Childhood vaccination schedules are carefully designed to protect children from a range of serious and potentially life-threatening diseases. The number of vaccines a child receives can vary depending on their age, health status, and geographic location, but in the United States, the Centers for Disease Control and Prevention (CDC) recommends a comprehensive schedule that typically includes vaccines against 14 different diseases by the age of 2. These vaccines, such as those for measles, mumps, rubella, polio, and whooping cough, are administered in multiple doses over time to ensure optimal protection. While the number of vaccines may seem high, they are rigorously tested and proven safe, and their benefits in preventing illness and saving lives far outweigh the minimal risks associated with vaccination.
Explore related products






What You'll Learn
- Vaccine Schedule Overview: Standard timeline for childhood vaccinations from birth to adolescence
- Common Childhood Vaccines: List of essential vaccines (e.g., MMR, DTaP, polio)
- Vaccine Safety: Addressing concerns about side effects and long-term safety
- Mandatory vs. Optional: Differences in required and recommended vaccines by region
- Vaccine Effectiveness: How well vaccines protect children from targeted diseases
![]()
Vaccine Schedule Overview: Standard timeline for childhood vaccinations from birth to adolescence
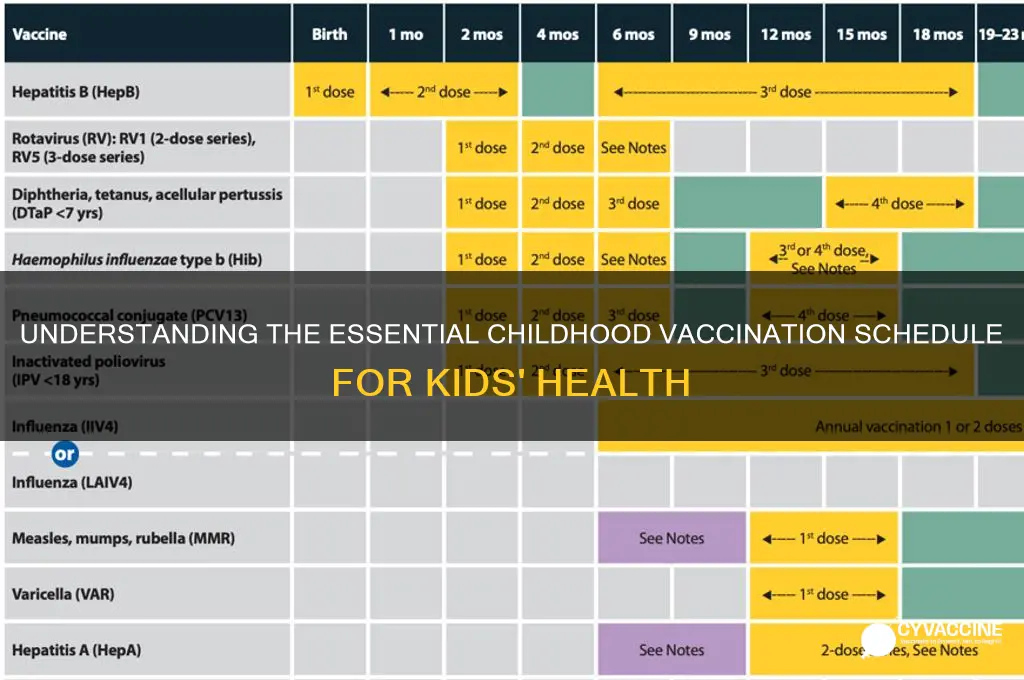
Childhood vaccinations follow a carefully structured schedule designed to protect against serious diseases at the most vulnerable stages of life. From birth to adolescence, this timeline ensures immunity builds when it’s needed most, aligning with a child’s developing immune system. The Centers for Disease Control and Prevention (CDC) and the American Academy of Pediatrics (AAP) jointly recommend a standardized schedule, which includes vaccines like hepatitis B, DTaP (diphtheria, tetanus, pertussis), and IPV (polio) starting at just hours old. Booster doses and additional vaccines are layered in during infancy, early childhood, and preadolescence to maintain protection.
The first year of life is critical, with multiple vaccines administered in a series. At 2 months, infants receive their first doses of DTaP, IPV, Hib (Haemophilus influenzae type b), PCV13 (pneumococcal conjugate), and rotavirus vaccines. This is followed by repeat doses at 4 and 6 months, ensuring robust immunity. The MMR (measles, mumps, rubella) and varicella (chickenpox) vaccines typically begin at 12 months, though some providers may split the doses for closer monitoring. Parents should track these appointments closely, as delays can leave children susceptible to outbreaks.
As children transition into early childhood, booster shots reinforce immunity. Between 4 and 6 years old, they receive DTaP, IPV, MMR, and varicella boosters, often before starting school. This age is also when the flu vaccine becomes an annual requirement, ideally administered by the end of October. Schools frequently mandate proof of these vaccinations, making adherence essential for enrollment. Parents can use immunization records or apps to stay organized, ensuring no dose is missed.
Adolescence introduces new vaccines tailored to emerging health risks. At 11–12 years, preteens receive Tdap (tetanus, diphtheria, pertussis) to replace the childhood DTaP series, along with meningococcal conjugate (MenACWY) and HPV (human papillomavirus) vaccines. The HPV vaccine, given in 2–3 doses depending on age, is particularly crucial for cancer prevention. A final MenACWY dose is recommended at 16 years. Parents should discuss these vaccines with teens, emphasizing their role in long-term health and disease prevention.
Practical tips can ease the vaccination process for families. Scheduling appointments during calm times of day and bringing a favorite toy or book can distract younger children. For teens, framing vaccines as a step toward independence and self-care can increase cooperation. Pharmacies and school-based clinics often offer convenient options for flu and other routine shots. Staying informed about updates to the vaccine schedule ensures children receive the fullest protection possible, safeguarding both individual and community health.
AstraZeneca Vaccine: Efficacy, Safety, and Global Impact Explained
You may want to see also
Explore related products






![]()
Common Childhood Vaccines: List of essential vaccines (e.g., MMR, DTaP, polio)
Children typically receive a series of vaccines during their early years to protect against serious, preventable diseases. These vaccines are carefully scheduled to ensure maximum efficacy and safety, often starting as early as birth and continuing through adolescence. Among the most critical are the MMR (Measles, Mumps, Rubella), DTaP (Diphtheria, Tetanus, Pertussis), and polio vaccines, which form the backbone of childhood immunization programs worldwide. Each vaccine targets specific pathogens, and their administration follows a precise timeline to build immunity when children are most vulnerable.
The MMR vaccine is a cornerstone of childhood immunization, administered in two doses: the first at 12–15 months and the second at 4–6 years. This vaccine prevents measles, a highly contagious virus that can lead to pneumonia, encephalitis, and even death; mumps, which can cause deafness and meningitis; and rubella, known for its severe risks to pregnant women and their fetuses. Despite occasional misinformation, decades of research confirm the MMR vaccine’s safety and effectiveness, with mild side effects like fever or rash being rare and short-lived.
Another essential vaccine is the DTaP, which protects against diphtheria, tetanus, and pertussis (whooping cough). Infants receive a series of five doses starting at 2 months, with boosters at 4–6 years and again at 11–12 years. Pertussis, in particular, poses a grave risk to young children, causing violent coughing fits that can lead to pneumonia or seizures. Tetanus, though rare in developed countries, remains a threat through contaminated wounds, while diphtheria can cause severe respiratory issues. The DTaP vaccine’s efficacy underscores its importance in preventing these life-threatening diseases.
Polio vaccination has nearly eradicated this once-feared disease globally, thanks to the inactivated poliovirus vaccine (IPV). Children receive four doses: at 2 months, 4 months, 6–18 months, and 4–6 years. Polio can cause paralysis or death, but the IPV has proven 99% effective in preventing infection. Its success highlights the power of vaccination in eliminating diseases that once crippled thousands annually. Parents should ensure timely administration, as delays can leave children susceptible during outbreaks.
Practical tips for parents include keeping a detailed immunization record, scheduling appointments well in advance, and discussing any concerns with healthcare providers. Mild side effects like soreness or low-grade fever are normal and can be managed with over-the-counter pain relievers. Most importantly, adhering to the recommended vaccine schedule ensures children are protected during critical developmental stages. By prioritizing these essential vaccines, parents play a vital role in safeguarding their children’s health and contributing to community immunity.
MMR Vaccine Schedule: Understanding the Timing Between Doses
You may want to see also
Explore related products






![]()
Vaccine Safety: Addressing concerns about side effects and long-term safety
Children in the United States typically receive up to 16 different vaccines by age 18, protecting against 14 potentially serious diseases. This comprehensive schedule, recommended by the CDC, sparks understandable concern about side effects and long-term safety. While vaccines are rigorously tested before approval, ongoing monitoring systems like VAERS (Vaccine Adverse Event Reporting System) and VSD (Vaccine Safety Datalink) continuously track potential issues.
Understanding Common Side Effects: Most vaccine reactions are mild and short-lived. For example, the MMR vaccine (measles, mumps, rubella) can cause fever in 5-15% of recipients, typically within 7-12 days. The DTaP shot (diphtheria, tetanus, pertussis) may lead to soreness at the injection site in 1 out of 4 children. These reactions are a sign the immune system is responding, not a cause for alarm. Severe allergic reactions are extremely rare, occurring in about 1 in a million doses.
Long-Term Safety: A Record of Reassurance: Decades of research consistently demonstrate the long-term safety of vaccines. Studies involving millions of children have found no link between vaccines and chronic conditions like autism, asthma, or diabetes. For instance, a 2019 study published in *Annals of Internal Medicine* analyzed data from over 650,000 children and found no increased risk of autism associated with the MMR vaccine.
Addressing Specific Concerns: Some parents worry about the number of vaccines given simultaneously. However, the immune system routinely encounters hundreds of foreign substances daily. Vaccines contain a tiny fraction of these antigens, and combination vaccines (like MMR) have been proven safe and effective. Empowering Informed Decisions: Open communication with healthcare providers is crucial. Parents should ask questions, express concerns, and seek reliable information from trusted sources like the CDC, WHO, and AAP. Remember, the benefits of vaccination in preventing serious diseases far outweigh the minimal risks.
H1N1 Vaccine: Does It Offer Protection Against H5N1 Strain?
You may want to see also
Explore related products

$26.59 $32.99





![]()
Mandatory vs. Optional: Differences in required and recommended vaccines by region
The number of vaccines children receive varies widely by region, influenced by local health policies, disease prevalence, and cultural attitudes. In the United States, for instance, the Centers for Disease Control and Prevention (CDC) recommends a comprehensive schedule that includes vaccines like MMR (measles, mumps, rubella), DTaP (diphtheria, tetanus, pertussis), and IPV (inactivated polio vaccine) starting at 2 months of age. However, not all of these are mandatory for school entry; requirements differ by state, with some allowing exemptions for medical, religious, or philosophical reasons. This contrast between recommended and required vaccines highlights the tension between public health goals and individual choice.
In contrast, countries like Australia and Germany take a stricter approach, mandating a broader range of vaccines for school attendance. Australia’s National Immunisation Program (NIP) includes vaccines for diseases such as hepatitis B, pneumococcal disease, and varicella (chickenpox), with some states offering financial incentives for compliance. Germany, while historically more lenient, has tightened its policies in recent years, requiring proof of vaccination against measles for school and daycare enrollment. These regional differences underscore how cultural and political contexts shape vaccine mandates, often reflecting societal priorities around collective immunity versus personal autonomy.
Mandatory vaccines typically target highly contagious diseases with severe outcomes, such as measles or polio, where herd immunity is critical. For example, the MMR vaccine is required in many regions because measles outbreaks can spread rapidly in unvaccinated populations, posing risks even to those who cannot be vaccinated due to medical reasons. Recommended vaccines, on the other hand, often address diseases with lower transmission rates or milder symptoms, like hepatitis A or rotavirus. Parents in regions with optional vaccines must weigh the benefits of protection against these diseases against factors like cost, side effects, and perceived necessity.
Practical considerations further complicate the mandatory vs. optional divide. In low-income regions, access to even recommended vaccines may be limited by supply chain issues or healthcare infrastructure, making mandates less feasible. Wealthier regions, meanwhile, may face challenges with vaccine hesitancy, where optional vaccines are skipped due to misinformation or distrust. For instance, the HPV vaccine, recommended for adolescents to prevent cervical cancer and other cancers, has lower uptake in some countries despite its proven efficacy, partly due to misconceptions about its safety and necessity.
Ultimately, the distinction between mandatory and recommended vaccines reflects a balance between public health imperatives and individual rights, shaped by regional realities. Parents navigating these differences should consult local health guidelines, consider disease prevalence in their area, and discuss concerns with healthcare providers. While mandatory vaccines provide a baseline of protection for communities, recommended vaccines offer additional layers of defense, particularly for vulnerable populations. Understanding these distinctions empowers families to make informed decisions tailored to their child’s needs and their region’s health landscape.
Florida's Monkeypox Vaccine Eligibility: Who Qualifies for Protection?
You may want to see also
Explore related products






![]()
Vaccine Effectiveness: How well vaccines protect children from targeted diseases
Children typically receive up to 14 different vaccines by age 6, targeting diseases like measles, mumps, polio, and whooping cough. While this number may seem high, it’s a carefully calibrated schedule designed to build immunity during critical developmental stages. Vaccine effectiveness, however, isn’t a one-size-fits-all metric. For instance, the measles vaccine is 97% effective after two doses, while the flu vaccine’s effectiveness varies annually, ranging from 40% to 60% depending on the strain match. Understanding these variations is key to appreciating how vaccines safeguard children’s health.
Consider the dosage and timing of vaccines, which play a pivotal role in their effectiveness. The DTaP vaccine (diphtheria, tetanus, pertussis) requires five doses between 2 months and 6 years of age to achieve 80-85% protection against pertussis. Skipping doses or delaying the schedule can leave children vulnerable during critical periods. Similarly, the HPV vaccine, administered in two or three doses depending on age, is nearly 100% effective in preventing cervical cancer precursors when given before exposure to the virus. Adhering to recommended schedules ensures maximum protection without overburdening the immune system.
A comparative analysis of vaccine effectiveness reveals striking contrasts. The chickenpox vaccine, for example, is 98% effective in preventing severe disease, even though mild breakthrough cases can occur. In contrast, the rotavirus vaccine reduces severe diarrhea hospitalizations by 85-98%, but its effectiveness can wane in low-resource settings due to environmental factors. These disparities highlight the interplay between vaccine design, delivery, and local conditions. Parents should consult healthcare providers to understand how these factors might affect their child’s protection.
Practical tips can enhance vaccine effectiveness. Ensure children are well-hydrated and rested before vaccinations to minimize side effects. Keep a record of vaccine dates and doses to avoid gaps in immunity. For vaccines like the flu shot, annual administration is essential due to evolving strains. Additionally, combining vaccines (e.g., MMR and varicella) at a single visit reduces clinic trips without compromising effectiveness. Addressing concerns with evidence-based information can also alleviate hesitancy, ensuring children receive full protection.
Finally, real-world data underscores the impact of vaccine effectiveness. Before the Hib vaccine, *Haemophilus influenzae* type b caused 20,000 severe infections annually in U.S. children; today, cases are virtually nonexistent. Similarly, global polio cases have dropped by 99.9% since 1988, thanks to widespread vaccination. These successes demonstrate that vaccines not only protect individuals but also contribute to herd immunity, shielding vulnerable populations. By understanding and trusting vaccine effectiveness, parents play a vital role in sustaining these achievements for future generations.
Hepatitis B Vaccines for Infants: Are They Mandatory in Bunei?
You may want to see also
Frequently asked questions
Children typically receive about 20-25 vaccine doses by the age of 2, protecting against 10-14 different diseases, depending on the vaccination schedule and country-specific recommendations.
Not all childhood vaccines are mandatory, as requirements vary by country, state, or region. Some vaccines are recommended but not legally required, while others may be necessary for school entry.
Yes, children can safely receive multiple vaccines in one visit. Combining vaccines reduces the number of visits and ensures timely protection against preventable diseases.
Newborns typically receive their first vaccine, the hepatitis B vaccine, within 24 hours of birth. Some countries also administer the BCG vaccine for tuberculosis at this stage.