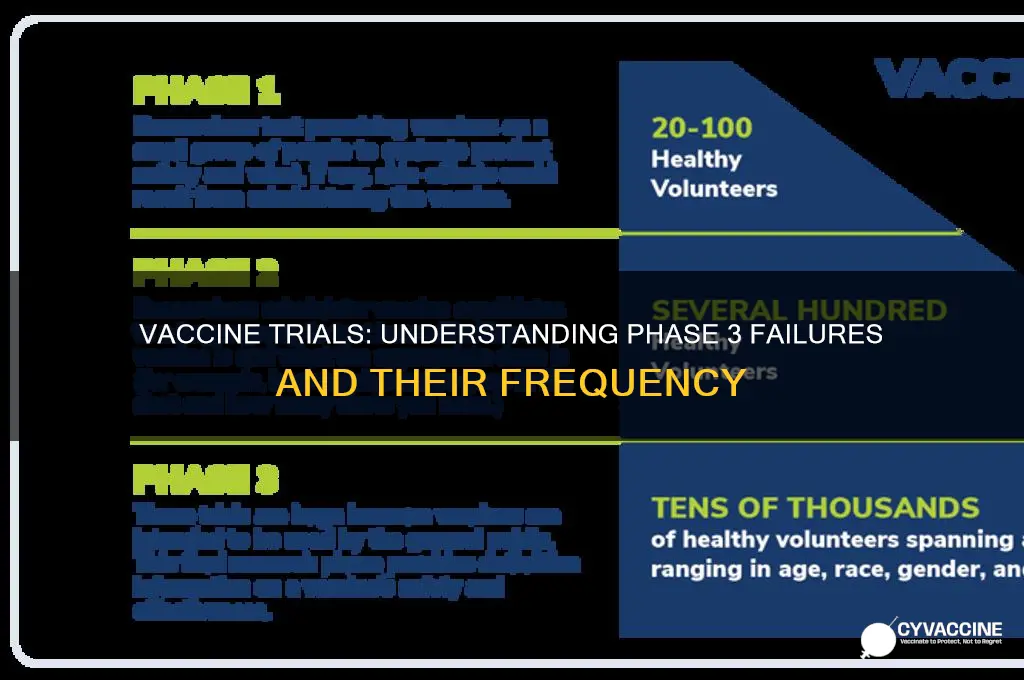
Vaccine development is a rigorous process involving multiple phases of clinical trials to ensure safety and efficacy before widespread use. Phase 3 trials, the final stage before approval, are large-scale studies designed to confirm a vaccine’s effectiveness in real-world populations. While these trials are highly scrutinized, vaccines can still fail at this stage due to insufficient efficacy, safety concerns, or inability to meet predefined endpoints. Historically, a significant percentage of vaccine candidates do not progress beyond Phase 3, highlighting the challenges in translating promising early results into a reliable, broadly effective product. Understanding the frequency and reasons for such failures is crucial for improving vaccine development and public health strategies.
Explore related products






What You'll Learn
- Failure Rates by Vaccine Type: Comparing failure rates across different vaccines in phase 3 trials
- Common Reasons for Failure: Identifying primary causes of phase 3 vaccine trial failures
- Efficacy Thresholds: Analyzing how efficacy thresholds impact phase 3 success rates
- Safety Concerns: Role of adverse events in halting phase 3 vaccine trials
- Regulatory Hurdles: How regulatory requirements contribute to phase 3 vaccine failures
![]()
Failure Rates by Vaccine Type: Comparing failure rates across different vaccines in phase 3 trials
Vaccine development is a rigorous process, and Phase 3 trials are a critical stage where efficacy and safety are evaluated in large, diverse populations. Failure rates in this phase can vary significantly depending on the type of vaccine being developed. For instance, viral vector-based vaccines, such as those for Ebola or COVID-19, have shown varying success rates. The Ebola vaccine Ervebo demonstrated high efficacy (around 97.5%) in Phase 3 trials, while some COVID-19 viral vector vaccines, like AstraZeneca’s, faced challenges with lower efficacy rates (around 60-70%) compared to mRNA alternatives. These differences highlight the complexity of viral vector technology and its dependence on factors like pre-existing immunity to the vector.
In contrast, mRNA vaccines, such as Pfizer-BioNTech and Moderna’s COVID-19 vaccines, have shown remarkably high efficacy rates in Phase 3 trials, typically exceeding 90%. This success is attributed to the innovative platform technology, which allows for rapid development and precise targeting of viral proteins. However, mRNA vaccines for other diseases, such as HIV or influenza, have not yet achieved similar success in Phase 3, underscoring the challenges of applying this technology broadly. Failure rates in these cases often stem from the complexity of the target pathogen and the difficulty in eliciting a robust immune response.
Protein subunit vaccines, like Novavax’s COVID-19 vaccine, have also demonstrated moderate to high efficacy (around 85-90%) in Phase 3 trials. These vaccines use a specific piece of the pathogen, often combined with adjuvants, to stimulate an immune response. While generally safer and more stable than other platforms, their efficacy can be limited by the choice of antigen and adjuvant. Failure in this category often occurs when the selected antigen fails to induce sufficient immunity or when the adjuvant does not enhance the response as expected.
Live attenuated and inactivated vaccines, commonly used for diseases like measles, polio, and influenza, have historically shown high success rates in Phase 3 trials. However, their failure rates can increase when applied to more complex pathogens or when attenuation is not optimally achieved. For example, some inactivated vaccines for respiratory syncytial virus (RSV) have failed in Phase 3 due to issues like immune enhancement, where the vaccine paradoxically worsens the disease upon exposure to the pathogen.
Finally, DNA vaccines, though promising in preclinical studies, have struggled in Phase 3 trials. Despite their theoretical advantages, such as stability and ease of production, they have often failed to demonstrate sufficient efficacy in humans. For instance, DNA vaccines for HIV and malaria have shown disappointing results, with efficacy rates well below 50%. This highlights the gap between preclinical promise and clinical performance, often attributed to inadequate immune stimulation in humans.
In summary, failure rates in Phase 3 trials vary widely across vaccine types, influenced by factors like platform technology, pathogen complexity, and immunological challenges. Understanding these differences is crucial for improving vaccine development strategies and setting realistic expectations for future candidates.
Understanding Childhood Vaccination Schedules: How Often Are Shots Needed?
You may want to see also
Explore related products





![]()
Common Reasons for Failure: Identifying primary causes of phase 3 vaccine trial failures
Phase 3 clinical trials are a critical stage in vaccine development, designed to assess safety, efficacy, and immunogenicity in a large, diverse population. Despite rigorous earlier phases, many vaccine candidates fail at this stage due to various factors. One of the primary reasons for failure is insufficient efficacy, where the vaccine does not provide the expected level of protection against the target disease. This can occur if the immune response generated is inadequate or if the pathogen mutates, rendering the vaccine less effective. For example, vaccines targeting rapidly evolving viruses like influenza or HIV often struggle to achieve consistent efficacy across diverse populations.
Another common cause of Phase 3 failure is safety concerns. While rare adverse events may not be detected in smaller Phase 1 or 2 trials, they can become apparent when the vaccine is administered to thousands of participants. Serious side effects, such as severe allergic reactions or unexpected long-term health issues, can halt a trial or lead to regulatory rejection. The 2020 COVID-19 vaccine trials, for instance, closely monitored participants for rare but significant events like thrombosis with thrombocytopenia syndrome (TTS) associated with adenovirus-vector vaccines.
Poor study design or execution is also a significant contributor to Phase 3 failures. Issues such as inadequate sample size, improper randomization, or insufficient follow-up periods can compromise the trial's ability to detect meaningful outcomes. Additionally, challenges in participant recruitment or retention, particularly in diverse or hard-to-reach populations, can skew results and undermine the trial's validity. For example, a vaccine trial that fails to enroll enough participants from high-risk groups may not accurately reflect real-world efficacy.
Manufacturing and logistical issues can further derail Phase 3 trials. Ensuring consistent vaccine quality across large-scale production is essential, as variations in formulation or storage conditions (e.g., temperature excursions) can affect potency and safety. Supply chain disruptions, particularly in global trials, can also delay or halt studies, as seen during the COVID-19 pandemic. These logistical challenges often highlight the complexity of scaling up vaccine production while maintaining stringent quality control.
Lastly, emerging scientific or regulatory hurdles can lead to Phase 3 failures. As trials progress, new data on the pathogen, competing vaccines, or evolving regulatory standards may render a candidate less viable. For instance, if a more effective vaccine enters the market during a Phase 3 trial, the ethical and practical justification for continuing the study may diminish. Similarly, regulatory agencies may introduce stricter requirements for approval, necessitating additional trials or modifications to the vaccine.
Understanding these common reasons for failure is crucial for improving the success rate of Phase 3 vaccine trials. By addressing efficacy, safety, study design, manufacturing, and regulatory challenges proactively, researchers can enhance the likelihood of developing safe and effective vaccines that meet public health needs.
Vaccine Effectiveness: Kennel Cough
You may want to see also
Explore related products






![]()
Efficacy Thresholds: Analyzing how efficacy thresholds impact phase 3 success rates
Efficacy thresholds play a pivotal role in determining the success or failure of vaccines during phase 3 clinical trials. These thresholds, typically set by regulatory agencies like the FDA or EMA, define the minimum level of effectiveness a vaccine must demonstrate to be considered viable for approval. For instance, COVID-19 vaccines were generally required to show an efficacy rate of at least 50% to meet regulatory standards. When a vaccine’s efficacy falls below this threshold, it risks failing phase 3, even if it shows some protective benefits. This stringent criterion ensures that only vaccines with proven, substantial public health impact progress to market, but it also means that many candidates, despite showing promise in earlier phases, may not meet the required bar.
The impact of efficacy thresholds on phase 3 success rates is further complicated by the variability in disease prevalence and trial design. In diseases with high prevalence, a vaccine may need to demonstrate higher efficacy to achieve statistically significant results, increasing the likelihood of failure. Conversely, in low-prevalence settings, even a moderately effective vaccine might struggle to prove its worth due to insufficient endpoint events in the trial. For example, a vaccine with 60% efficacy might fail in a trial with too few cases to confidently measure its impact. Thus, the interplay between efficacy thresholds and trial design can significantly influence whether a vaccine succeeds or fails in phase 3.
Another critical factor is the comparison of the vaccine candidate against existing treatments or vaccines. If a disease already has highly effective vaccines or treatments available, regulatory agencies may set higher efficacy thresholds for new candidates to ensure they offer meaningful improvements. This raises the bar for success and increases the likelihood of failure for vaccines that, while effective, do not outperform existing options. For instance, a new flu vaccine with 70% efficacy might fail phase 3 if it does not demonstrate superiority over a currently available vaccine with 75% efficacy.
The choice of endpoints in phase 3 trials also interacts with efficacy thresholds to determine success rates. Trials often measure multiple endpoints, such as prevention of infection, severe disease, or hospitalization. If a vaccine fails to meet the efficacy threshold for the primary endpoint but succeeds in secondary endpoints, it may still be deemed a failure overall. This highlights the importance of aligning trial endpoints with regulatory expectations and public health needs. Vaccines that show strong efficacy in preventing severe outcomes but fall short in preventing mild infections may still offer significant value, yet they risk failing phase 3 if the primary endpoint is not met.
Finally, the global health context and evolving disease dynamics can influence how efficacy thresholds are applied and how often vaccines fail in phase 3. For example, during the COVID-19 pandemic, vaccines were evaluated against rapidly mutating variants, which could reduce their efficacy over time. If a vaccine’s efficacy drops below the threshold due to variant-specific challenges, it may fail phase 3 despite initial success. This underscores the need for flexible yet rigorous thresholds that account for real-world complexities while maintaining high standards for public safety and efficacy. In summary, efficacy thresholds are a critical determinant of phase 3 success rates, and their application must balance scientific rigor with practical considerations to ensure the development of effective vaccines.
Mississippi's Law on Vaccines for Children
You may want to see also
Explore related products






![]()
Safety Concerns: Role of adverse events in halting phase 3 vaccine trials
Phase 3 clinical trials are a critical stage in vaccine development, designed to assess both the efficacy and safety of a vaccine in a large, diverse population. While efficacy is a primary focus, safety concerns, particularly adverse events, play a pivotal role in determining whether a trial continues or is halted. Adverse events (AEs) are any undesirable experiences occurring after vaccination, ranging from mild reactions like soreness at the injection site to severe, life-threatening conditions. The occurrence of serious adverse events (SAEs) can raise significant red flags, prompting regulatory bodies and data safety monitoring boards (DSMBs) to reevaluate the trial's risks versus benefits.
The decision to halt a Phase 3 vaccine trial due to adverse events is not taken lightly. It typically occurs when there is a clear signal of harm that outweighs the potential benefits of the vaccine. For instance, if a cluster of severe AEs is observed in the vaccinated group compared to the placebo group, it may indicate a causal relationship with the vaccine. Historical examples, such as the 2020 pause of the Oxford-AstraZeneca COVID-19 vaccine trial due to a case of transverse myelitis, highlight how even rare but serious events can lead to temporary halts. These pauses allow investigators to thoroughly investigate the cause, severity, and frequency of the adverse event before deciding whether to proceed.
Transparency and rigorous monitoring are essential in managing safety concerns during Phase 3 trials. DSMBs independently review accumulating data to ensure participant safety and trial integrity. If an adverse event is deemed related to the vaccine and poses an unacceptable risk, the trial may be suspended or terminated. This process is crucial for maintaining public trust and ensuring that only safe vaccines advance to regulatory approval. However, it is important to note that not all adverse events lead to trial halts; many are minor and do not impact the trial's progression.
The frequency of Phase 3 vaccine trials being halted due to adverse events is relatively low, as safety is meticulously evaluated in earlier phases. However, when such halts occur, they underscore the importance of prioritizing participant safety over expediting vaccine development. For example, the 2007 halt of a dengue vaccine trial due to an increased risk of severe disease in certain recipients demonstrated how adverse events can reveal critical insights into a vaccine's mechanism and population-specific risks. These instances also emphasize the need for diverse trial populations to detect rare but significant safety issues.
In conclusion, adverse events are a central consideration in Phase 3 vaccine trials, with the potential to halt or modify studies if they pose serious safety risks. While such occurrences are infrequent, they serve as a reminder of the rigorous standards applied to vaccine development. By carefully monitoring and addressing safety concerns, researchers and regulators ensure that approved vaccines meet high safety thresholds, protecting public health while maintaining confidence in immunization programs. Understanding the role of adverse events in trial halts is essential for appreciating the complexities and safeguards inherent in vaccine development.
Jenny McCarthy's Vaccine Views: A Change of Heart?
You may want to see also
Explore related products

$47.99 $59.99





![]()
Regulatory Hurdles: How regulatory requirements contribute to phase 3 vaccine failures
Vaccine development is a rigorous process, and Phase 3 clinical trials are a critical juncture where many candidates face significant challenges, including regulatory hurdles. These hurdles are not merely bureaucratic obstacles but essential safeguards designed to ensure the safety, efficacy, and quality of vaccines before they reach the public. However, the stringent regulatory requirements can sometimes contribute to Phase 3 failures, particularly when developers struggle to meet the high standards set by agencies like the FDA, EMA, or WHO. One major regulatory requirement is the demonstration of statistical significance in clinical endpoints, such as disease prevention or reduction in severity. If a vaccine fails to meet these predefined thresholds, even by a narrow margin, it may be deemed ineffective, leading to trial failure. This is compounded by the need for large, diverse study populations, which can be difficult to recruit and retain, especially in regions with low disease incidence or logistical challenges.
Another regulatory factor contributing to Phase 3 failures is the demand for long-term safety data. Regulatory agencies often require extended follow-up periods to identify rare adverse events that may not appear during shorter trials. This prolongs the trial timeline and increases costs, creating financial and operational pressures for developers. Additionally, the evolving nature of regulatory guidelines can pose challenges. For instance, changes in safety monitoring requirements or the introduction of new biomarkers for efficacy assessment may necessitate mid-trial adjustments, potentially compromising data integrity or requiring additional resources. These shifting standards can be particularly burdensome for smaller biotech companies with limited flexibility.
Manufacturing and quality control standards also play a pivotal role in regulatory compliance and can lead to Phase 3 failures if not adequately addressed. Vaccines must be produced under Good Manufacturing Practices (GMP) to ensure consistency and purity across batches. Any deviations, such as contamination or variability in formulation, can result in regulatory rejection, even if the vaccine shows promise in clinical trials. Furthermore, the complexity of certain vaccine platforms, such as mRNA or viral vector-based vaccines, adds layers of regulatory scrutiny, as these technologies often require novel analytical methods and stability assessments.
Regulatory agencies also enforce strict criteria for trial design, including the choice of control groups and endpoints. For example, using a placebo control in regions where an effective vaccine is already available may raise ethical concerns, necessitating the use of active comparators, which can complicate efficacy assessments. Similarly, the selection of primary endpoints must align with regulatory expectations, and misalignment can lead to trial failure even if the vaccine demonstrates benefits in secondary outcomes. These design constraints require meticulous planning and often involve extensive consultations with regulators, adding complexity and delay to the development process.
Finally, global regulatory harmonization remains an ongoing challenge. Vaccines intended for international markets must meet the requirements of multiple regulatory bodies, each with its own standards and procedures. This lack of harmonization can lead to discrepancies in trial design, data interpretation, and approval timelines, increasing the risk of Phase 3 failure. For instance, a vaccine that meets the criteria of one agency may fall short in another due to differences in acceptable safety profiles or efficacy thresholds. Navigating these diverse regulatory landscapes requires significant expertise and resources, further exacerbating the hurdles faced by vaccine developers.
In summary, while regulatory requirements are essential for public health protection, they can contribute to Phase 3 vaccine failures through stringent efficacy and safety standards, manufacturing complexities, trial design constraints, and global harmonization challenges. Addressing these hurdles requires a collaborative effort between developers, regulators, and stakeholders to streamline processes without compromising safety or efficacy. By understanding and mitigating these regulatory challenges, the vaccine development pipeline can become more resilient, ultimately increasing the likelihood of success in Phase 3 trials.
Vaccines: Safeguarding Public Health and Strengthening Our Society's Well-being
You may want to see also
Frequently asked questions
The failure rate of vaccines in phase 3 trials varies, but historically, approximately 30-40% of vaccine candidates fail at this stage due to insufficient efficacy, safety concerns, or other issues.
Vaccines often fail in phase 3 due to inadequate immune response (low efficacy), unexpected side effects, or difficulty demonstrating superiority over existing vaccines or placebos in large, diverse populations.
Yes, a vaccine that fails in phase 3 can be reconsidered or redeveloped if the issues are addressable, such as adjusting the dosage, formulation, or target population. However, it requires additional research, funding, and regulatory approval to proceed.