Childhood vaccination schedules are carefully designed to protect children from a range of serious and potentially life-threatening diseases. These schedules typically include a series of vaccines administered at specific ages, starting from infancy through adolescence. The number of vaccines in a childhood schedule can vary depending on the country and its public health guidelines, but in the United States, for example, the Centers for Disease Control and Prevention (CDC) recommends around 14 different vaccines to protect against diseases such as measles, mumps, rubella, polio, whooping cough, and influenza. While the number of vaccines may seem high, they are rigorously tested and proven safe, and their benefits in preventing illness and saving lives far outweigh the minimal risks associated with vaccination. Understanding the childhood vaccination schedule is crucial for parents and caregivers to ensure their children receive timely protection against preventable diseases.
Explore related products


$11.93 $21.99




What You'll Learn
- Vaccine Types: Overview of different vaccines included in the childhood immunization schedule
- Age-Specific Doses: Recommended vaccine doses and timing for various childhood age groups
- Mandatory vs. Optional: Distinction between required and optional vaccines in childhood schedules
- Combination Vaccines: Use of combination vaccines to reduce the number of shots needed
- Global Variations: Differences in childhood vaccine schedules across countries and regions
![]()
Vaccine Types: Overview of different vaccines included in the childhood immunization schedule
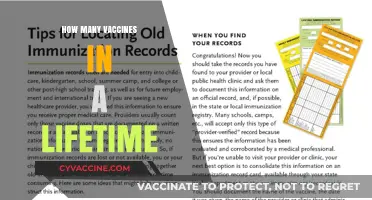
Childhood immunization schedules are meticulously designed to protect against a range of preventable diseases, with vaccines administered at specific ages to maximize efficacy and safety. These schedules typically include 14–16 vaccine types, though the exact number varies by country and healthcare guidelines. Each vaccine targets distinct pathogens, employing unique mechanisms to build immunity. Understanding these types is crucial for parents and caregivers navigating the complexities of pediatric healthcare.
Inactivated and Live-Attenuated Vaccines: The Foundation of Early Immunity
Many childhood vaccines fall into two primary categories: inactivated and live-attenuated. Inactivated vaccines, like the injectable polio vaccine (IPV), contain killed pathogens incapable of causing disease but sufficient to trigger an immune response. These are often administered in multiple doses, such as the 4-dose IPV series starting at 2 months. Live-attenuated vaccines, such as the measles, mumps, and rubella (MMR) vaccine, use weakened pathogens to stimulate robust immunity. The MMR vaccine is typically given as a first dose at 12–15 months and a second dose at 4–6 years, offering lifelong protection against three serious diseases with a single shot.
Combination Vaccines: Streamlining Immunization
To simplify the schedule and reduce the number of injections, combination vaccines are widely used. For instance, the DTaP vaccine protects against diphtheria, tetanus, and pertussis in a single shot, administered at 2, 4, and 6 months, followed by boosters at 15–18 months and 4–6 years. Similarly, the Pentavalent vaccine, available in some regions, combines protection against diphtheria, tetanus, pertussis, hepatitis B, and *Haemophilus influenzae* type b (Hib), reducing clinic visits and improving compliance.
Conjugate and Subunit Vaccines: Targeted Precision
Conjugate vaccines, like the Hib and pneumococcal conjugate vaccines (PCV13), link a weak antigen to a strong one to enhance the immune response in young children. PCV13, given at 2, 4, 6, and 12–15 months, protects against 13 strains of pneumococcal bacteria, a leading cause of pneumonia and meningitis. Subunit vaccines, such as the hepatitis B vaccine, use specific pieces of the pathogen (e.g., proteins or sugars) to elicit immunity. The hepatitis B vaccine is often administered at birth, followed by doses at 1–2 months and 6–18 months, providing early protection against a lifelong infection.
Practical Tips for Parents: Navigating the Schedule
Adhering to the immunization schedule is critical, but flexibility exists for missed doses. For example, if a child misses the 6-month dose of DTaP, it can be administered as soon as possible without restarting the series. Parents should also be aware of potential side effects, such as mild fever or soreness at the injection site, which are normal and manageable with acetaminophen or cool compresses. Keeping a vaccination record and discussing any concerns with a healthcare provider ensures children receive timely protection against preventable diseases.
This overview highlights the diversity and specificity of vaccines in the childhood schedule, each designed to safeguard health through scientifically proven methods. By understanding these types, caregivers can make informed decisions and contribute to global efforts to eradicate vaccine-preventable diseases.
Understanding the CPT Code for Malaria Vaccine Administration
You may want to see also
Explore related products



$55



![]()
Age-Specific Doses: Recommended vaccine doses and timing for various childhood age groups
Childhood vaccination schedules are meticulously designed to provide protection when children are most vulnerable to specific diseases. The timing and dosage of vaccines are tailored to each age group, ensuring optimal immune response while minimizing risks. For instance, the Hepatitis B vaccine is typically administered at birth, with subsequent doses at 1–2 months and 6–18 months, offering early protection against a potentially life-threatening virus. This precision in scheduling underscores the importance of adhering to age-specific guidelines.
Infants (0–12 months) receive the bulk of their vaccinations, as their immune systems are still developing. The Centers for Disease Control and Prevention (CDC) recommends vaccines like DTaP (Diphtheria, Tetanus, Pertussis), Hib (Haemophilus influenzae type b), and PCV13 (Pneumococcal conjugate vaccine) in a series of doses starting at 2 months. Each dose builds upon the previous one, creating a robust immune memory. Parents should note that some vaccines, like Rotavirus, are given orally and require a specific number of doses (usually 2 or 3) depending on the brand. Missing a dose can delay protection, so maintaining a consistent schedule is crucial.
Toddlers and preschoolers (1–4 years) receive booster shots to reinforce immunity. For example, the MMR (Measles, Mumps, Rubella) vaccine is typically given as a first dose at 12–15 months and a second dose at 4–6 years. This two-dose regimen ensures long-term protection against highly contagious diseases. Additionally, the flu vaccine is recommended annually starting at 6 months of age, with children under 9 requiring two doses in their first year of vaccination to build full immunity. This age group also receives the final doses of vaccines like Hepatitis A and Chickenpox, completing their early childhood immunization series.
School-age children (5–10 years) focus on maintaining immunity and addressing new risks. The DTaP series concludes with a booster dose (DTaP or Tdap) around 4–6 years, while the IPV (Inactivated Polio Vaccine) series is completed by age 6. Preteens (11–12 years) receive additional vaccines like HPV (Human Papillomavirus), Meningococcal, and a Tdap booster. These vaccines are timed to provide protection before potential exposure increases, such as during adolescence. For example, the HPV vaccine is most effective when given before potential exposure to the virus, typically in two doses for those vaccinated before age 15.
Practical tips for parents include keeping a detailed vaccination record, scheduling appointments well in advance, and discussing any concerns with healthcare providers. Some vaccines, like the flu shot, require annual administration, while others, like MMR, are given years apart. Understanding the rationale behind age-specific doses empowers parents to make informed decisions and ensures children receive the full benefits of immunization. Adhering to these schedules not only protects individual children but also contributes to community immunity, safeguarding those who cannot be vaccinated due to medical reasons.
Debunking the Myth: The MMR Vaccine and Autism Connection
You may want to see also
Explore related products






![]()
Mandatory vs. Optional: Distinction between required and optional vaccines in childhood schedules
Childhood vaccination schedules are meticulously designed to protect against serious diseases, but not all vaccines are treated equally. A clear distinction exists between mandatory and optional vaccines, shaped by factors like disease prevalence, public health risk, and regional policies. Mandatory vaccines, such as MMR (measles, mumps, rubella) and DTaP (diphtheria, tetanus, pertussis), are required for school entry in most countries due to their proven efficacy in preventing highly contagious and potentially fatal illnesses. Optional vaccines, like the rotavirus or hepatitis A vaccines, are recommended but not enforced, often targeting diseases with lower transmission rates or milder outcomes in specific populations.
Consider the MMR vaccine, typically administered in two doses at 12–15 months and 4–6 years. Its mandatory status stems from measles’ highly contagious nature, with a single case capable of infecting 90% of unvaccinated contacts. In contrast, the HPV vaccine, recommended for adolescents around ages 11–12, is often optional despite its ability to prevent cancers caused by human papillomavirus. This distinction reflects societal priorities and the perceived balance between individual choice and public health benefits.
The decision to classify a vaccine as mandatory or optional also hinges on regional disease burden and healthcare infrastructure. For instance, the meningococcal vaccine is mandatory in certain U.S. states due to localized outbreaks, while it remains optional in countries with lower incidence rates. Similarly, the influenza vaccine, though universally recommended annually starting at 6 months, is rarely mandatory outside specific settings like healthcare employment. Parents must weigh these recommendations against their child’s health needs, travel plans, and community risk factors.
Practical considerations further complicate this distinction. Mandatory vaccines often align with school entry requirements, simplifying compliance but limiting flexibility. Optional vaccines, however, require proactive decision-making. For example, the chickenpox vaccine (Varicella), mandatory in some regions, is optional in others, leaving parents to assess risks like potential complications (e.g., pneumonia) versus the likelihood of natural exposure. Tools like immunization trackers and pediatrician consultations can help navigate these choices effectively.
Ultimately, the mandatory-optional divide underscores the dynamic nature of vaccination policies. While mandatory vaccines form the backbone of herd immunity, optional vaccines address nuanced risks, empowering parents to tailor protection to their child’s unique circumstances. Understanding this distinction ensures informed decisions, balancing public health imperatives with individual needs.
How European Vaccine Manufacturing Differs: A Comparative Analysis
You may want to see also
Explore related products






![]()
Combination Vaccines: Use of combination vaccines to reduce the number of shots needed
Childhood vaccination schedules often include multiple doses of various vaccines, which can be overwhelming for both parents and children. To streamline this process, combination vaccines have been developed, merging multiple antigens into a single shot. For instance, the DTaP vaccine protects against diphtheria, tetanus, and pertussis, reducing the need for three separate injections. This approach not only minimizes the number of shots but also simplifies the immunization process, ensuring children receive essential protection with fewer clinic visits.
Consider the practical benefits of combination vaccines for parents and healthcare providers. A typical childhood schedule might include vaccines for measles, mumps, rubella (MMR), and varicella (chickenpox), which can now be administered together as the MMRV vaccine. This combination reduces the number of injections from four to two, easing the physical and emotional stress on children. Additionally, it optimizes clinic efficiency by reducing appointment times and administrative burdens. For example, the Pentacel vaccine combines DTaP, IPV (polio), and Hib (Haemophilus influenzae type b) into one shot, suitable for infants aged 6 weeks to 4 years, requiring only four doses instead of separate administrations.
However, the use of combination vaccines requires careful consideration of potential drawbacks. While they reduce the number of shots, some combinations may increase the risk of mild side effects, such as fever or soreness at the injection site. For instance, the MMRV vaccine has been associated with a slightly higher risk of fever-related seizures in children aged 12–23 months compared to separate MMR and varicella shots. Parents should weigh these risks against the convenience and ensure open communication with healthcare providers to make informed decisions.
Implementing combination vaccines also demands precision in dosage and timing. For example, the DTaP-IPV-Hib vaccine (e.g., Pentacel) is administered in a 3-dose series at 2, 4, and 6 months of age, followed by boosters. Adhering to this schedule ensures optimal immunity without overloading the child’s immune system. Healthcare providers must stay updated on evolving guidelines, as new combinations like the hexavalent vaccine (DTaP-IPV-Hib-HepB) are introduced, offering protection against six diseases in one shot but requiring strict adherence to age-specific protocols.
In conclusion, combination vaccines are a strategic innovation in childhood immunization, reducing the number of shots while maintaining robust protection against multiple diseases. By consolidating antigens, they offer practical advantages for families and healthcare systems, though careful consideration of potential side effects and precise scheduling is essential. As vaccine technology advances, these combinations will continue to play a pivotal role in simplifying and optimizing childhood vaccination schedules.
Polio Vaccine: Muscles, Nerves, and Side Effects
You may want to see also
Explore related products





![]()
Global Variations: Differences in childhood vaccine schedules across countries and regions
Childhood vaccine schedules vary significantly across the globe, reflecting differences in disease prevalence, healthcare infrastructure, and public health priorities. For instance, the United States Centers for Disease Control and Prevention (CDC) recommends up to 14 different vaccines by age 6, including measles, mumps, rubella (MMR), and human papillomavirus (HPV). In contrast, the World Health Organization (WHO) provides a more streamlined Essential Programme on Immunization (EPI), focusing on six core vaccines: BCG (tuberculosis), DTP (diphtheria, tetanus, pertussis), polio, measles, and hepatitis B. These disparities highlight how regional health challenges shape immunization strategies.
Consider the case of Japan, where the childhood schedule includes vaccines like BCG at birth and a 4-dose DTaP series starting at 3 months. However, Japan does not routinely administer the varicella (chickenpox) vaccine until age 5, unlike the U.S., where it is given in two doses starting at 12 months. Such variations often stem from historical disease patterns; Japan’s lower incidence of chickenpox in early childhood influences its delayed vaccination approach. Parents navigating international moves should consult healthcare providers to ensure continuity in their child’s immunization, especially when transitioning between countries with differing schedules.
In low-resource regions, vaccine schedules are often tailored to combat the most immediate threats. For example, in sub-Saharan Africa, yellow fever vaccination is prioritized due to the disease’s endemic status, typically administered at 9 months. Similarly, countries with high tuberculosis rates, such as India, mandate BCG vaccination at birth, often leaving a distinctive scar as a marker of immunization. These adaptations underscore the importance of aligning vaccine schedules with local epidemiological data, ensuring resources are directed where they are most needed.
A comparative analysis reveals that wealthier nations often incorporate newer vaccines, such as rotavirus and pneumococcal conjugate vaccines, into their schedules. For instance, Australia includes a 3-dose rotavirus series starting at 2 months, while many African countries are still working to introduce it due to cost and logistical challenges. This disparity highlights the role of economic factors in shaping vaccine accessibility. Global initiatives like Gavi, the Vaccine Alliance, aim to bridge this gap by subsidizing vaccines for low-income countries, but disparities persist, emphasizing the need for sustained international collaboration.
Practical tips for parents and healthcare providers include staying informed about regional vaccine requirements, especially when traveling or relocating. For example, some countries require proof of certain vaccinations, like yellow fever, for entry. Additionally, maintaining a detailed immunization record is crucial, as schedules may differ in dosing intervals or vaccine combinations. For instance, the U.K. uses a 3-in-1 DTaP/IPV/Hib vaccine, while the U.S. administers these separately or in different combinations. Understanding these nuances ensures children receive timely and appropriate protection, regardless of their location.
Effective and Gentle Vaccine Administration Tips for Children Aged 8-10
You may want to see also
Frequently asked questions
The childhood immunization schedule typically includes around 14 different vaccines, which protect against 16 vaccine-preventable diseases.
No, some vaccines are combined into a single shot to reduce the number of injections. For example, the MMR vaccine protects against measles, mumps, and rubella.
The number of doses varies by vaccine. Some require a single dose, while others need multiple doses (e.g., 2-4 doses) for full protection, often given at specific intervals.
Yes, the schedule is regularly updated by health organizations like the CDC and WHO based on new scientific evidence, disease trends, and vaccine availability.
Requirements vary by country and state, but many vaccines in the childhood schedule are mandatory for school entry, though exemptions may be allowed for medical, religious, or philosophical reasons.