The question of how many deaths worldwide are directly attributable to vaccines is a complex and highly debated topic. While vaccines are widely recognized as one of the most effective public health interventions, saving millions of lives annually, rare adverse events, including fatalities, can occur. However, these instances are extremely rare and typically involve individuals with specific underlying health conditions or severe allergic reactions. Global health organizations, such as the World Health Organization (WHO), emphasize that the benefits of vaccination far outweigh the risks, and comprehensive monitoring systems, like the Vaccine Adverse Event Reporting System (VAERS) in the U.S., are in place to track and investigate potential vaccine-related deaths. Accurate data on vaccine-related fatalities is challenging to compile due to varying reporting standards and the need to distinguish between correlation and causation, but consensus among medical experts is that such deaths are exceptionally uncommon compared to the lives saved by vaccination.
Explore related products






What You'll Learn
- Reported Vaccine-Related Deaths: Official data on fatalities directly linked to vaccines globally
- Adverse Event Tracking: Systems monitoring vaccine side effects, including rare fatal cases
- COVID-19 Vaccine Deaths: Specific mortality data associated with COVID-19 vaccinations worldwide
- Historical Vaccine Fatalities: Pre-pandemic vaccine-related death statistics and trends
- Misinformation vs. Facts: Debunking false claims about vaccine-induced deaths with evidence
![]()
Reported Vaccine-Related Deaths: Official data on fatalities directly linked to vaccines globally
Vaccine safety monitoring systems globally have identified a minuscule number of fatalities directly linked to vaccination. According to the World Health Organization (WHO) and national regulatory bodies like the U.S. Centers for Disease Control and Prevention (CDC) and the European Medicines Agency (EMA), such deaths are exceedingly rare. For instance, the CDC’s Vaccine Adverse Event Reporting System (VAERS) and the Vaccine Safety Datalink (VSD) have recorded fewer than 100 deaths annually in the U.S. that were temporally associated with vaccines, out of hundreds of millions of doses administered. These cases often involve severe allergic reactions (anaphylaxis) or rare conditions like thrombosis with thrombocytopenia syndrome (TTS) linked to specific vaccines, such as the Johnson & Johnson COVID-19 vaccine.
Analyzing the data reveals that the risk of vaccine-related fatalities is dwarfed by the risks of the diseases they prevent. For example, COVID-19 vaccines have saved millions of lives globally, with studies estimating over 20 million deaths averted in the first year of their rollout. In contrast, TTS associated with the adenovirus vector vaccines occurred at a rate of approximately 7 per 1 million doses among women aged 18–49. Similarly, anaphylaxis from mRNA vaccines occurs in about 2–5 cases per million doses. These figures underscore the extraordinary safety profile of vaccines when compared to the mortality rates of infectious diseases like measles, influenza, or COVID-19.
Practical steps for healthcare providers and individuals include recognizing early signs of severe adverse reactions, such as difficulty breathing, swelling, or rapid heartbeat within 30 minutes of vaccination, which may indicate anaphylaxis. Immediate administration of epinephrine is critical in such cases. For vaccines with known rare risks, such as TTS, regulatory bodies recommend specific age and gender restrictions. For instance, many countries limit the use of the Johnson & Johnson vaccine to individuals over 50 or those unable to access other vaccines. Staying informed through official channels like the WHO, CDC, or EMA ensures adherence to the latest safety guidelines.
Comparatively, vaccine-related deaths are far less common than fatalities from common medical interventions. For example, general anesthesia carries a mortality risk of approximately 1 in 200,000 cases, while the risk of dying from a penicillin allergy is about 1 in 100,000. This context highlights the exceptional safety of vaccines, which undergo rigorous testing and continuous monitoring. Public health campaigns should emphasize these statistics to counter misinformation and build trust in vaccination programs, ensuring that rare adverse events are not misrepresented as widespread risks.
In conclusion, official data on vaccine-related fatalities confirm their extreme rarity, with rates far below those of the diseases they prevent. Understanding these specifics—such as the 7 per 1 million TTS risk or the 2–5 per million anaphylaxis rate—empowers individuals and healthcare providers to make informed decisions. By focusing on evidence-based information and following safety protocols, societies can maximize the life-saving benefits of vaccines while minimizing their minimal risks.
Flying to Mexico: Are COVID-19 Vaccinations Required for Travel?
You may want to see also
Explore related products






![]()
Adverse Event Tracking: Systems monitoring vaccine side effects, including rare fatal cases
Vaccine safety is a cornerstone of public health, but no medical intervention is entirely risk-free. Adverse Event Tracking Systems (AETS) play a critical role in identifying, monitoring, and mitigating rare but serious side effects, including fatalities. These systems, such as the Vaccine Adverse Event Reporting System (VAERS) in the U.S. and the Yellow Card scheme in the U.K., rely on healthcare providers and the public to report adverse events post-vaccination. While these reports are essential, they are not definitive proof of causation, as they often lack detailed clinical data. For instance, a reported death following vaccination could be coincidental, especially in older populations where mortality rates are higher. Understanding this distinction is crucial for interpreting data accurately.
Analyzing AETS data requires a nuanced approach. Take the COVID-19 vaccines, which have been administered to billions worldwide. As of 2023, VAERS has received thousands of reports of deaths following vaccination, but studies consistently show that these vaccines are not a leading cause of death. For example, a 2022 CDC analysis found that the risk of severe COVID-19 outcomes, including death, was significantly higher in unvaccinated individuals. AETS data must be cross-referenced with population-level mortality rates and controlled studies to determine causality. This process ensures that rare but genuine vaccine-related fatalities, such as those linked to anaphylaxis (occurring in approximately 2-5 cases per million doses), are identified and addressed.
Implementing effective AETS involves more than just collecting reports. It requires proactive surveillance, such as the use of electronic health records to flag potential adverse events in real time. For instance, the Vaccine Safety Datalink (VSD) in the U.S. monitors healthcare data from over 12 million people, enabling rapid investigation of safety signals. Additionally, global collaboration through the WHO’s Global Advisory Committee on Vaccine Safety ensures that rare events detected in one country are promptly shared internationally. This interconnected approach was pivotal in identifying and managing the rare thrombosis with thrombocytopenia syndrome (TTS) linked to adenovirus vector COVID-19 vaccines, leading to updated dosage recommendations and age restrictions.
For individuals, understanding AETS empowers informed decision-making. If you experience severe symptoms post-vaccination, such as difficulty breathing, chest pain, or persistent dizziness, seek medical attention immediately. Mild side effects like fever or soreness typically resolve within 48 hours and do not require reporting unless they persist. Parents should monitor children for unusual behavior or persistent crying, as these could indicate a rare adverse reaction. Remember, the vast majority of vaccine side effects are minor, and the risk of fatal outcomes remains extremely low compared to the risks of the diseases vaccines prevent.
In conclusion, AETS are vital tools for maintaining vaccine safety, but their data must be interpreted carefully. By combining passive reporting with active surveillance and global collaboration, these systems ensure that rare fatal cases are identified and managed effectively. For the public, awareness of these mechanisms fosters trust in vaccination programs while encouraging vigilance in reporting potential adverse events. As vaccination campaigns continue to evolve, robust AETS will remain essential for balancing individual safety with public health goals.
Is Gardasil Still Available? Debunking Vaccine Discontinuation Myths
You may want to see also
Explore related products






![]()
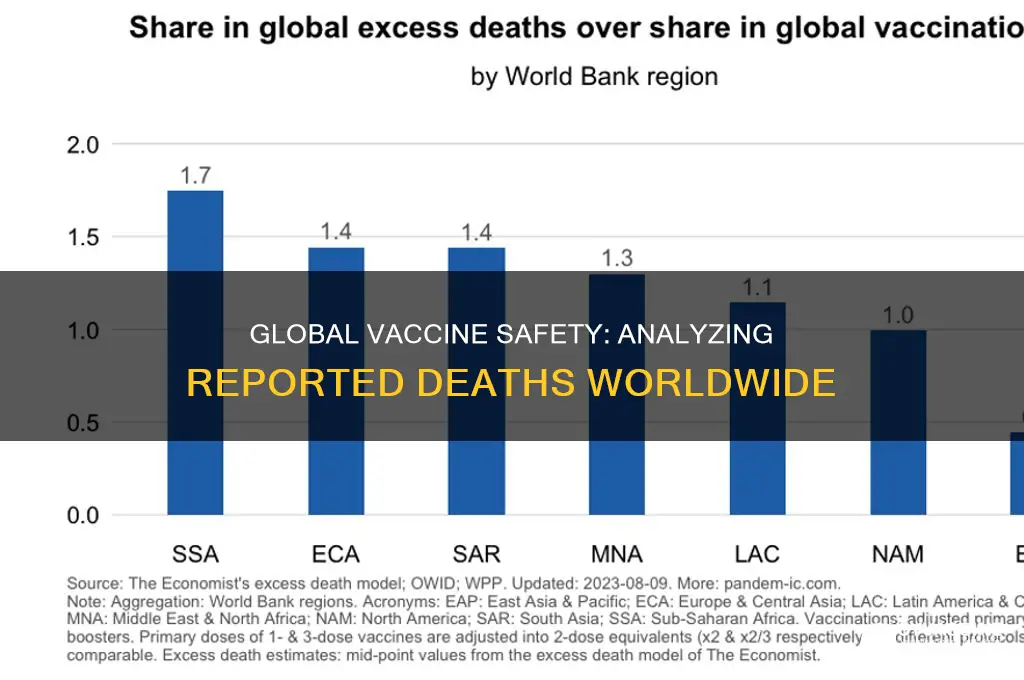
COVID-19 Vaccine Deaths: Specific mortality data associated with COVID-19 vaccinations worldwide
The global rollout of COVID-19 vaccines has been one of the most extensive public health interventions in history, with over 13 billion doses administered as of 2023. While vaccines have saved millions of lives, concerns about rare adverse events, including deaths, have persisted. Data from pharmacovigilance systems, such as the Vaccine Adverse Event Reporting System (VAERS) in the U.S. and the EudraVigilance in Europe, provide critical insights into these occurrences. However, interpreting these numbers requires understanding their limitations: reported cases are not always confirmed as vaccine-related, and underreporting is common. For instance, VAERS reported 15,000 deaths following COVID-19 vaccination by late 2022, but only a fraction were causally linked to the vaccine after investigation.
Analyzing specific mortality data reveals that severe outcomes are exceedingly rare. Studies show that anaphylaxis, a severe allergic reaction, occurs in approximately 2 to 5 cases per million doses, with fatalities even rarer. Another rare condition, vaccine-induced immune thrombotic thrombocytopenia (VITT), has been associated with adenovirus vector vaccines like AstraZeneca and Johnson & Johnson, with an incidence rate of 1 in 50,000 to 100,000 doses, primarily in younger adults. For context, the risk of death from COVID-19 itself is significantly higher, particularly in older age groups and those with comorbidities. A 2022 study in *The Lancet* estimated that COVID-19 vaccines prevented over 20 million deaths globally in their first year of use.
Age and dosage play a role in risk stratification. For example, many countries limited the use of adenovirus vector vaccines to older populations due to the higher risk of VITT in younger individuals. Additionally, the second dose of mRNA vaccines (Pfizer and Moderna) has been associated with a slightly higher risk of myocarditis, particularly in young males, though the condition is typically mild and treatable. Public health bodies recommend completing the primary series but advise careful consideration of boosters, balancing individual risk with community protection.
Practical tips for individuals include monitoring for severe symptoms post-vaccination, such as persistent chest pain, severe headache, or difficulty breathing, and seeking medical attention promptly. Healthcare providers should remain vigilant for rare adverse events and report them to national surveillance systems. Policymakers must communicate risks transparently, emphasizing the vast disparity between vaccine-related fatalities and COVID-19 mortality. For instance, the risk of dying from a vaccine is approximately 1 in a million, compared to 1 in 100 for unvaccinated COVID-19 cases in high-risk groups.
In conclusion, while no medical intervention is without risk, the mortality data associated with COVID-19 vaccines underscores their safety and efficacy. Rare fatalities, though tragic, are dwarfed by the lives saved through vaccination. Ongoing surveillance and transparent communication are essential to maintaining public trust and ensuring the continued success of vaccination campaigns.
Bray Wyatt's Vaccine Status: Unraveling the Truth Behind the Rumors
You may want to see also
Explore related products






![]()
Historical Vaccine Fatalities: Pre-pandemic vaccine-related death statistics and trends
Vaccine safety has been a cornerstone of public health for centuries, but historical data on vaccine-related fatalities provides critical context for understanding risks. Pre-pandemic records show that serious adverse events, including deaths, were exceedingly rare. For instance, the smallpox vaccine, one of the earliest and most impactful vaccines, had a fatality rate of approximately 1 to 2 per million doses administered. This minuscule risk pales in comparison to the millions of lives saved from smallpox-related deaths, which peaked at over 300 million in the 20th century alone. Such historical examples underscore the principle that the benefits of vaccination overwhelmingly outweigh the risks.
Analyzing trends from the 20th century reveals that vaccine safety has continually improved through rigorous testing and monitoring. The diphtheria, tetanus, and pertussis (DTaP) vaccine, introduced in the 1940s, initially had a higher adverse event profile, particularly in its early formulations. However, by the 1990s, advancements in vaccine technology reduced severe reactions to fewer than 1 in a million doses. Similarly, the oral polio vaccine (OPV) was linked to vaccine-derived poliovirus cases in approximately 1 out of every 2.7 million doses, prompting the development of the inactivated polio vaccine (IPV) as a safer alternative. These historical adjustments highlight the adaptive nature of vaccine safety protocols.
A comparative analysis of pre-pandemic vaccine fatalities across age groups reveals that risks were often higher in specific demographics. For example, the influenza vaccine, while generally safe, had slightly elevated risks for the elderly due to age-related immune responses. However, even in this vulnerable population, fatalities were estimated at less than 1 in 10 million doses. In contrast, childhood vaccines, such as the measles, mumps, and rubella (MMR) vaccine, demonstrated exceptional safety profiles, with fatal reactions occurring in fewer than 1 in a million cases. These disparities emphasize the importance of tailoring vaccine administration to individual risk factors.
Practical takeaways from historical data include the necessity of post-vaccination monitoring and transparent reporting systems. Countries with robust surveillance programs, such as the United States’ Vaccine Adverse Event Reporting System (VAERS), have been instrumental in identifying and mitigating rare risks. For instance, the 1976 swine flu vaccination campaign, which saw an increased risk of Guillain-Barré syndrome (approximately 1 in 100,000 doses), led to improved safety protocols and public communication strategies. Such lessons remain vital for maintaining trust in vaccination programs today.
In conclusion, historical vaccine fatalities were rare and often addressed through technological advancements and targeted safety measures. Understanding these trends provides a foundation for evaluating current vaccine safety concerns. By learning from past challenges, public health systems can continue to minimize risks while maximizing the life-saving potential of vaccines. This historical perspective is essential for informed decision-making and combating misinformation in the modern era.
When to Vaccinate Your Kitten Against Rabies: Age Guidelines
You may want to see also
Explore related products






![]()
Misinformation vs. Facts: Debunking false claims about vaccine-induced deaths with evidence
Misinformation about vaccine-induced deaths often relies on anecdotal evidence or misinterpreted data, creating a distorted narrative that undermines public trust in life-saving immunizations. For instance, claims that COVID-19 vaccines have caused millions of fatalities worldwide are frequently cited without credible sources. In reality, global health organizations like the World Health Organization (WHO) and the Centers for Disease Control and Prevention (CDC) rigorously monitor vaccine safety through systems such as the Vaccine Adverse Event Reporting System (VAERS) and the Global Advisory Committee on Vaccine Safety (GACVS). These systems have consistently shown that serious adverse events, including deaths, are exceedingly rare. For example, out of over 13 billion COVID-19 vaccine doses administered globally as of 2023, the number of confirmed deaths directly attributed to vaccines is in the low hundreds, primarily linked to rare conditions like thrombosis with thrombocytopenia syndrome (TTS) associated with adenovirus vector vaccines.
To debunk false claims effectively, it’s essential to understand how misinformation spreads and why it gains traction. Misinformation often exploits emotional triggers—fear, uncertainty, and distrust—to bypass critical thinking. For example, a viral social media post might claim “thousands of vaccine deaths are being covered up,” but fail to provide verifiable evidence or distinguish correlation from causation. To counter this, fact-checkers and health professionals must emphasize the scientific method: adverse events are investigated through controlled studies, autopsy reports, and peer-reviewed research. A practical tip for individuals is to verify claims against trusted sources like PubMed, WHO, or CDC, and to question the credibility of the information’s origin. For instance, a study published in *The Lancet* found no significant increase in all-cause mortality among vaccinated populations compared to unvaccinated groups, further disproving widespread death claims.
Comparing the risks of vaccination to the risks of the diseases they prevent provides crucial context. For example, COVID-19 has caused over 6 million confirmed deaths globally, with many more when accounting for excess mortality. In contrast, the risk of severe harm from vaccines is minuscule. The Pfizer-BioNTech and Moderna mRNA vaccines, administered in billions of doses, have a TTS risk of approximately 7 cases per million doses in individuals aged 30–49, with even lower rates in other age groups. Similarly, the flu vaccine, given annually to millions, has a fatality rate of less than 1 in a million. By framing vaccine risks against the mortality rates of preventable diseases—such as measles, which has a 1–3% fatality rate in unvaccinated populations—it becomes clear that the benefits of vaccination overwhelmingly outweigh the risks.
Finally, addressing misinformation requires a proactive approach to education and transparency. Health authorities must communicate vaccine safety data clearly and consistently, acknowledging rare adverse events while emphasizing their rarity. For example, the CDC’s Vaccine Safety Datalink (VSD) continuously monitors vaccinated populations, ensuring that any potential safety signals are promptly investigated. Individuals can contribute by sharing evidence-based information and avoiding the amplification of unverified claims. A practical step is to encourage friends and family to consult healthcare providers for personalized advice, especially for those with specific concerns, such as pre-existing conditions or allergies. By combining scientific evidence with clear communication, society can combat misinformation and protect public health.
Vaccinated Cat Bite: Immediate Steps and Precautions to Take
You may want to see also
Frequently asked questions
The exact number of vaccine-related deaths globally is not definitively known, as reporting systems vary by country. However, vaccine-related deaths are extremely rare. For example, the COVID-19 vaccines have been administered billions of times, with reported deaths linked to vaccines (such as from rare side effects like thrombosis with thrombocytopenia syndrome or TTS) numbering in the thousands, which is a tiny fraction of the total doses administered.
No, vaccine deaths are far less common than deaths caused by the diseases vaccines prevent. For instance, diseases like measles, polio, and COVID-19 have caused millions of deaths globally, while vaccine-related fatalities are exceedingly rare. Vaccines are rigorously tested for safety and monitored continuously to ensure their benefits far outweigh the risks.
Vaccine-related deaths are tracked through national and international surveillance systems, such as the Vaccine Adverse Event Reporting System (VAERS) in the U.S. and the World Health Organization’s (WHO) global monitoring programs. These systems rely on healthcare providers and individuals to report adverse events, which are then investigated to determine if they are directly linked to vaccination. However, underreporting and challenges in causality assessment can affect the accuracy of these numbers.