vaccines have reached populations. Comparing vaccine rollout strategies and outcomes among states highlights disparities in access, prioritization, and administration, offering valuable insights into best practices and areas for improvement. These comparisons not only shed light on the challenges faced by individual regions but also underscore the importance of equitable distribution and coordinated global efforts in achieving widespread immunity.
Explore related products






What You'll Learn
- Vaccine Distribution Strategies: Comparing state-level approaches to equitable vaccine allocation and delivery methods
- Vaccination Rates by State: Analyzing disparities in vaccination completion rates across different states
- Logistical Challenges: Examining supply chain, storage, and workforce hurdles in state rollouts
- Public Trust and Hesitancy: Assessing how state-specific campaigns address vaccine skepticism and misinformation
- Policy and Mandates: Comparing state-level vaccine requirements and their impact on uptake
![]()
Vaccine Distribution Strategies: Comparing state-level approaches to equitable vaccine allocation and delivery methods
The COVID-19 vaccine rollout in the United States has been a complex, state-driven process, revealing a patchwork of strategies aimed at equitable allocation and efficient delivery. Some states, like California, adopted a phased approach prioritizing healthcare workers, seniors, and essential workers, while others, such as Alaska, opted for a more age-based strategy, opening eligibility to all residents over 65 early on. These differing approaches highlight the tension between speed and fairness, as well as the influence of local demographics and infrastructure on distribution methods.
Consider the logistical challenges of delivering vaccines to rural areas versus urban centers. States like Montana and Wyoming, with vast rural populations, utilized mobile clinics and partnerships with local pharmacies to ensure accessibility. In contrast, densely populated states like New York and Illinois leaned heavily on mass vaccination sites, such as stadiums and convention centers, capable of administering thousands of doses daily. For instance, New York’s Javits Center administered over 10,000 doses per day at its peak, while Montana’s mobile units focused on smaller, targeted outreach, often administering 50–100 doses per stop. These methods underscore the importance of tailoring delivery systems to local needs.
Equity in vaccine allocation has been a central concern, with many states implementing strategies to address disparities. For example, North Carolina launched a data-driven approach, using the CDC’s Social Vulnerability Index to identify and prioritize underserved communities. Similarly, Michigan allocated additional doses to counties with higher COVID-19 mortality rates, ensuring that areas hardest hit received proportional resources. Practical tips for states aiming to replicate these efforts include leveraging existing health equity frameworks, partnering with community organizations for outreach, and offering multilingual resources to bridge communication gaps.
A comparative analysis reveals that states with centralized, data-informed systems tended to achieve higher vaccination rates among vulnerable populations. For instance, Connecticut’s use of a statewide pre-registration system streamlined appointments and reduced confusion, while Texas’s decentralized approach led to early bottlenecks. States considering improvements should focus on integrating real-time data into decision-making, ensuring transparency in allocation criteria, and providing clear, actionable instructions for residents, such as specifying required documents for appointments and offering second-dose reminders.
Ultimately, the success of vaccine distribution hinges on adaptability and collaboration. States that combined top-down coordination with bottom-up community engagement, like Massachusetts and Oregon, demonstrated resilience in addressing emerging challenges. By studying these examples, policymakers can refine strategies to balance speed, equity, and accessibility, ensuring that future public health initiatives are both efficient and just.
Unveiling the True Purpose of Vaccines: Beyond Disease Prevention
You may want to see also
Explore related products






![]()
Vaccination Rates by State: Analyzing disparities in vaccination completion rates across different states
The COVID-19 vaccine rollout in the United States has revealed striking disparities in vaccination completion rates across states. As of recent data, states like Vermont and Connecticut boast vaccination rates exceeding 75% for eligible populations, while others, such as Mississippi and Alabama, lag behind at around 50%. This gap highlights the complex interplay of factors influencing vaccine uptake, from socioeconomic conditions to political leanings and public health infrastructure. Understanding these variations is crucial for tailoring strategies to bridge the divide and ensure equitable health outcomes nationwide.
One key factor driving these disparities is the urban-rural divide. Urban states with dense populations and robust healthcare systems, like Massachusetts and California, have generally achieved higher vaccination rates due to better access to vaccine sites and stronger public health campaigns. In contrast, rural states face challenges such as limited healthcare facilities, longer travel distances, and lower population density, which hinder efficient vaccine distribution. For instance, in Wyoming, only 45% of the eligible population has completed vaccination, compared to 70% in New York. Addressing this gap requires targeted solutions, such as mobile vaccination clinics and partnerships with local pharmacies in underserved areas.
Another critical aspect is the role of political and cultural attitudes toward vaccination. States with higher skepticism or resistance to vaccines, often correlated with conservative political leanings, have seen slower uptake. For example, in Idaho and Montana, misinformation and distrust in government mandates have contributed to vaccination rates below 50%. Conversely, states with strong public health messaging and community engagement, like Maine and Oregon, have achieved higher compliance. Public health officials can combat this by collaborating with local leaders and trusted figures to disseminate accurate information and build confidence in vaccines.
Age and demographic factors also play a significant role in vaccination disparities. While most states have prioritized elderly populations, younger age groups have shown lower vaccination rates, particularly in states with large youth populations. In Florida, for instance, only 40% of individuals aged 18-29 have completed their vaccine series, compared to 85% of those over 65. Encouraging younger demographics to get vaccinated requires creative approaches, such as pop-up clinics at colleges, incentives like gift cards, and social media campaigns tailored to their preferences.
To address these disparities effectively, states must adopt a multi-faceted approach. First, allocate resources to areas with the lowest vaccination rates, focusing on accessibility and convenience. Second, leverage data to identify and target specific demographics with tailored messaging. Third, foster partnerships between state governments, local organizations, and private sectors to amplify outreach efforts. By learning from high-performing states and adapting strategies to local contexts, the U.S. can narrow the vaccination gap and protect more communities from preventable diseases.
Are New Vaccines FDA Approved? Understanding Emergency Use Authorization
You may want to see also
Explore related products

$20.46 $21.95





![]()
Logistical Challenges: Examining supply chain, storage, and workforce hurdles in state rollouts
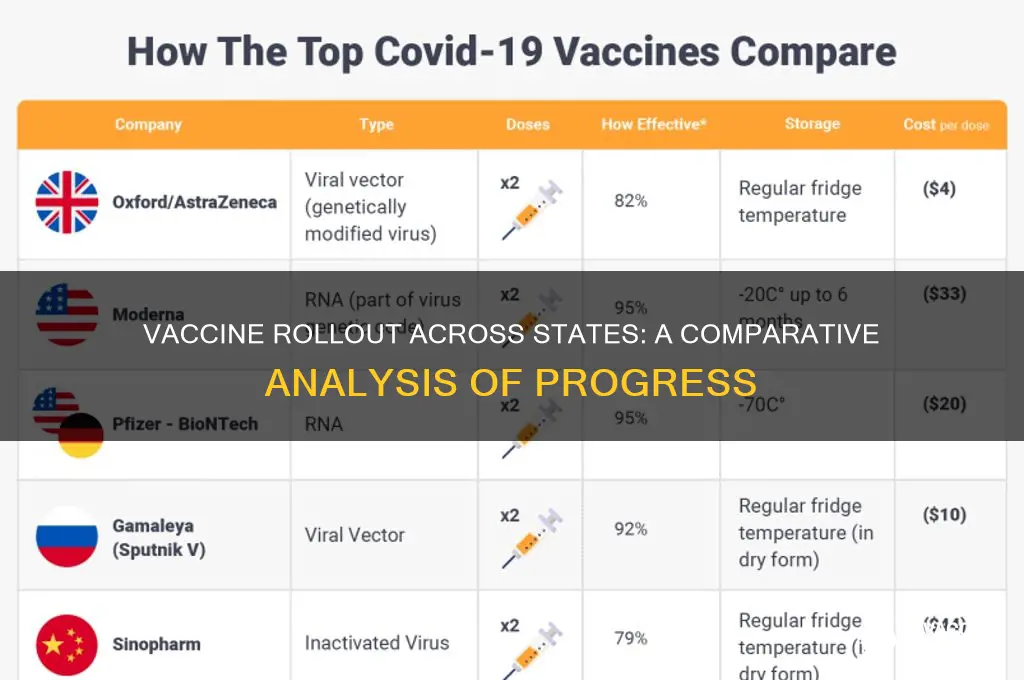
The success of a vaccine rollout hinges on a delicate logistical ballet, and states are discovering that even the smallest misstep can lead to significant delays. Consider the Pfizer-BioNTech vaccine, which requires ultra-cold storage at -70°C. This presents a unique challenge for states with limited access to specialized freezers, particularly in rural areas. For instance, Alaska, with its vast geography and dispersed population, had to invest in portable ultra-cold storage units and develop a distribution network capable of reaching remote communities. This example highlights the critical interplay between supply chain infrastructure and the specific requirements of different vaccines.
A well-orchestrated vaccine rollout demands a robust supply chain, meticulous storage solutions, and a dedicated workforce. Imagine a complex relay race where the baton is a vial of vaccine, passing through manufacturers, distributors, storage facilities, and finally, into the arms of citizens. Each handoff requires precision and coordination. States with established cold chain infrastructure, like California with its extensive network of medical distributors, have an advantage in this race. They can leverage existing systems to ensure vaccines remain viable during transport and storage.
However, the challenges don't end with storage. Workforce shortages plague many states, particularly in rural areas. Administering vaccines requires trained personnel, from pharmacists and nurses to support staff managing registration and observation. States like Mississippi, with a high proportion of rural residents, face the dual challenge of attracting healthcare workers to underserved areas and ensuring they have the necessary training for vaccine administration. This highlights the need for creative solutions, such as deploying mobile vaccination units staffed by traveling medical teams or partnering with community health centers.
The logistical hurdles of vaccine rollout are not insurmountable, but they demand proactive planning and innovative solutions. States must assess their unique vulnerabilities and strengths. Those with limited cold chain capacity might prioritize vaccines with less stringent storage requirements, like the Johnson & Johnson vaccine, which can be stored at standard refrigerator temperatures. Others might invest in training programs to expand their healthcare workforce, offering incentives to attract professionals to underserved areas. By addressing these logistical challenges head-on, states can ensure a smoother and more equitable vaccine distribution, ultimately protecting their citizens and contributing to the global effort to end the pandemic.
Meningitis Vaccine for 6-Month-Olds: Live or Not?
You may want to see also
Explore related products






![]()
Public Trust and Hesitancy: Assessing how state-specific campaigns address vaccine skepticism and misinformation
Vaccine hesitancy is not a monolithic issue; it varies widely by region, influenced by local cultures, histories, and information ecosystems. States with successful rollout campaigns often tailor their strategies to address specific concerns within their populations. For instance, California’s *Community Immunity* initiative partnered with trusted local leaders—religious figures, teachers, and healthcare workers—to debunk myths about vaccine side effects and efficacy. By contrast, Mississippi, a state with historically low vaccination rates, focused on simplifying access by offering mobile clinics in rural areas and emphasizing the safety of the 0.5 mL pediatric Pfizer dose for children aged 5–11. These state-specific approaches highlight the importance of understanding local skepticism to build trust effectively.
Consider the role of messaging in combating misinformation. In Vermont, where hesitancy was fueled by online conspiracy theories, the state launched a digital literacy campaign teaching residents to identify unreliable sources. This included workshops on fact-checking tools and a hotline for verifying vaccine information. Meanwhile, Texas, grappling with political polarization, framed vaccination as a matter of personal freedom and community responsibility, avoiding divisive language. Such strategies demonstrate that addressing hesitancy requires not just factual correction but also an understanding of the emotional and ideological drivers behind skepticism.
A critical takeaway is the need for flexibility and adaptability in campaign design. For example, New York’s *Vax4NY* program initially struggled to reach minority communities due to historical medical mistrust. In response, the state shifted to hyper-local outreach, using multilingual materials and hosting town halls in underserved neighborhoods. Similarly, Oregon’s campaign incorporated storytelling, sharing personal narratives of vaccinated individuals to humanize the issue. These examples underscore that one-size-fits-all approaches often fail; success hinges on meeting communities where they are, both physically and psychologically.
Practical tips for state health departments include leveraging data to identify hesitancy hotspots and tailoring interventions accordingly. For instance, if a county shows high engagement with anti-vaccine social media, counter with targeted ads featuring local success stories. Additionally, ensure that all campaigns provide clear, actionable information—such as the recommended two-dose schedule for Moderna (4 weeks apart) or the single-dose convenience of Johnson & Johnson. By combining empathy, evidence, and specificity, states can dismantle barriers to trust and foster a more resilient public health response.
Gardasil Vaccine Launch in Australia: A Timeline of Introduction
You may want to see also
![]()
Policy and Mandates: Comparing state-level vaccine requirements and their impact on uptake
The patchwork of state-level vaccine mandates has created a natural experiment in public health policy, with wide variations in requirements and, consequently, uptake. Some states, like California, have implemented strict mandates for schoolchildren, requiring all students to receive vaccines such as MMR (measles, mumps, rubella) and Tdap (tetanus, diphtheria, pertussis) unless they have a medical exemption. In contrast, states like Idaho allow exemptions for both medical and philosophical reasons, leading to lower vaccination rates. For instance, California’s kindergarten MMR coverage stands at 95%, while Idaho’s hovers around 86%, according to CDC data. This disparity highlights how policy rigor directly correlates with community immunity.
Consider the COVID-19 vaccine rollout, where state mandates for healthcare workers or government employees have sharply divided outcomes. New York’s mandate for healthcare workers, implemented in late 2021, saw compliance rates exceed 98%, with minimal workforce disruption despite initial resistance. Conversely, Florida’s prohibition on vaccine mandates led to lower uptake among similar demographics, with only 75% of healthcare workers fully vaccinated by early 2022. These examples underscore the power of mandates to shape behavior, but also reveal the importance of clear communication and enforcement mechanisms. For policymakers, the lesson is clear: mandates work, but only when paired with accessible resources and public trust.
A comparative analysis of age-specific mandates further illustrates their impact. In states like Mississippi and West Virginia, which require all schoolchildren to receive the full CDC-recommended vaccine schedule (including doses for polio, varicella, and hepatitis B), vaccine-preventable diseases are nearly nonexistent. Mississippi, for example, has a 99.4% compliance rate for the DTaP vaccine among kindergartners, one of the highest in the nation. Meanwhile, states with lenient policies, such as Oregon, where non-medical exemptions are easily obtained, report recurring outbreaks of diseases like pertussis. This suggests that stringent policies not only protect individuals but also safeguard public health by maintaining herd immunity thresholds.
For those navigating state-specific mandates, practical tips can ease compliance. First, verify your state’s requirements early; many school systems have deadlines for submitting vaccination records. Second, leverage local health departments or clinics for low-cost or free vaccines, particularly if you’re uninsured. Third, document all doses meticulously—some states require proof of specific lot numbers or administration dates. Finally, if seeking an exemption, understand the legal criteria; in states like California, medical exemptions must be signed by a licensed physician and often require detailed justification. Proactive steps like these can prevent last-minute hurdles and ensure adherence to state policies.
Ultimately, the impact of state-level mandates on vaccine uptake is a testament to the interplay between policy and public behavior. While mandates can drive compliance, their success hinges on factors like accessibility, enforcement, and community buy-in. States with robust mandates and supportive infrastructure, such as New York’s COVID-19 vaccine clinics or Mississippi’s school-based immunization programs, consistently outperform those with fragmented or permissive policies. As vaccine-preventable diseases persist and new threats emerge, the lessons from these state-level comparisons offer a roadmap for balancing individual choice with collective health imperatives.
Can Vaccines Reduce Appetite and Manage Diabetes Symptoms Effectively?
You may want to see also
Frequently asked questions
As of recent data, states like Vermont, Massachusetts, and Connecticut consistently rank among the highest in vaccination rates, with over 75% of their populations fully vaccinated.
Rural states often face challenges like lower vaccine uptake due to hesitancy, limited access to healthcare facilities, and logistical hurdles, while urban states typically have higher vaccination rates due to better infrastructure and denser populations.
Key factors include differences in state policies, vaccine hesitancy, healthcare infrastructure, population density, and socioeconomic disparities, which can significantly impact rollout efficiency.
Blue states generally have higher vaccination rates due to more supportive policies and lower levels of vaccine hesitancy, while red states often lag behind due to political and cultural factors influencing public health decisions.
States like California and New York have implemented targeted strategies to ensure equitable distribution, focusing on underserved communities, while others struggle with disparities based on race, income, and geography.