The global response to the COVID-19 pandemic has highlighted significant disparities in vaccine distribution and access among countries. As nations raced to secure doses for their populations, the number of vaccines ordered by each country became a critical indicator of their preparedness and strategy. Wealthier nations often pre-purchased large quantities of multiple vaccine candidates, ensuring a robust supply, while many low- and middle-income countries faced challenges in securing sufficient doses due to limited resources and global supply chain constraints. Analyzing how many vaccines each country ordered provides insight into the geopolitical dynamics of vaccine equity, the role of international initiatives like COVAX, and the broader implications for global health cooperation.
Explore related products





What You'll Learn
![]()
Global vaccine distribution disparities
The COVID-19 pandemic exposed a stark reality: vaccine distribution is not equitable. While some countries secured enough doses to vaccinate their populations multiple times over, others struggled to access even a fraction of what they needed. Data from Duke University's Global Health Innovation Center reveals a glaring disparity: as of 2022, high-income countries had purchased over 7 billion vaccine doses, compared to just 1.2 billion for low-income countries. This imbalance isn't merely a numbers game; it translates to lives lost, economies crippled, and a prolonged global health crisis.
High-income nations, leveraging their financial muscle and existing relationships with pharmaceutical companies, secured advance purchase agreements early in the pandemic. The United States, for instance, pre-ordered enough doses to vaccinate its population nearly five times over, while Canada secured enough for nearly three times its population. This "vaccine hoarding" left low-income countries reliant on initiatives like COVAX, which, despite its noble intentions, faced significant funding shortfalls and logistical challenges.
Consider the case of India, a middle-income country with a massive population. Despite having domestic vaccine production capabilities, it faced a devastating second wave in 2021 due to initial vaccine shortages. In contrast, Israel, a high-income country with a smaller population, secured early access to vaccines and became one of the first nations to achieve widespread vaccination coverage. This disparity highlights the critical role of purchasing power and global solidarity in ensuring equitable access.
A closer look at dosage requirements further complicates the picture. Many vaccines require two doses, and some, like the Pfizer-BioNTech vaccine, necessitate ultra-cold storage, posing additional challenges for countries with limited infrastructure. This means that even if a country secures a certain number of doses, logistical hurdles can hinder effective distribution, particularly in rural or underserved areas.
Addressing these disparities requires a multi-pronged approach. Wealthy nations must fulfill their dose-sharing pledges and support initiatives like COVAX with both financial contributions and technology transfers to boost local production capacities in low-income countries. Waiving intellectual property rights for COVID-19 vaccines, as proposed by some countries, could also accelerate global production. Ultimately, achieving vaccine equity isn't just a moral imperative; it's a public health necessity. Until every country has access to sufficient vaccines, the pandemic will continue to pose a threat to global health and economic stability.
Do Vaccines Expire in Your Body? Understanding Immunity Duration
You may want to see also
Explore related products






![]()
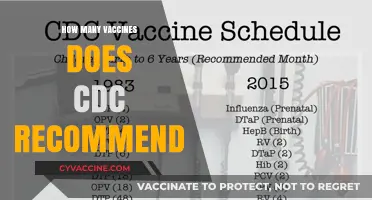
Top countries by vaccine orders
The global race to secure COVID-19 vaccines revealed stark disparities in purchasing power and strategic planning among nations. Leading the pack, the United States pre-ordered over 1.2 billion doses, enough to vaccinate its population multiple times and donate surplus doses internationally. This aggressive procurement strategy, part of Operation Warp Speed, aimed to ensure domestic supply while positioning the U.S. as a key player in global vaccine distribution. Canada, despite its smaller population, secured over 400 million doses—nearly 10 times its population—to hedge against potential supply chain disruptions and variant-specific booster needs. These examples highlight how wealthier nations prioritized over-procurement to safeguard their populations and maintain geopolitical influence.
Contrastingly, low-income countries faced significant challenges in securing adequate vaccine supplies. For instance, many African nations relied heavily on COVAX, a global initiative aimed at equitable vaccine distribution, yet still struggled to meet even minimal vaccination targets. India, a major vaccine producer, initially focused on domestic manufacturing and export bans to address its massive population, later shifting to large-scale orders of foreign vaccines like Sputnik V. This underscores the dual role of countries as both producers and consumers, with strategic decisions influenced by manufacturing capacity, population size, and diplomatic ties.
Analyzing these trends reveals a clear correlation between economic strength and vaccine procurement. High-income countries often secured deals directly with manufacturers, bypassing COVAX and creating a "vaccine apartheid." For example, the European Union collectively ordered over 2 billion doses, ensuring member states had access to multiple vaccine types. Meanwhile, middle-income countries like Brazil and Mexico adopted hybrid strategies, combining direct purchases with COVAX allocations to balance cost and supply reliability. This tiered approach to procurement exacerbated global inequities, leaving poorer nations at a disadvantage.
Practical takeaways from these strategies include the importance of early investment in vaccine development and manufacturing partnerships. Countries that engaged in advance purchase agreements (APAs) with multiple manufacturers were better insulated from production delays. Additionally, diversifying vaccine portfolios—as seen in the UK’s orders of Pfizer, AstraZeneca, and Moderna doses—provided flexibility in addressing variant-specific challenges. For nations still navigating vaccine procurement, prioritizing transparency in contracts and collaborating with regional blocs can mitigate risks and improve access.
Ultimately, the top countries by vaccine orders illustrate a blend of foresight, financial muscle, and strategic diplomacy. While over-procurement by wealthy nations ensured security, it also raised ethical questions about global equity. Moving forward, lessons from this pandemic emphasize the need for a more coordinated, inclusive approach to vaccine distribution, ensuring that no country is left behind in future health crises.
RNA vs. DNA Vaccines: Key Differences and How They Work
You may want to see also
Explore related products






![]()
Low-income nations' vaccine access
The COVID-19 pandemic exposed a stark divide in global vaccine access, with low-income nations often left behind in the race to secure doses. While high-income countries pre-ordered enough vaccines to cover their populations multiple times over, many low-income nations struggled to secure even a single dose per person. For instance, as of early 2021, Canada had ordered enough vaccines to cover its population nearly six times, whereas many African countries had secured fewer than 20 doses per 100 people. This disparity highlights the urgent need for equitable distribution mechanisms.
One of the primary challenges for low-income nations is the financial barrier to purchasing vaccines. With limited budgets, these countries often cannot compete with wealthier nations in the global vaccine market. The COVAX initiative, a global collaboration to ensure equitable vaccine access, aimed to address this by pooling resources and negotiating prices. However, COVAX faced significant funding shortfalls and supply chain disruptions, leaving many low-income nations with delayed or insufficient deliveries. For example, by mid-2021, COVAX had delivered only 10% of the doses it promised to low-income countries, forcing them to rely on donations from wealthier nations.
Another critical issue is the logistical complexity of vaccine distribution in low-income settings. Many of these countries lack the infrastructure for cold-chain storage, particularly for mRNA vaccines that require ultra-low temperatures. This limitation often forces them to rely on less effective or harder-to-store vaccines. For instance, the AstraZeneca vaccine, which can be stored at standard refrigerator temperatures, became a lifeline for many low-income nations, even as wealthier countries shifted to mRNA options. Practical solutions, such as investing in solar-powered refrigerators and training local healthcare workers, are essential to overcome these hurdles.
To improve vaccine access in low-income nations, a multi-faceted approach is necessary. Wealthier countries must fulfill their dose-sharing pledges and support initiatives like COVAX with both funding and surplus vaccines. Pharmaceutical companies should also waive intellectual property rights temporarily to enable local production in low-income regions. For instance, the World Health Organization’s mRNA technology transfer hub in South Africa is a step in this direction, aiming to build vaccine manufacturing capacity in Africa. Additionally, low-income nations should prioritize vaccinating high-risk groups, such as the elderly and healthcare workers, with available doses, even if full population coverage remains out of reach.
Ultimately, the vaccine access gap is not just a moral failure but a global health risk. As long as the virus circulates unchecked in low-income nations, new variants can emerge, threatening progress worldwide. Addressing this disparity requires immediate action, innovative solutions, and a commitment to global solidarity. Without it, the pandemic’s impact will continue to disproportionately burden the world’s most vulnerable populations.
Skipping Vaccines: The Ripple Effect on Public Health and Safety
You may want to see also
Explore related products






![]()
Regional vaccine procurement trends
The global distribution of COVID-19 vaccines has revealed distinct regional procurement trends, shaped by economic power, geopolitical alliances, and public health infrastructure. High-income countries in North America and Europe, such as the United States and Germany, secured billions of doses early through advance purchase agreements with manufacturers like Pfizer-BioNTech and Moderna. For instance, the U.S. ordered over 1.5 billion doses, enough to vaccinate its population multiple times and donate surplus doses globally. This aggressive procurement strategy highlights the ability of wealthy nations to prioritize their populations while influencing global vaccine availability.
In contrast, low- and middle-income countries in Africa and Southeast Asia faced significant challenges in securing sufficient doses. Many relied on the COVAX initiative, a global vaccine-sharing mechanism, which aimed to provide equitable access but fell short of its targets. For example, as of late 2021, African countries had received only about 20% of the doses needed to fully vaccinate their populations. This disparity underscores the limitations of global solidarity mechanisms and the need for regional self-sufficiency in vaccine production. Countries like South Africa and India have since invested in local manufacturing capabilities to reduce dependency on imports.
Latin America presents a mixed picture, with countries like Brazil and Chile securing early doses through bilateral deals, while others struggled due to financial constraints. Brazil, for instance, ordered over 500 million doses, including AstraZeneca and Sinovac, but faced logistical challenges in distribution. Smaller nations, such as Honduras and Paraguay, relied heavily on donations from wealthier countries and COVAX. This regional trend highlights the importance of economic stability and diplomatic relationships in vaccine procurement, as well as the need for coordinated regional strategies to address disparities.
The Middle East and Gulf states adopted a unique approach, leveraging their financial resources to secure diverse vaccine portfolios. The United Arab Emirates ordered doses from multiple suppliers, including Sinopharm, Pfizer, and Sputnik V, ensuring flexibility in their vaccination campaigns. Israel, a global leader in vaccination rates, secured early access to Pfizer doses through a data-sharing agreement, administering over 17 million doses to its population of 9 million. This region’s strategy demonstrates how financial capacity and innovative agreements can overcome supply chain limitations, offering lessons in proactive procurement for other regions.
Practical takeaways from these trends include the need for diversified sourcing strategies, investment in local manufacturing, and strengthened regional collaborations. Countries should assess their population size, age distribution, and storage capabilities when ordering vaccines. For example, mRNA vaccines like Pfizer require ultra-cold storage, making them less suitable for regions with limited infrastructure. By studying regional trends, nations can better navigate future health crises, ensuring equitable and efficient vaccine distribution.
Are You Contagious After the MMR Vaccine? Facts and Myths
You may want to see also
Explore related products






![]()
Impact of COVAX on orders
The COVAX initiative, led by Gavi, the Vaccine Alliance, aimed to ensure equitable access to COVID-19 vaccines, particularly for low- and middle-income countries (LMICs). Its impact on global vaccine orders is evident in the redistribution of purchasing power, where wealthier nations, which initially dominated vaccine procurement, were encouraged to share doses. For instance, by mid-2021, high-income countries had secured over 6 billion doses, while LMICs struggled to access even 10% of that volume. COVAX stepped in by pooling funds and negotiating deals, enabling 92 LMICs to receive vaccines without direct orders. This mechanism effectively reduced the hoarding of vaccines by wealthy nations, as COVAX’s collective bargaining power allowed it to secure 1.3 billion doses by the end of 2021, primarily from manufacturers like AstraZeneca and Pfizer.
Analyzing the data reveals a shift in ordering behavior due to COVAX. Countries like Canada and the UK, which initially ordered doses exceeding their population needs (e.g., Canada ordered 8 doses per capita), began donating excess supplies to COVAX. This redistribution was critical for LMICs, where vaccination rates were as low as 3% in some African nations in late 2021. However, COVAX’s impact was limited by supply chain delays and vaccine nationalism. For example, India’s Serum Institute, a key supplier, faced export bans, delaying COVAX deliveries by months. Despite these challenges, COVAX’s presence forced a reevaluation of global vaccine orders, pushing countries to consider equity in their procurement strategies.
From a practical standpoint, COVAX’s influence extended beyond orders to dosage strategies. In LMICs, where cold chain infrastructure is limited, COVAX prioritized vaccines like AstraZeneca, which require standard refrigeration (2–8°C), over mRNA vaccines needing ultra-cold storage. This decision influenced how countries placed orders, with many LMICs relying on COVAX for 70–80% of their vaccine supply. For instance, Ghana received 600,000 AstraZeneca doses through COVAX, targeting adults aged 18–59, while wealthier nations focused on booster campaigns for all age groups. This highlights how COVAX shaped not just the quantity but also the type and allocation of vaccines ordered globally.
Persuasively, COVAX’s role in vaccine orders underscores the need for global solidarity in health crises. Without it, LMICs would have faced even greater disparities, prolonging the pandemic. For instance, Rwanda, which received 40% of its vaccines through COVAX, vaccinated 60% of its population by mid-2022, compared to 3% in non-COVAX-supported nations. This success demonstrates that equitable distribution, not just individual country orders, is key to controlling pandemics. Moving forward, COVAX’s model should be institutionalized, ensuring that future vaccine orders are coordinated globally, with binding commitments from wealthy nations to share doses and resources. This approach would mitigate the impact of vaccine nationalism and save lives worldwide.
Hepatitis B Vaccine vs. Past Infection: Key Differences Explained
You may want to see also
Frequently asked questions
You can find information on vaccine orders by country through various sources such as the World Health Organization (WHO), UNICEF, and Our World in Data. These organizations provide regularly updated data on vaccine distribution and orders globally.
As of my knowledge cutoff in October 2023, countries like the United States, the European Union (as a bloc), the United Kingdom, Canada, and Australia have been among the largest procurers of COVID-19 vaccines. However, the exact numbers can vary over time due to new agreements and deliveries.
No, access to vaccines is not equal across all countries. Factors such as economic status, manufacturing capacity, and distribution logistics play significant roles. Initiatives like COVAX aim to ensure equitable access, but wealthier nations often secure larger quantities through direct deals with manufacturers.