The Vaccine Adverse Event Reporting System (VAERS) is a national early warning system in the United States that collects and analyzes reports of adverse events following vaccination. It serves as a critical tool for monitoring vaccine safety, allowing healthcare professionals, vaccine manufacturers, and the public to report any potential side effects or health issues that occur after receiving a vaccine. Understanding how many adverse events are reported to VAERS is essential for assessing the system's effectiveness, identifying potential safety signals, and ensuring public trust in vaccination programs. While VAERS data provide valuable insights, it is important to note that reports do not necessarily indicate causation, as they are often unverified and may include coincidental events. Analyzing the volume and nature of these reports helps public health officials distinguish between rare but significant risks and common, mild reactions, ultimately contributing to the ongoing improvement of vaccine safety.
Explore related products






What You'll Learn
- VAERS Reporting Trends: Annual adverse event reports and their fluctuations over time
- Commonly Reported Symptoms: Most frequent vaccine side effects documented in VAERS
- Serious vs. Non-Serious Events: Classification and comparison of reported adverse events
- Vaccine-Specific Data: Adverse event rates for different vaccines (e.g., COVID-19, flu)
- VAERS Limitations: Challenges in interpreting data due to passive reporting system
![]()
VAERS Reporting Trends: Annual adverse event reports and their fluctuations over time
The Vaccine Adverse Event Reporting System (VAERS) is a critical tool for monitoring vaccine safety in the United States, allowing healthcare professionals and the public to report adverse events following vaccination. Understanding the trends in VAERS reporting is essential for interpreting the data accurately and identifying potential safety signals. Annual adverse event reports to VAERS have shown significant fluctuations over time, influenced by various factors such as vaccination campaigns, public awareness, and specific vaccine introductions. For instance, the COVID-19 pandemic led to an unprecedented surge in VAERS reports due to the rapid rollout of COVID-19 vaccines and heightened public scrutiny of vaccine safety.
Historically, VAERS has received a relatively stable number of reports annually, typically ranging from 30,000 to 50,000 reports per year prior to 2020. These reports cover a wide range of vaccines, including influenza, MMR, and HPV vaccines. However, the introduction of COVID-19 vaccines in late 2020 caused a dramatic increase in reporting. In 2021 alone, VAERS received over 1 million reports, a more than 20-fold increase compared to pre-pandemic years. This spike reflects both the massive scale of COVID-19 vaccination efforts and increased public and provider awareness of the reporting system. It is important to note that the volume of reports does not necessarily indicate a higher risk of adverse events, as VAERS is a passive surveillance system that includes unverified and coincidental events.
Fluctuations in VAERS reporting are also influenced by specific events or vaccine safety concerns. For example, the 2009 H1N1 influenza vaccine campaign led to a temporary increase in reports, as did concerns about the rotavirus vaccine in the late 1990s. These trends highlight the system's responsiveness to public health initiatives and emerging issues. Additionally, media coverage and public discourse can amplify reporting during periods of heightened vaccine scrutiny, as seen during the COVID-19 pandemic. Analyzing these patterns requires careful consideration of the context in which reports are filed.
Another key aspect of VAERS reporting trends is the proportionality of reports to vaccine doses administered. While the absolute number of reports may rise with increased vaccination rates, the proportion of adverse events per dose can provide a more meaningful metric for safety monitoring. For example, despite the surge in COVID-19 vaccine reports, the proportion of serious adverse events remained relatively low compared to the hundreds of millions of doses administered. This underscores the importance of interpreting VAERS data in conjunction with other surveillance systems and epidemiological studies.
In conclusion, VAERS reporting trends demonstrate dynamic fluctuations influenced by vaccination campaigns, public awareness, and specific vaccine introductions. The system's passive nature and susceptibility to external factors necessitate cautious interpretation of the data. By examining annual reports and their context, public health officials can better identify genuine safety signals and communicate vaccine risks effectively. Continued monitoring and transparency in reporting remain vital for maintaining public trust in vaccination programs.
Interstate Travel: Vaccination Requirements for Flying
You may want to see also
Explore related products






![]()
Commonly Reported Symptoms: Most frequent vaccine side effects documented in VAERS
The Vaccine Adverse Event Reporting System (VAERS) is a national early warning system in the United States that collects and analyzes reports of adverse events following vaccination. It is important to note that VAERS reports are voluntary and may include incomplete, inaccurate, or unverified information. However, the system provides valuable insights into potential patterns or trends in adverse events. When examining the data, certain symptoms and side effects are frequently reported, offering a glimpse into the most common experiences documented by individuals after receiving vaccines.
Among the most commonly reported symptoms in VAERS are localized reactions at the injection site. These include pain, swelling, and redness, which are typically mild to moderate in severity and resolve within a few days. Such reactions are a normal part of the body's immune response to vaccination and are not usually a cause for concern. For instance, the COVID-19 vaccines, as well as many others, often list these local reactions as expected side effects, indicating their frequent occurrence and benign nature.
Systemic reactions are also frequently documented in VAERS reports. These can include fatigue, headache, muscle pain, and fever. Such symptoms are generally mild to moderate and short-lived, often lasting a day or two after vaccination. For example, many individuals who received the COVID-19 vaccine reported experiencing fatigue and headache, which are now recognized as common side effects associated with this particular vaccine. These systemic reactions are a sign that the body is mounting an immune response, which is the intended purpose of vaccination.
In some cases, more specific adverse events are reported, such as allergic reactions, which can range from mild, like rash and itching, to severe, including anaphylaxis. Although rare, these reactions are closely monitored and studied through VAERS data. Another commonly reported symptom is lymphadenopathy, or swollen lymph nodes, particularly after COVID-19 vaccination. This side effect is typically temporary and resolves without intervention. It is important to emphasize that while these symptoms are frequently reported, they do not necessarily indicate a safety issue with the vaccine, but rather provide a comprehensive view of the post-vaccination experiences of a diverse population.
The analysis of VAERS data allows healthcare professionals and researchers to identify patterns and potential safety signals. By understanding the most commonly reported symptoms, medical experts can better educate and reassure the public about what to expect after vaccination. It is crucial to encourage reporting to VAERS to ensure a comprehensive dataset, enabling continuous monitoring and improvement of vaccine safety profiles. This system plays a vital role in maintaining public trust and confidence in vaccination programs by providing transparency and facilitating prompt investigation of any potential concerns.
Michigan Parents: Are Vaccines Mandatory for Kids?
You may want to see also
Explore related products






![]()
Serious vs. Non-Serious Events: Classification and comparison of reported adverse events
The Vaccine Adverse Event Reporting System (VAERS) is a critical tool for monitoring the safety of vaccines in the United States. It allows healthcare professionals, vaccine manufacturers, and the public to report any adverse events following vaccination. These reports are essential for identifying potential safety signals, but it is crucial to understand the distinction between serious and non-serious events to interpret the data accurately. VAERS receives a significant number of reports annually, ranging from mild reactions like soreness at the injection site to more severe outcomes such as hospitalization or death. Classifying these events as serious or non-serious helps prioritize investigations and ensures appropriate public health responses.
Classification of Adverse Events: Serious adverse events are defined by the FDA as those that result in death, a life-threatening condition, hospitalization, disability, congenital anomaly, or require medical intervention to prevent permanent impairment. These events are of particular concern and often trigger further investigation by health authorities. Non-serious adverse events, on the other hand, include symptoms like mild fever, headache, fatigue, or localized pain at the injection site. While these events are less critical, they are still important for understanding the overall safety profile of vaccines and can provide insights into common reactions that do not require medical attention.
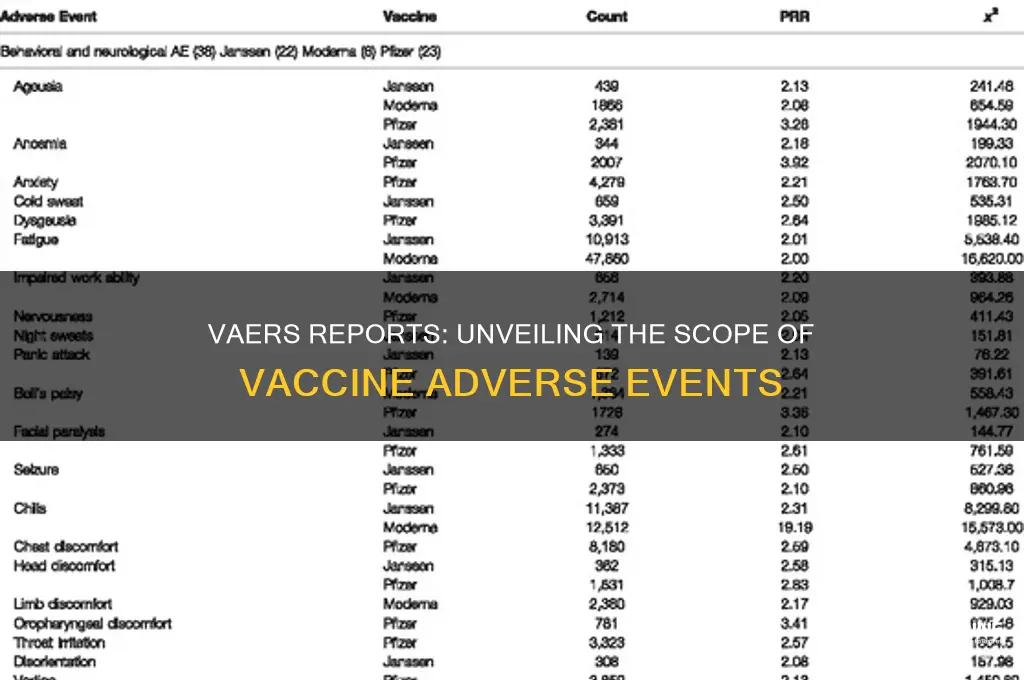
Comparison of Reported Events: A review of VAERS data reveals that non-serious adverse events far outnumber serious ones. For example, in the context of COVID-19 vaccines, millions of reports have been submitted, with the majority describing non-serious reactions such as pain at the injection site or mild flu-like symptoms. Serious events, though rare, are meticulously documented and analyzed. These include severe allergic reactions (anaphylaxis), thrombosis with thrombocytopenia syndrome (TTS), and myocarditis, particularly in younger populations. The disparity in numbers highlights the importance of distinguishing between the two categories to avoid misinterpretation of vaccine safety data.
Implications for Public Health: The classification of adverse events into serious and non-serious categories serves multiple purposes. Firstly, it helps regulatory agencies focus resources on investigating events that pose significant health risks. Secondly, it provides transparency to the public, ensuring that minor, expected reactions do not cause undue alarm. For instance, knowing that soreness and fatigue are common non-serious events can reassure individuals that their symptoms are normal. Conversely, identifying serious events promptly allows for swift action, such as updating vaccine guidelines or issuing warnings for specific populations.
Challenges and Considerations: While the classification system is valuable, it is not without challenges. VAERS is a passive reporting system, meaning it relies on voluntary submissions, which can lead to underreporting or incomplete data. Additionally, the system does not establish causality; a reported event does not necessarily mean the vaccine caused it. This limitation underscores the need for additional studies, such as clinical trials and epidemiological analyses, to confirm associations between vaccines and serious adverse events. Despite these challenges, the distinction between serious and non-serious events remains a cornerstone of vaccine safety surveillance, enabling informed decision-making and public trust.
Pneumonia Vaccines: Effective Defense Against Aspiration Pneumonia?
You may want to see also
Explore related products






![]()
Vaccine-Specific Data: Adverse event rates for different vaccines (e.g., COVID-19, flu)
The Vaccine Adverse Event Reporting System (VAERS) is a national early warning system in the United States that collects and analyzes reports of adverse events following vaccination. It is important to note that VAERS reports are voluntary and may not represent all adverse events that occur after vaccination. However, the data provides valuable insights into the safety profiles of different vaccines, including COVID-19 and flu vaccines. When examining vaccine-specific data, it is crucial to consider the number of doses administered and the types of adverse events reported.
For COVID-19 vaccines, VAERS data shows that as of October 2023, over 1 billion doses have been administered in the United States. The reported adverse event rates vary depending on the specific vaccine and the demographic group. For instance, the Pfizer-BioNTech and Moderna mRNA vaccines have been associated with a higher rate of anaphylaxis, albeit still rare, with approximately 2 to 5 cases per million doses administered. In contrast, the Johnson & Johnson (Janssen) viral vector vaccine has been linked to a rare but serious blood clotting condition, with an estimated rate of 7 per 1 million doses among women aged 18-49. Local reactions, such as pain at the injection site, and systemic reactions, like fatigue and headache, are more commonly reported across all COVID-19 vaccines, typically occurring in 10-60% of recipients.
Flu vaccines, which have been administered seasonally for decades, also have well-documented adverse event rates in VAERS. Each year, hundreds of millions of flu vaccine doses are given, and the majority of reported adverse events are mild, such as soreness at the injection site, headache, or fever. Serious adverse events are rare, with anaphylaxis occurring at a rate of approximately 1.3 cases per million doses. The live attenuated influenza vaccine (LAIV), administered as a nasal spray, has a slightly different safety profile, with a higher likelihood of mild respiratory symptoms in children but a lower risk of local reactions compared to injectable vaccines.
Comparing adverse event rates between COVID-19 and flu vaccines highlights both similarities and differences. Both types of vaccines have rare but serious adverse events, such as anaphylaxis, though the specific risks vary. COVID-19 vaccines, particularly the mRNA types, have been more frequently associated with myocarditis and pericarditis, especially in young males after the second dose, with rates ranging from 10 to 40 cases per million doses. In contrast, flu vaccines have a longer safety record and are generally associated with fewer reports of severe adverse events. However, the sheer volume of COVID-19 vaccine doses administered in a short period has led to more intensive monitoring and reporting, which may influence the perceived risk.
It is essential to interpret VAERS data with caution, as the system relies on passive reporting and does not establish causality between vaccines and adverse events. Signal detection and follow-up studies are often conducted to investigate potential safety concerns. For example, the initial reports of blood clots with the Janssen vaccine led to a temporary pause in its use, followed by updated guidance and warnings. Similarly, the association between mRNA COVID-19 vaccines and myocarditis prompted age-specific recommendations and ongoing surveillance. Understanding vaccine-specific adverse event rates helps healthcare providers and regulatory agencies balance the benefits of vaccination against potential risks, ensuring public trust and informed decision-making.
In conclusion, vaccine-specific adverse event data from VAERS provides critical information for assessing the safety of different vaccines, including COVID-19 and flu vaccines. While both types of vaccines have rare serious adverse events, their safety profiles differ based on the vaccine technology, population demographics, and the scale of administration. Continuous monitoring, transparent reporting, and context-appropriate interpretation of VAERS data are essential for maintaining vaccine safety and public confidence in immunization programs.
Natural Immunity vs. Vaccine: CDC's Take
You may want to see also
Explore related products


$14.99 $16.99




![]()
VAERS Limitations: Challenges in interpreting data due to passive reporting system
The Vaccine Adverse Event Reporting System (VAERS) is a critical tool for monitoring vaccine safety, but its passive reporting nature introduces significant limitations that complicate data interpretation. Unlike active surveillance systems, VAERS relies on voluntary submissions from healthcare providers, patients, and manufacturers. This means that not all adverse events are reported, leading to underreporting. The extent of underreporting is difficult to quantify, making it challenging to determine the true incidence of vaccine-related adverse events. For example, minor side effects like soreness at the injection site may go unreported, while more severe events are more likely to be documented. This variability skews the data, making it hard to draw accurate conclusions about the frequency and severity of adverse events.
Another challenge with VAERS is the lack of denominator data, which refers to the total number of vaccine doses administered. Without this information, it is impossible to calculate rates of adverse events per vaccine dose. This limitation prevents researchers from assessing the risk of specific adverse events relative to the vaccinated population. For instance, knowing that 100 cases of an adverse event were reported is less informative than knowing that these cases occurred out of 1 million doses administered. The absence of denominator data limits the system's ability to provide context and meaningful risk assessments.
The passive nature of VAERS also means that the data collected are often incomplete or inconsistent. Reports may lack critical details such as the patient’s medical history, concurrent medications, or the timing of symptom onset relative to vaccination. This incompleteness can make it difficult to establish a causal relationship between the vaccine and the reported event. Additionally, the system does not verify the accuracy of reports before they are included in the database, which can lead to the inclusion of erroneous or misleading information. Such inconsistencies further complicate efforts to analyze and interpret the data reliably.
Furthermore, VAERS is subject to reporting biases that can distort the data. Healthcare providers and the public may be more likely to report adverse events following vaccines that have received significant media attention or public scrutiny, even if the events are unrelated. This phenomenon, known as "stimulated reporting," can create the appearance of increased risk for certain vaccines. Conversely, underreporting may occur if healthcare providers are unaware of the reporting process or perceive it as burdensome. These biases can lead to misinterpretations of vaccine safety signals and undermine public trust in vaccination programs.
Lastly, VAERS data alone are insufficient for establishing causality between vaccines and adverse events. The system is designed to detect signals—unusual or unexpected patterns—that may warrant further investigation. However, the presence of a report in VAERS does not prove that a vaccine caused the adverse event. Confounding factors, such as underlying medical conditions or coincidental illnesses, can complicate the interpretation of individual reports. Rigorous epidemiological studies, such as clinical trials or post-authorization safety studies, are necessary to confirm or refute causal relationships. Thus, while VAERS is a valuable early warning system, its passive reporting structure necessitates cautious and nuanced interpretation of its data.
Vaccination Requirements for Driving into the USA
You may want to see also
Frequently asked questions
The number of reports submitted to VAERS varies each year, but on average, it receives around 30,000 to 50,000 reports annually.
No, VAERS is a passive reporting system, meaning it collects reports of adverse events after vaccination but does not determine causation. Not all reported events are confirmed to be caused by vaccines.
Approximately 10-15% of VAERS reports are classified as serious, which includes events such as hospitalizations, life-threatening conditions, or deaths.
The number of VAERS reports is very small compared to the total number of vaccines administered. For example, in the U.S., hundreds of millions of vaccines are given annually, with only a tiny fraction resulting in reports to VAERS.