Hepatitis A is a highly contagious liver infection caused by the hepatitis A virus, typically spread through contaminated food or water or close contact with an infected person. Vaccination is the most effective way to prevent this disease, and the hepatitis A vaccine is administered in a series of shots to ensure long-term immunity. The standard schedule for the hepatitis A vaccine involves two doses, with the second dose given 6 to 18 months after the first. This interval is crucial for building robust and lasting protection against the virus. Understanding the timing between doses is essential for maximizing the vaccine’s effectiveness and ensuring individuals are fully safeguarded against hepatitis A.
| Characteristics | Values |
|---|---|
| Vaccine Type | Hepatitis A vaccine (inactivated) |
| Primary Series Schedule | 2 doses |
| Interval Between Doses | 6 to 18 months (minimum 6 months between doses) |
| Age for First Dose | 12 months or older |
| Booster Dose | Not routinely needed for immunocompetent individuals |
| Duration of Protection | Long-term (at least 20 years, possibly lifelong) |
| Special Populations | - Travelers to endemic areas: Accelerated schedule (0, 6-12 months) |
| - Immunocompromised individuals: May require additional doses | |
| Vaccine Brands | Havrix, Vaqta (commonly used in the U.S.) |
| Side Effects | Mild: Soreness at injection site, headache, fatigue, loss of appetite |
| Contraindications | Severe allergic reaction to a previous dose or vaccine component |
| Pregnancy and Breastfeeding | Safe during pregnancy and breastfeeding if risk of exposure is high |
| Storage Requirements | Refrigerated at 2°C to 8°C (36°F to 46°F) |
| Global Recommendations | Varies by country; routine vaccination in high-risk areas |
| Post-Exposure Prophylaxis | Administer vaccine within 2 weeks of exposure, or IG if indicated |
Explore related products






What You'll Learn
- Recommended Dosing Schedule: Standard intervals between initial and booster doses for optimal immunity
- Age-Specific Timing: Vaccination frequency varies by age group, from children to adults
- Travel Requirements: Accelerated schedules for travelers to high-risk hepatitis A regions
- Immune Status Impact: Adjusted intervals for immunocompromised individuals needing additional protection
- Combination Vaccines: Timing when hepatitis A is paired with other vaccines (e.g., hepatitis B)
![]()
Recommended Dosing Schedule: Standard intervals between initial and booster doses for optimal immunity
The recommended dosing schedule for the hepatitis A vaccine is designed to ensure optimal immunity against the virus. For individuals aged 1 year and older, the standard regimen involves two doses of the vaccine. The initial dose is administered at the first visit, followed by a booster dose to enhance and prolong immunity. The timing of this booster is crucial for achieving the best protective effect. Typically, the second dose is given 6 to 18 months after the first dose. This interval allows the immune system to develop a robust response to the initial vaccine before reinforcing it with the booster. Adhering to this schedule ensures that the body builds and maintains sufficient antibodies to combat hepatitis A effectively.
For children, the hepatitis A vaccine is often administered as part of routine immunizations. The first dose is usually given between 12 and 23 months of age, followed by the booster dose 6 to 18 months later. This timing aligns with other childhood vaccinations, making it convenient for parents and healthcare providers. It is important to note that the minimum interval between doses should not be less than 6 months, as shorter intervals may reduce the vaccine's effectiveness. If the booster dose is delayed beyond the recommended timeframe, it can still be administered without the need to restart the series, ensuring flexibility in scheduling.
Adults and older children who were not vaccinated earlier can also receive the hepatitis A vaccine. The same two-dose schedule applies, with the doses administered 6 to 18 months apart. Travelers to regions with high rates of hepatitis A are often advised to complete the vaccine series before departure, but if time is limited, an accelerated schedule may be considered. In such cases, the booster dose can be given as early as 6 months after the initial dose, though the standard interval remains the preferred option for long-term immunity.
In certain situations, such as outbreaks or high-risk exposures, an immune globulin (IG) shot may be given along with the hepatitis A vaccine. However, this does not alter the standard dosing schedule for the vaccine itself. It is essential to follow the recommended intervals to ensure the vaccine's full efficacy. Healthcare providers should document the vaccination dates and remind patients of their booster appointments to maintain compliance with the schedule.
For individuals with compromised immune systems, the standard dosing schedule remains applicable, but the vaccine's effectiveness may vary. In such cases, additional precautions or monitoring may be recommended. Regardless of the individual's health status, the 6 to 18 month interval between doses is critical for achieving optimal immunity. This schedule has been extensively studied and validated, providing a reliable framework for hepatitis A prevention. By adhering to these guidelines, individuals can significantly reduce their risk of infection and contribute to broader public health goals.
Chickenpox Vaccine: Egg-Free or Not?
You may want to see also
Explore related products






![]()
Age-Specific Timing: Vaccination frequency varies by age group, from children to adults
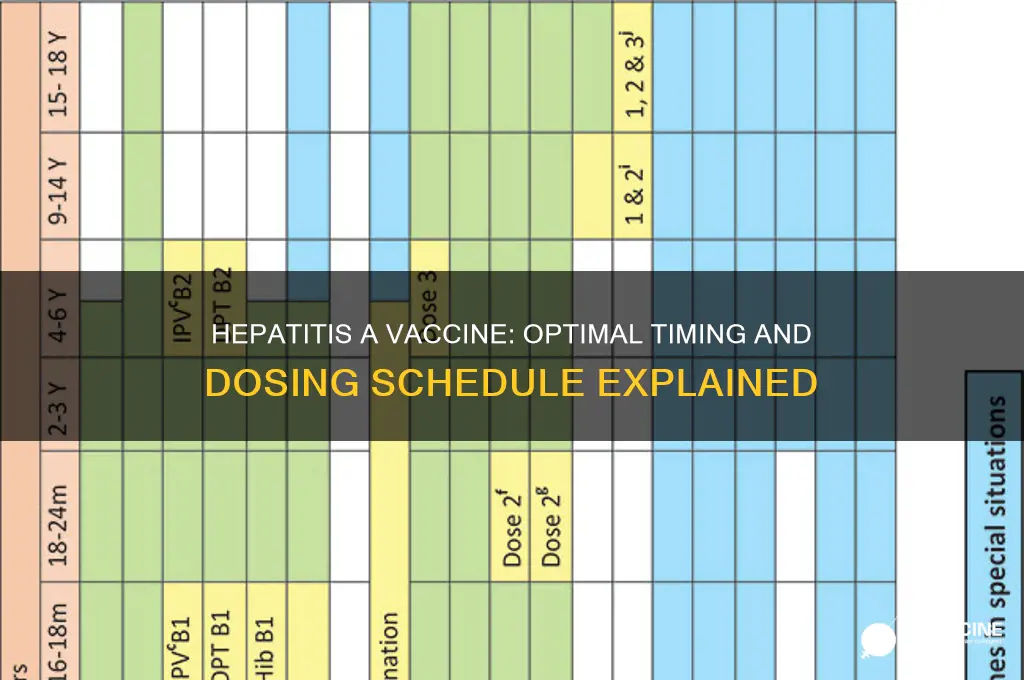
The timing and frequency of Hepatitis A vaccination differ significantly across age groups, reflecting varying levels of risk and immune response. For infants and young children, the Centers for Disease Control and Prevention (CDC) recommends the first dose of the Hepatitis A vaccine at 12 months of age, followed by a second dose 6 to 18 months later. This two-dose schedule ensures robust immunity during childhood, a period when exposure risks may increase due to daycare or school environments. The interval between doses is crucial for maximizing antibody production, with studies showing that a gap of at least 6 months provides optimal protection.
For older children and adolescents who were not vaccinated earlier, the same two-dose series applies, but the timing can be more flexible. The first dose can be administered at any point, with the second dose following 6 to 18 months later. This age group often receives the vaccine as part of catch-up immunization efforts, especially before traveling to regions with high Hepatitis A prevalence or during outbreaks. Adhering to the recommended interval ensures long-term immunity, reducing the risk of infection during teenage years and early adulthood.
Adults seeking Hepatitis A vaccination follow a similar two-dose regimen, but the urgency and context often differ. The first dose is given at the initial visit, with the second dose administered 6 to 12 months later. This schedule is particularly important for adults at higher risk, such as travelers, men who have sex with men, people with chronic liver disease, or those experiencing homelessness. Unlike children, adults may require expedited vaccination if traveling imminently; in such cases, the second dose can be given 6 months later, but not earlier, to ensure adequate immune response.
Special populations, such as immunocompromised individuals or those with specific medical conditions, may require tailored vaccination schedules. For example, people living with HIV or those undergoing chemotherapy might need additional doses or closer monitoring to ensure immunity. Healthcare providers often assess these cases individually, balancing the need for protection with the individual's health status. Regardless of age, the principle remains consistent: the interval between doses is critical for achieving and maintaining immunity against Hepatitis A.
In summary, the frequency of Hepatitis A vaccination is age-specific, with a standard two-dose series spaced 6 to 18 months apart for all age groups. While the core schedule remains consistent, adjustments are made based on age, risk factors, and individual health conditions. Adhering to these guidelines ensures that individuals across the lifespan receive the maximum benefit from the vaccine, reducing the global burden of Hepatitis A infections.
Eli Lilly's Monkey Source for Polio Vaccine
You may want to see also
Explore related products

$11.93 $21.99





![]()
Travel Requirements: Accelerated schedules for travelers to high-risk hepatitis A regions
For travelers planning to visit regions with high endemic rates of hepatitis A, adhering to an accelerated vaccination schedule is crucial to ensure protection before departure. The standard hepatitis A vaccine schedule typically involves two doses administered 6 to 12 months apart. However, this timeline may not align with urgent travel plans. In such cases, an accelerated schedule can be implemented, where the second dose is given as early as 6 months after the first dose, but ideally, it can be administered at a minimum interval of 6 months to ensure optimal immunity. This flexibility allows travelers to achieve protection within a shorter timeframe, reducing the risk of contracting hepatitis A during their trip.
Travelers should consult a healthcare provider or travel clinic at least 4 to 6 weeks before departure to discuss their vaccination needs. During this consultation, the provider will assess the traveler’s health status, destination-specific risks, and the urgency of their travel plans. If an accelerated schedule is deemed necessary, the first dose of the hepatitis A vaccine will be administered immediately. This initial dose provides partial protection, but it is the second dose that ensures long-term immunity. For those traveling to high-risk areas, combining the hepatitis A vaccine with immune globulin (IG) may be recommended for additional short-term protection, especially if travel is imminent and the full vaccine series cannot be completed beforehand.
It is important to note that the accelerated schedule does not compromise the vaccine’s effectiveness when doses are administered at least 6 months apart. However, delaying the second dose beyond 12 months may reduce the vaccine’s long-term efficacy. Travelers should prioritize receiving the second dose as close to the 6-month mark as possible to ensure sustained immunity. Additionally, maintaining good hygiene practices, such as frequent handwashing and avoiding contaminated food and water, complements the vaccine’s protection while traveling in high-risk regions.
For individuals traveling with children, the hepatitis A vaccine is approved for use in children as young as 12 months. The accelerated schedule applies to children as well, ensuring they are protected before travel. Parents should plan ahead and consult a pediatrician to ensure their child’s vaccination schedule aligns with travel dates. In some cases, combining the hepatitis A vaccine with other routine childhood immunizations may be possible, streamlining the process for families.
Lastly, travelers should be aware that proof of hepatitis A vaccination may be required for entry into certain countries or for specific activities, such as volunteering in healthcare settings. Carrying a vaccination record or International Certificate of Vaccination or Prophylaxis (ICVP) is advisable. By following an accelerated schedule and staying informed about travel requirements, individuals can safeguard their health and enjoy their journey to high-risk hepatitis A regions with peace of mind.
Vaccine Safety: No Carcinogenic or Mutagenic Concerns
You may want to see also
Explore related products






![]()
Immune Status Impact: Adjusted intervals for immunocompromised individuals needing additional protection
For immunocompromised individuals, the standard hepatitis A vaccine schedule may not provide sufficient protection due to their reduced immune response. Typically, the hepatitis A vaccine is administered in two doses, with the second dose given 6 to 12 months after the first. However, those with weakened immune systems often require an adjusted vaccination strategy to ensure optimal immunity. This is because immunocompromised individuals, such as organ transplant recipients, HIV patients, or those undergoing chemotherapy, may not produce enough antibodies from the standard vaccine regimen.
The impact of immune status on vaccine efficacy is a critical consideration. Studies suggest that immunocompromised patients might benefit from a shorter interval between doses to enhance their immune response. For instance, a modified schedule could involve administering the second dose after 1 to 2 months, followed by a third dose 6 to 12 months later. This accelerated schedule aims to boost antibody production and provide better protection against hepatitis A, which is crucial for this vulnerable population.
Adjusting the vaccine intervals is a strategic approach to compensate for the compromised immune system's limitations. By reducing the time between doses, the immune system is stimulated more frequently, potentially leading to a stronger and more sustained response. This is particularly important for hepatitis A prevention, as the virus can cause severe complications in immunocompromised individuals, including liver failure.
Furthermore, healthcare providers should consider additional measures to ensure the vaccine's effectiveness. This may include monitoring antibody levels post-vaccination and offering booster doses as needed. Regular assessment of immune status and hepatitis A antibody titers can help determine the necessity for further vaccinations. Personalized vaccine schedules, tailored to the individual's immune response, are essential to achieving adequate protection.
In summary, immunocompromised individuals require a tailored approach to hepatitis A vaccination, often involving shorter intervals between doses and additional booster shots. This adjusted strategy aims to overcome the challenges posed by a weakened immune system, ensuring better protection against hepatitis A infection and its potential complications. Healthcare professionals play a vital role in assessing and managing these customized vaccination plans.
Vaccination's Lifesaving Legacy: Counting Lives Saved Since Edward Jenner
You may want to see also
Explore related products






![]()
Combination Vaccines: Timing when hepatitis A is paired with other vaccines (e.g., hepatitis B)
Combination vaccines offer a convenient and efficient way to protect against multiple diseases with fewer injections. When hepatitis A (HepA) is paired with other vaccines, such as hepatitis B (HepB), the timing of doses becomes crucial to ensure optimal immunity. The HepA and HepB combination vaccine, for instance, is administered in a series of doses to provide long-term protection against both viruses. Typically, this combination vaccine is given as a 3-dose series, with the first dose administered at any time, followed by the second dose 1 to 2 months later, and the third dose given 6 months after the first dose. This schedule ensures that the immune system has sufficient time to build a robust response to both hepatitis A and B antigens.
For individuals who require protection against both hepatitis A and B, the combination vaccine is a practical choice, especially for travelers or those at increased risk of exposure. The dual protection offered by this vaccine reduces the number of clinic visits and injections needed, improving compliance and overall vaccination rates. It’s important to note that the timing between doses must be adhered to for maximum effectiveness. Deviating from the recommended schedule may compromise the immune response, necessitating additional doses or delaying full protection.
In some cases, HepA may also be combined with other vaccines, such as those for typhoid or inactivated polio vaccine (IPV), depending on the manufacturer and regional availability. When HepA is part of a multi-component vaccine, the dosing intervals are typically aligned with the component requiring the most frequent administration. For example, if HepA is combined with a vaccine that follows a 2-dose schedule, the timing of the HepA doses may be adjusted to match, ensuring all components are administered correctly. Healthcare providers should consult the specific product information for the combination vaccine being used to confirm the appropriate dosing intervals.
Travelers, in particular, benefit from combination vaccines as they often need protection against multiple diseases before their trips. For instance, a traveler to a region with high rates of hepatitis A and B may receive the HepA-HepB combination vaccine, with the first dose administered as soon as possible, followed by the second dose 1 month later, and the third dose 6 months after the first. This accelerated schedule can provide earlier protection, though it may require careful planning to ensure all doses are received within the recommended timeframe. It’s essential to discuss travel plans with a healthcare provider to determine the most appropriate vaccination schedule.
Lastly, for children and adolescents, combination vaccines including HepA and HepB are often integrated into routine immunization schedules. The Centers for Disease Control and Prevention (CDC) recommends the HepA vaccine for all children starting at age 12 months, and when combined with HepB, the series can be coordinated with other childhood vaccinations. This approach minimizes the number of injections a child receives while ensuring timely protection against multiple diseases. Parents and caregivers should follow the guidance of their healthcare provider to ensure their child receives all doses of the combination vaccine at the correct intervals.
In summary, when hepatitis A is paired with other vaccines like hepatitis B in combination formulations, the timing of doses is carefully structured to maximize immunity and convenience. Adhering to the recommended schedule is essential for achieving full protection, whether for routine immunization, travel, or specific risk groups. Healthcare providers play a critical role in educating patients about the importance of completing the vaccine series and ensuring doses are administered at the appropriate intervals.
Bacterin vs. Vaccine: Understanding the Key Differences and Uses
You may want to see also
Frequently asked questions
Typically, the hepatitis A vaccine requires two doses. The second dose should be given 6 to 18 months after the first dose for long-term protection.
It is not recommended to administer the doses closer than 6 months apart, as this interval ensures optimal immune response and long-lasting immunity.
No, if the interval between doses is longer than 18 months, you do not need to restart the series. The previously administered dose(s) still count, and you can receive the remaining dose(s) as soon as possible.