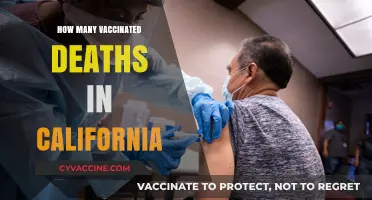
The topic of vaccine-related deaths in the United States is a subject of significant public interest and scrutiny, particularly in the context of widespread immunization campaigns, such as those for COVID-19. While vaccines are rigorously tested and monitored for safety, rare adverse events, including fatalities, can occur. According to the Centers for Disease Control and Prevention (CDC) and the Vaccine Adverse Event Reporting System (VAERS), the number of reported deaths potentially linked to vaccines is extremely low compared to the millions of doses administered annually. For instance, as of recent data, COVID-19 vaccine-related deaths are estimated at a rate of less than 0.002% of administered doses. It is crucial to note that not all reported deaths are directly caused by vaccines, as underlying health conditions or coincidental events may play a role. Public health officials emphasize that the benefits of vaccination in preventing severe disease and death far outweigh the risks, making vaccines a cornerstone of disease prevention and control.
| Characteristics | Values |
|---|---|
| Total Reported Deaths (VAERS) | 22,623 (as of October 2023) |
| Deaths per Million Doses Administered | Approximately 2-4 (varies by vaccine type and population) |
| COVID-19 Vaccine-Related Deaths | ~15,000 reported to VAERS (majority unverified as vaccine-caused) |
| Verified Vaccine-Related Deaths | Extremely rare (e.g., anaphylaxis: ~2-5 per million doses) |
| Leading Cause of Vaccine-Related Deaths | COVID-19 vaccines (due to higher administration numbers) |
| Comparison to Other Causes | Significantly lower than deaths from COVID-19 infection or other risks |
| Data Source | CDC, VAERS (Vaccine Adverse Event Reporting System) |
| Note | VAERS data is passive and includes unverified reports |
Disclaimer: The data reflects reported numbers and does not confirm causality. Most reported deaths are coincidental or unrelated to vaccination. Always consult official health sources for accurate information.
Explore related products






What You'll Learn
- COVID-19 vaccine fatalities reported to VAERS (Vaccine Adverse Event Reporting System)
- Historical vaccine-related deaths in the United States since 1900
- Flu vaccine mortality rates compared to other vaccines
- Analysis of rare anaphylaxis deaths post-vaccination in the U.S
- Vaccine safety monitoring systems and death investigation protocols in the U.S
![]()
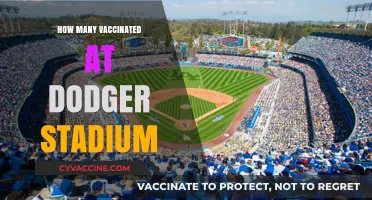
COVID-19 vaccine fatalities reported to VAERS (Vaccine Adverse Event Reporting System)
The Vaccine Adverse Event Reporting System (VAERS) has been a focal point in discussions about COVID-19 vaccine safety, particularly regarding fatalities. VAERS is a passive reporting system co-managed by the CDC and FDA, where healthcare professionals, vaccine manufacturers, and individuals can submit reports of adverse events following vaccination. As of recent data, VAERS has received thousands of reports of deaths following COVID-19 vaccination, but interpreting these numbers requires careful analysis. For instance, a report to VAERS does not automatically mean the vaccine caused the death; it only indicates a temporal association. This distinction is critical for understanding the system’s limitations and strengths.
Analyzing VAERS data reveals trends that help contextualize these reports. For example, the majority of reported deaths involve individuals aged 65 and older, a demographic already at higher risk of severe illness and death from COVID-19. Additionally, many reports lack detailed medical histories or autopsies, making it challenging to establish causality. Studies comparing VAERS data with background mortality rates show that the number of reported deaths is not significantly higher than expected in a vaccinated population of this size. This suggests that while rare fatalities may occur, they are not necessarily linked to the vaccine itself.
To navigate VAERS data effectively, it’s essential to cross-reference it with other surveillance systems, such as the CDC’s Vaccine Safety Datalink (VSD). The VSD uses active monitoring from healthcare organizations to identify potential safety signals. When VAERS reports align with findings from the VSD or other studies, they carry more weight. For example, the rare association between the Johnson & Johnson vaccine and thrombosis with thrombocytopenia syndrome (TTS) was first flagged in VAERS and later confirmed through additional research, leading to updated guidelines for vaccine administration.
Practical tips for interpreting VAERS data include focusing on patterns rather than individual reports and considering the vaccinated population’s size. As of 2023, over 650 million COVID-19 vaccine doses have been administered in the U.S., making extremely rare events more likely to appear in the dataset. Healthcare providers should also educate patients about VAERS’s role as an early warning system, not a definitive source of causation. Encouraging reporting of any adverse events, no matter how minor, strengthens the system’s ability to detect genuine safety concerns.
In conclusion, while VAERS reports of COVID-19 vaccine-related fatalities can be alarming, they must be interpreted within the context of the system’s design and limitations. By combining VAERS data with active surveillance and epidemiological studies, public health officials can better assess vaccine safety and communicate risks effectively. For individuals, understanding how VAERS works fosters informed decision-making and trust in the vaccination process.
China's COVID-19 Vaccine: Breakthrough or Bust?
You may want to see also
Explore related products






![]()
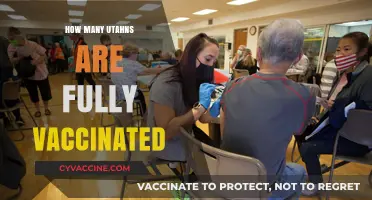
Historical vaccine-related deaths in the United States since 1900
Vaccine-related deaths in the United States since 1900 are exceedingly rare, with historical data showing that fatalities directly attributable to vaccines are statistically insignificant compared to the millions of lives saved. For instance, the smallpox vaccine, widely administered in the early 20th century, had a fatality rate of approximately 1 to 2 per million doses, yet it eradicated a disease that once killed 30% of its victims. This stark contrast underscores the overwhelming benefits of vaccination despite minimal risks.
One notable example of vaccine-related fatalities occurred during the 1955 Cutter incident, where improperly inactivated polio vaccine doses caused 40,000 cases of abortive polio, 56 cases of paralytic polio, and 5 deaths. This event led to stricter manufacturing regulations, illustrating how historical tragedies have driven improvements in vaccine safety. Such incidents, however, remain isolated and do not reflect the safety profile of modern vaccines, which undergo rigorous testing and monitoring.
Comparatively, the 1976 swine flu vaccination campaign provides another historical case study. Approximately 45 million Americans received the vaccine, and 25 deaths were attributed to Guillain-Barré syndrome (GBS), a rare neurological condition. While this raised public concern, the risk of GBS from the vaccine was approximately 1 in 100,000 doses, far lower than the risks associated with the flu itself. This example highlights the importance of weighing vaccine risks against the dangers of preventable diseases.
Analyzing trends, the introduction of the Vaccine Adverse Event Reporting System (VAERS) in 1990 has allowed for systematic tracking of potential vaccine-related deaths. However, VAERS data must be interpreted cautiously, as it relies on voluntary reporting and does not establish causation. For instance, between 2006 and 2016, VAERS received 2,154 reports of death following vaccination, but investigations found no consistent patterns suggesting vaccines were the cause. This emphasizes the need for robust epidemiological studies to distinguish correlation from causation.
In conclusion, historical vaccine-related deaths in the U.S. are rare and often tied to specific incidents that have since informed safety protocols. Modern vaccines, such as those for COVID-19, undergo extensive clinical trials and post-market surveillance, further minimizing risks. Practical tips for individuals include staying informed about vaccine safety data, consulting healthcare providers, and reporting any adverse events to VAERS. The historical record demonstrates that vaccines remain one of the safest and most effective public health interventions.
Does the J&J Vaccine Hurt? Pain, Side Effects, and Recovery Explained
You may want to see also
Explore related products

$29.95 $25.48


$20.41 $29.99



![]()
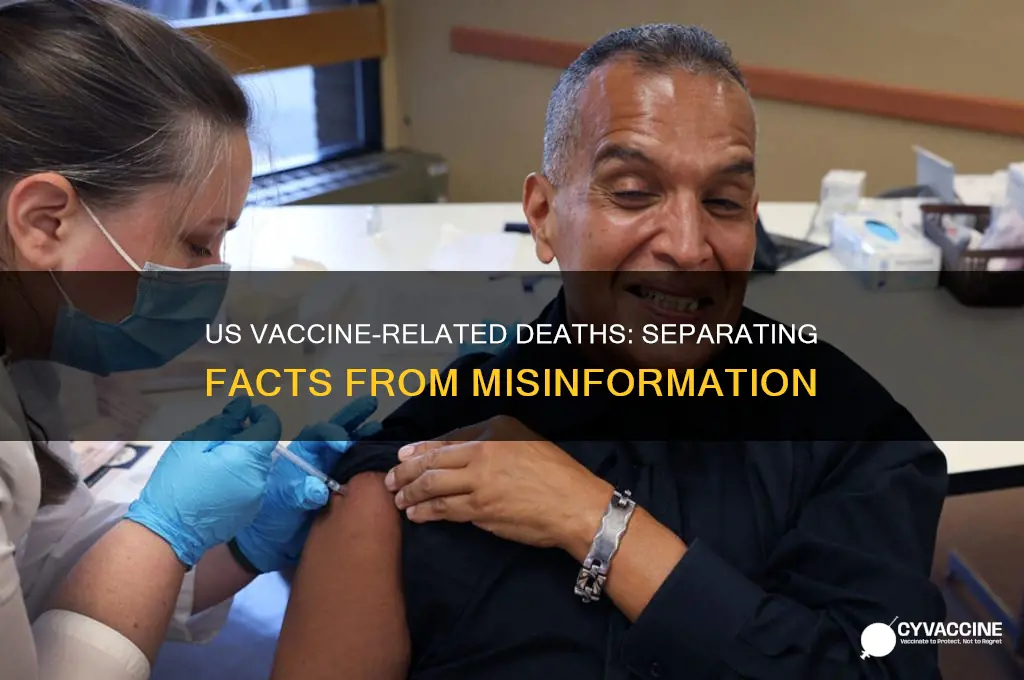
Flu vaccine mortality rates compared to other vaccines
The flu vaccine, a seasonal staple in public health, carries a mortality rate so minuscule it’s often measured in fractions per million doses. According to the CDC’s Vaccine Adverse Event Reporting System (VAERS), severe reactions resulting in death are exceedingly rare, with estimates suggesting fewer than 1 in a million recipients experience fatal outcomes. This contrasts sharply with the flu itself, which claims tens of thousands of lives annually in the U.S., particularly among the elderly and immunocompromised. For context, the 2019-2020 flu season saw approximately 22,000 deaths, while the vaccine’s safety profile remains one of the most robust in modern medicine.
Consider the flu vaccine’s mortality rate in comparison to other vaccines. The MMR (measles, mumps, rubella) vaccine, for instance, has a fatality rate of roughly 1 in 3 million doses, primarily linked to severe allergic reactions. Similarly, the COVID-19 vaccines, administered in billions of doses globally, have shown death rates of approximately 2-4 per million, often associated with rare conditions like thrombosis with thrombocytopenia syndrome (TTS). The flu vaccine’s safety record is thus not just impressive in isolation but stands out even when benchmarked against other highly vetted vaccines.
Practical tips for minimizing risks further underscore the flu vaccine’s safety. Individuals with severe egg allergies, a historical concern due to egg-based manufacturing, can now safely receive most flu vaccines, including egg-free formulations like Flublok. Additionally, the CDC recommends monitoring for severe allergic reactions (anaphylaxis) post-vaccination, though such events occur in fewer than 2 cases per million doses. For those over 65, high-dose or adjuvanted flu vaccines are available, offering enhanced protection without compromising safety.
A comparative analysis reveals that the flu vaccine’s mortality rate is not just low but also reflective of its targeted design. Unlike vaccines for diseases like smallpox (historical fatality rates of 1-2 per million) or yellow fever (3-4 per million in rare cases), the flu vaccine is annually updated to match circulating strains, minimizing mismatch risks. This adaptability, combined with decades of safety data, positions it as one of the safest medical interventions available.
In conclusion, the flu vaccine’s mortality rate is a testament to its rigorous development and monitoring. When weighed against the mortality burden of influenza itself or the safety profiles of other vaccines, it emerges as a critical, low-risk tool in public health. For those hesitant due to safety concerns, the data is clear: the risks of forgoing vaccination far outweigh the vanishingly small risks of the vaccine itself.
Vaccines and Fetal Cells: Separating Fact from Fiction
You may want to see also
Explore related products






![]()
Analysis of rare anaphylaxis deaths post-vaccination in the U.S
Vaccine-related deaths are exceedingly rare, yet anaphylaxis—a severe, life-threatening allergic reaction—remains a critical concern post-vaccination. In the U.S., the Centers for Disease Control and Prevention (CDC) and the Vaccine Adverse Event Reporting System (VAERS) monitor such cases closely. Data from COVID-19 vaccine administration reveals that anaphylaxis occurs at a rate of approximately 2 to 5 cases per million doses. While the majority of these reactions are treatable with prompt medical intervention, a handful have tragically resulted in fatalities. Understanding these rare events is essential for public health transparency and improving safety protocols.
Anaphylaxis post-vaccination typically occurs within minutes to hours of receiving a dose, with symptoms including rapid onset of respiratory distress, swelling, and hypotension. The mechanism often involves an immune response to vaccine components, such as polyethylene glycol (PEG), found in mRNA vaccines like Pfizer-BioNTech and Moderna. Individuals with a history of severe allergies, particularly to PEG or polysorbate, are at higher risk. For instance, the CDC recommends that those with such histories be observed for 30 minutes post-vaccination, compared to the standard 15 minutes for the general population. This extended observation period has been instrumental in managing anaphylactic reactions effectively.
Analyzing the fatalities, it’s crucial to note that these cases are not uniform. Age, pre-existing conditions, and the timeliness of medical response play significant roles. For example, older adults, particularly those over 65, may have a higher risk due to age-related immune changes or comorbidities. However, the overall number of anaphylaxis-related deaths remains minuscule compared to the millions of doses administered. As of recent data, fewer than 20 such deaths have been reported in the U.S. out of over 600 million COVID-19 vaccine doses given—a rate of approximately 1 in 30 million doses.
To mitigate risks, healthcare providers must adhere to strict protocols. Pre-vaccination screening for allergy histories, ensuring immediate access to epinephrine (e.g., EpiPens), and training staff in anaphylaxis management are critical steps. Patients should also be educated on recognizing early symptoms, such as hives, dizziness, or throat tightness, and instructed to seek emergency care promptly. For high-risk individuals, alternative vaccines (e.g., Novavax, which does not contain PEG) may be considered, though availability and efficacy must be weighed.
In conclusion, while anaphylaxis deaths post-vaccination are tragic, they are exceptionally rare and manageable with proper precautions. The U.S. healthcare system’s vigilance in monitoring and responding to these events underscores the commitment to vaccine safety. By refining protocols and raising awareness, the risks can be further minimized, ensuring public trust in vaccination programs remains strong.
Step-by-Step Guide to Registering for Your COVID-19 Vaccination Appointment
You may want to see also
Explore related products






![]()
Vaccine safety monitoring systems and death investigation protocols in the U.S
The U.S. employs a multi-layered vaccine safety monitoring system to detect and investigate rare adverse events, including deaths. At its core is the Vaccine Adverse Event Reporting System (VAERS), a passive surveillance program co-managed by the CDC and FDA. Anyone—healthcare providers, patients, or manufacturers—can submit reports of suspected vaccine-related issues. While VAERS captures a broad range of events, its voluntary nature limits its ability to establish causality. For instance, a report of a death following vaccination does not automatically imply the vaccine was the cause; it merely signals a need for further investigation.
When a death is reported to VAERS, it triggers a series of steps under the Vaccine Safety Datalink (VSD) and the Clinical Immunization Safety Assessment (CISA) Project. The VSD, a network of healthcare organizations, conducts near real-time analyses of vaccination data from over 12 million people. If a signal emerges—such as an unexpected number of deaths in a specific age group, say adults over 65 receiving a high-dose flu vaccine—it is escalated for in-depth review. The CISA Project, comprising medical experts, evaluates complex cases, often involving detailed medical records and autopsy reports. For example, a 42-year-old with no pre-existing conditions who dies within 48 hours of receiving an mRNA COVID-19 vaccine would undergo rigorous scrutiny to rule out coincidental causes like undiagnosed cardiac conditions.
One critical tool in death investigations is the CDC’s Vaccine Safety Technical (VaST) workgroup, which convenes experts to assess data and recommend actions. During the COVID-19 vaccine rollout, VaST analyzed reports of rare thrombosis with thrombocytopenia syndrome (TTS) following the Johnson & Johnson vaccine. This led to a temporary pause in its use for individuals under 50, demonstrating how monitoring systems can prompt swift public health responses. Similarly, the CDC’s investigation into myocarditis cases in young males post-mRNA vaccination resulted in updated dosage recommendations—a single dose for high-risk adolescents instead of the standard two.
Despite these robust systems, challenges remain. Distinguishing between coincidental deaths and vaccine-related fatalities is complex. For example, in a country where approximately 7,700 people die daily from natural causes, temporal associations between vaccination and death are inevitable. To address this, investigators use statistical methods like proportional reporting ratios and background mortality rates. Public transparency is also crucial; the CDC publishes weekly reports on COVID-19 vaccine safety, including death investigations, to maintain trust. As of 2023, out of over 600 million COVID-19 vaccine doses administered in the U.S., the CDC confirmed fewer than 100 deaths plausibly linked to vaccines—a rate of approximately 0.000016%.
In practice, healthcare providers play a pivotal role in this system. They are instructed to report any death within 30 days of vaccination to VAERS, regardless of suspected causality. Patients and caregivers can also contribute by documenting symptoms and timelines. For instance, if a 70-year-old experiences severe chest pain 24 hours after a pneumonia vaccine, immediate reporting could expedite investigation. While no system is perfect, the U.S.’s layered approach ensures that even the rarest vaccine-related deaths are identified, analyzed, and acted upon, safeguarding public health without compromising vaccine confidence.
Essential Puppy Distemper Vaccination Schedule: How Many Shots Are Needed?
You may want to see also
Frequently asked questions
As of the latest data from the CDC and FDA, the number of deaths directly attributed to COVID-19 vaccines is extremely low. Reports of severe adverse events, including deaths, are rare and thoroughly investigated. The Vaccine Adverse Event Reporting System (VAERS) has received a small number of reports, but causality is not always established.
While rare cases of severe adverse events, such as anaphylaxis or thrombosis with thrombocytopenia syndrome (TTS), have been linked to COVID-19 vaccines, confirmed deaths directly caused by the vaccines are exceptionally rare. Most reported deaths in vaccinated individuals are unrelated to the vaccine.
The risk of death from COVID-19 far outweighs the risk of death from the vaccines. Millions of lives have been saved by vaccination, while vaccine-related deaths remain extremely rare, with rates significantly lower than COVID-19 mortality rates.
VAERS is a passive reporting system that collects data on adverse events following vaccination. While it helps identify potential safety signals, it does not prove causation. Reports of deaths in VAERS are investigated further to determine if they are vaccine-related.
Health authorities like the CDC and FDA continuously monitor vaccine safety through systems like VAERS, the Vaccine Safety Datalink, and clinical trials. Any reported deaths are thoroughly reviewed to assess causality and ensure ongoing vaccine safety.