The number of vaccines recommended by each country varies significantly due to differences in public health priorities, disease prevalence, and healthcare infrastructure. For instance, high-income countries like the United States and those in Western Europe often recommend a comprehensive vaccination schedule covering diseases such as measles, mumps, rubella, influenza, and HPV, totaling around 14-16 vaccines from infancy to adulthood. In contrast, low- and middle-income countries may prioritize vaccines for diseases more prevalent in their regions, such as yellow fever or tuberculosis, while potentially offering fewer optional vaccines due to resource constraints. Additionally, global initiatives like the World Health Organization’s Expanded Programme on Immunization (EPI) provide a baseline for essential vaccines, but individual countries adapt these recommendations based on local needs, resulting in diverse vaccination schedules worldwide.
Explore related products






What You'll Learn
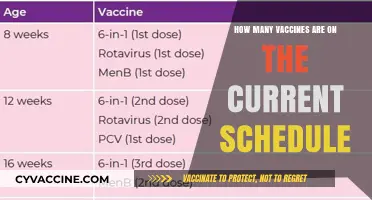
- Vaccine Schedules by Age: Countries outline specific vaccines for different age groups, from infants to seniors
- Mandatory vs. Recommended: Some vaccines are compulsory, while others are strongly advised but optional
- Regional Disease Prevalence: Local disease risks influence which vaccines are prioritized in each country
- Travel-Related Vaccines: Additional vaccines may be recommended for travelers to certain regions
- Vaccine Availability: Recommendations depend on access to specific vaccines in each country
![]()
Vaccine Schedules by Age: Countries outline specific vaccines for different age groups, from infants to seniors
Vaccine schedules vary significantly across countries, tailored to local disease prevalence, public health priorities, and healthcare infrastructure. For infants and young children, most countries prioritize vaccines that protect against life-threatening diseases. For instance, the United States, through the Centers for Disease Control and Prevention (CDC), recommends a series of vaccines starting at birth, including hepatitis B, followed by doses of DTaP (diphtheria, tetanus, pertussis), Hib (Haemophilus influenzae type b), pneumococcal conjugate vaccine (PCV), and polio vaccine by 2 months of age. Similarly, the UK’s National Health Service (NHS) schedules vaccines like the 6-in-1 vaccine (diphtheria, tetanus, pertussis, polio, hepatitis B, and Hib), rotavirus, and meningitis B for infants. Many countries also include BCG (tuberculosis) at birth, particularly in regions with high TB prevalence.
As children grow, school-age vaccine schedules expand to include boosters and additional vaccines. In the U.S., children around 4-6 years old receive boosters for DTaP, polio, MMR (measles, mumps, rubella), and varicella (chickenpox). Countries like Canada and Australia follow similar patterns, with some variations based on regional needs. For example, Australia includes the HPV vaccine for both boys and girls around 12-13 years old, while some European countries offer it only to girls. Japan, on the other hand, has historically had a more conservative approach to vaccines, with fewer mandatory requirements, though recent years have seen expansions in recommended vaccines.
Adolescents and young adults are targeted for vaccines that address diseases prevalent in their age group. The HPV vaccine is widely recommended globally to prevent cervical cancer and other HPV-related diseases. Many countries also recommend the Tdap booster (tetanus, diphtheria, pertussis) during adolescence. In the U.S., the meningococcal conjugate vaccine (MenACWY) is advised for preteens and teens, while some European countries include it in their schedules for older adolescents. Additionally, countries with a history of outbreaks, such as mumps or measles, may recommend additional MMR doses during this period.
For adults, vaccine schedules focus on maintaining immunity and preventing diseases that become more relevant with age. Most countries recommend a Td (tetanus, diphtheria) or Tdap booster every 10 years. Influenza vaccination is widely advised annually for adults, especially those with chronic conditions or over 65. Pneumococcal vaccines (PPSV23 and PCV15/PCV20) are also recommended for older adults in many countries, including the U.S. and the UK, to prevent pneumonia and other invasive diseases. In regions with higher risks, vaccines like hepatitis A and B, typhoid, or rabies may be included for specific populations.
Seniors receive tailored vaccine recommendations to address age-related immune decline. In addition to annual flu shots and pneumococcal vaccines, many countries recommend shingles (herpes zoster) vaccination for adults over 50 or 60. The U.S. and Canada, for example, advise the recombinant zoster vaccine (Shingrix) for this age group. Some countries also emphasize the importance of COVID-19 vaccination and boosters for older adults, given their higher risk of severe illness. In Japan and South Korea, where aging populations are significant, vaccine schedules for seniors are particularly comprehensive, often including additional doses of influenza and pneumococcal vaccines.
Overall, vaccine schedules by age reflect a global effort to protect individuals throughout their lives, with each country adapting its recommendations to address specific health challenges. While core vaccines like DTaP, MMR, and polio are universally recommended, variations in additional vaccines highlight the importance of local disease patterns and public health strategies. Understanding these schedules is crucial for ensuring optimal protection across all age groups.
Measles Myth: Vaccines and the Source of Outbreaks
You may want to see also
Explore related products





![]()
Mandatory vs. Recommended: Some vaccines are compulsory, while others are strongly advised but optional
The distinction between mandatory and recommended vaccines is a critical aspect of public health policies worldwide, reflecting each country's approach to disease prevention and individual autonomy. Mandatory vaccines are legally required, often for school entry, employment in certain sectors, or travel, and non-compliance can result in penalties such as fines or exclusion from activities. For instance, countries like the United States, Italy, and Australia have mandatory vaccination policies for diseases like measles, mumps, and rubella (MMR), particularly for children attending public schools. These vaccines are deemed essential for herd immunity and the eradication of highly contagious diseases. In contrast, recommended vaccines are strongly advised by health authorities but not legally enforced. Examples include the annual influenza vaccine or the HPV vaccine, which are encouraged to prevent widespread illness but remain optional. This distinction often depends on the severity of the disease, the availability of the vaccine, and cultural or societal attitudes toward vaccination.
The number of vaccines recommended by each country varies significantly based on factors such as disease prevalence, healthcare infrastructure, and public health priorities. For example, high-income countries like the United States and Canada recommend a comprehensive list of vaccines, including those for hepatitis A and B, varicella, and pneumococcal disease, in addition to the core childhood vaccines. In contrast, low-income countries may prioritize vaccines for diseases like tuberculosis (BCG) and yellow fever due to higher prevalence rates. The World Health Organization (WHO) provides global guidelines, but individual countries adapt these recommendations to their specific needs. Recommended vaccines often target diseases that, while not eradicated, are less immediately threatening or have lower transmission rates, allowing individuals to make informed choices based on personal risk factors.
Mandatory vaccination policies are often implemented for vaccines with proven efficacy in preventing diseases that pose significant public health risks. For example, many European countries mandate vaccines like MMR and diphtheria-tetanus-pertussis (DTP) to maintain high vaccination rates and prevent outbreaks. However, these policies are not without controversy. Some argue that mandatory vaccination infringes on personal freedoms, while others emphasize the collective benefit of herd immunity. In countries like France and Germany, public debates have led to stricter mandates, while in others, like Sweden and the Netherlands, a more voluntary approach is favored, with strong public trust in health authorities driving high vaccination rates.
Recommended vaccines, on the other hand, rely on public awareness and trust in healthcare systems to achieve high uptake. For instance, the COVID-19 vaccine has been mandatory in some countries, such as Austria and Indonesia, for certain age groups or professions, while in others, like the United Kingdom and Japan, it has been strongly recommended but optional. This approach allows for flexibility, particularly in addressing vaccine hesitancy or logistical challenges. Health campaigns, accessible healthcare services, and incentives are often used to promote recommended vaccines, ensuring that individuals understand the benefits and make voluntary decisions to protect themselves and their communities.
Ultimately, the balance between mandatory and recommended vaccines reflects a country's public health strategy and societal values. While mandatory vaccines ensure high coverage for critical diseases, recommended vaccines empower individuals to take responsibility for their health based on personal and community risks. Global trends show a shift toward more personalized vaccination schedules, with countries increasingly tailoring their recommendations to demographic and regional factors. Understanding these distinctions is essential for policymakers, healthcare providers, and the public to navigate the complexities of vaccination programs and achieve optimal health outcomes.
Vaccinated Mothers Pass Antibodies to Newborns
You may want to see also
Explore related products






![]()
Regional Disease Prevalence: Local disease risks influence which vaccines are prioritized in each country
The number of vaccines recommended by each country is heavily influenced by regional disease prevalence, as local health authorities prioritize immunizations that address the most significant public health threats in their area. For instance, countries in sub-Saharan Africa often include the yellow fever vaccine in their routine immunization schedules due to the endemic nature of the disease in these regions. Similarly, nations in Southeast Asia may prioritize vaccines against Japanese encephalitis, a mosquito-borne virus prevalent in rural agricultural areas. This tailored approach ensures that limited healthcare resources are allocated efficiently to combat the most pressing disease risks.
In contrast, countries with temperate climates, such as those in Northern Europe, may place less emphasis on vaccines for tropical diseases like yellow fever or dengue fever. Instead, their immunization programs focus on diseases like influenza, measles, mumps, and rubella (MMR), which pose a higher risk in densely populated urban areas with colder climates. For example, annual flu vaccination campaigns are a cornerstone of public health strategies in these regions due to the seasonal nature of influenza outbreaks. This demonstrates how regional disease patterns directly shape vaccine prioritization.
Tropical and subtropical regions often face a higher burden of vaccine-preventable diseases due to factors like climate, vector prevalence, and population density. Countries in these areas, such as India and Brazil, typically recommend vaccines against cholera, typhoid, and hepatitis A, which are more common due to challenges in water sanitation and food safety. Additionally, the introduction of vaccines like the dengue vaccine in endemic countries, such as the Philippines and Mexico, reflects a targeted response to local disease risks. These decisions are guided by epidemiological data and the need to reduce disease morbidity and mortality.
In regions with a history of specific outbreaks, vaccines are prioritized to prevent future epidemics. For example, the meningitis A vaccine is a critical component of immunization programs in the African "meningitis belt," a region stretching from Senegal to Ethiopia where outbreaks of meningococcal meningitis are frequent. Similarly, countries in the Middle East and parts of Asia include the polio vaccine in their schedules due to ongoing risks of poliovirus transmission, despite global eradication efforts. This localized approach ensures that vaccines are deployed where they can have the greatest impact.
Finally, economic and geographic factors also play a role in vaccine prioritization based on regional disease prevalence. Wealthier nations with robust healthcare systems may offer a broader range of vaccines, including those for less common diseases like shingles or human papillomavirus (HPV), as part of their public health programs. In contrast, low-income countries often focus on essential vaccines provided through initiatives like Gavi, the Vaccine Alliance, targeting diseases like measles, polio, and tuberculosis. This disparity highlights the importance of global collaboration to address regional disease risks and ensure equitable access to life-saving vaccines.
Unvaccinated Autistic Children: A Rare but Real Phenomenon
You may want to see also
Explore related products






![]()
Travel-Related Vaccines: Additional vaccines may be recommended for travelers to certain regions
When planning international travel, it's crucial to consider travel-related vaccines, as different regions may pose specific health risks that are not typically addressed by routine immunizations. These additional vaccines are recommended based on factors such as destination, duration of stay, type of travel, and individual health status. For instance, travelers to sub-Saharan Africa or South America may need protection against yellow fever, a vaccine often required for entry into certain countries in these regions. Similarly, Japanese encephalitis vaccination is advised for those visiting rural areas of Southeast Asia or the Pacific Islands, especially during peak transmission seasons.
Another critical travel-related vaccine is meningococcal meningitis, particularly for travelers to the meningitis belt in Africa, which spans from Senegal to Ethiopia. Pilgrims to Saudi Arabia for the Hajj or Umrah are also required to show proof of meningococcal vaccination. Additionally, rabies vaccination may be recommended for travelers engaging in outdoor activities in regions with high rabies prevalence, such as parts of Asia, Africa, and Central or South America. While rabies is rare in travelers, pre-exposure vaccination is advised for those with potential animal contact, such as hikers or veterinarians.
Typhoid and hepatitis A vaccines are commonly recommended for travelers to developing countries with poor sanitation or limited access to clean water. These vaccines are particularly important for those visiting rural areas or staying with local families. In contrast, cholera vaccination is less frequently required but may be advised for travelers to areas with active outbreaks, such as parts of Africa, Haiti, or certain regions in Asia. It's essential to consult with a healthcare provider or travel clinic to determine which vaccines are necessary based on your itinerary.
For travelers to tropical regions, malaria prophylaxis is not a vaccine but a critical preventive measure. However, some countries may recommend vaccines like dengue in areas with high transmission rates, such as Southeast Asia, the Pacific Islands, or Latin America. Dengue vaccination is typically considered for individuals with previous dengue infection, as it can pose risks to those without prior exposure. Similarly, tick-borne encephalitis vaccination may be advised for travelers to forested areas of Central and Eastern Europe or parts of Asia during tick season.
Lastly, the COVID-19 vaccine and its boosters remain essential for international travel, with many countries requiring proof of vaccination for entry or to avoid quarantine. Additionally, influenza vaccination is recommended for travelers, especially during flu season in their destination country. It's important to plan ahead, as some travel-related vaccines require multiple doses or take time to become effective. Resources like the World Health Organization (WHO) and the Centers for Disease Control and Prevention (CDC) provide country-specific vaccine recommendations, ensuring travelers are adequately protected against region-specific health risks. Always consult a healthcare professional at least 4-6 weeks before departure to ensure timely vaccination and a safe journey.
DNA Vaccines: How They Train Your Body to Fight Future Diseases
You may want to see also
Explore related products





![]()
Vaccine Availability: Recommendations depend on access to specific vaccines in each country
The number of vaccines recommended by a country is deeply intertwined with the availability of those vaccines within its borders. Vaccine availability is a critical factor that shapes national immunization schedules, as countries can only recommend vaccines that are accessible, affordable, and approved for use. For instance, high-income countries often have robust healthcare systems and purchasing power, allowing them to offer a broader range of vaccines, including those for diseases like rotavirus, human papillomavirus (HPV), and meningococcal meningitis. In contrast, low- and middle-income countries may prioritize essential vaccines such as those for measles, polio, and tuberculosis, due to limited resources and supply chain constraints. This disparity highlights how vaccine availability directly influences the scope of recommendations.
Global initiatives like Gavi, the Vaccine Alliance, play a pivotal role in improving vaccine availability in low-income countries by providing funding and support for vaccine procurement. However, even with such assistance, the range of vaccines recommended in these countries remains narrower compared to wealthier nations. For example, while most high-income countries include the HPV vaccine in their routine immunization schedules, many low-income countries still struggle to introduce it due to high costs and limited supply. This underscores the reality that recommendations are not just based on public health needs but also on the practicalities of vaccine access.
The manufacturing capacity and distribution networks of vaccine producers also impact availability. Countries with strong domestic pharmaceutical industries or strategic partnerships with global manufacturers often have better access to a wider array of vaccines. Conversely, nations reliant on imports may face delays or shortages, particularly during global health crises like the COVID-19 pandemic, when demand outstrips supply. As a result, their vaccine recommendations may be more conservative, focusing on core vaccines that are consistently available.
Another factor influencing vaccine availability is regulatory approval. Before a vaccine can be recommended for use, it must be approved by the country’s health regulatory authority. This process can vary significantly in duration and rigor across countries, affecting when and if a vaccine becomes available. For instance, a vaccine approved and widely used in Europe or the United States may take years to gain approval in other regions, delaying its inclusion in national immunization programs. This regulatory lag further complicates the alignment of recommendations with global health standards.
Ultimately, vaccine availability is a dynamic and multifaceted issue that dictates the feasibility of recommendations. Countries must balance public health priorities with the realities of access, affordability, and approval processes. As global efforts continue to expand vaccine equity, the hope is that more countries will be able to recommend and provide a comprehensive range of vaccines, tailored to their populations’ needs. Until then, the number and type of vaccines recommended will remain a reflection of each country’s unique challenges and resources in securing these life-saving tools.
Public Reaction to the Polio Vaccine: Hope, Hesitation, and Triumph
You may want to see also
Frequently asked questions
The Centers for Disease Control and Prevention (CDC) recommends approximately 16 vaccines for children and adolescents, covering diseases such as measles, mumps, rubella, polio, and COVID-19, depending on age and health status.
The UK’s National Health Service (NHS) recommends around 13 vaccines for children, including those for meningitis, rotavirus, and human papillomavirus (HPV), as part of their routine immunization schedule.
India’s Universal Immunization Programme (UIP) recommends about 12 vaccines for infants and children, covering diseases like tuberculosis, hepatitis B, and Japanese encephalitis, with additional vaccines for pregnant women.
Australia’s National Immunisation Program (NIP) recommends approximately 14 vaccines for children, including those for whooping cough, pneumococcal disease, and varicella (chickenpox), with updates based on public health needs.