The development and distribution of the COVID-19 vaccine have been a monumental global effort, involving multiple stages to ensure safety, efficacy, and accessibility. Understanding the stages of the coronavirus vaccine process is crucial for appreciating the complexity and rigor behind its creation. From initial research and pre-clinical trials to clinical trials, regulatory approval, manufacturing, and distribution, each phase plays a vital role in delivering a reliable vaccine to the public. This process not only highlights the scientific advancements but also underscores the collaborative efforts of researchers, governments, and healthcare organizations worldwide in combating the pandemic.
Explore related products


$11.67 $21.99

$50 $50



What You'll Learn
- Vaccine Development Phases: Pre-clinical, Phase I, II, III trials, and regulatory approval stages explained
- Dosing Schedule: Single-dose vs. multi-dose vaccines and their effectiveness timelines
- Booster Shots: Need, timing, and their role in prolonged immunity enhancement
- Vaccine Platforms: mRNA, viral vector, protein subunit, and inactivated virus technologies
- Global Distribution Stages: Manufacturing, allocation, and equitable access challenges worldwide
![]()
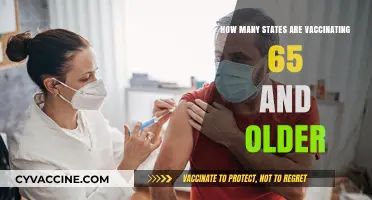
Vaccine Development Phases: Pre-clinical, Phase I, II, III trials, and regulatory approval stages explained
Vaccine development is a rigorous, multi-stage process designed to ensure safety, efficacy, and quality before a vaccine can be administered to the public. The journey from initial concept to widespread distribution involves several critical phases, each with specific objectives and regulatory oversight. For COVID-19 vaccines, this process has been accelerated due to the global health emergency, but without compromising the essential steps that guarantee safety and effectiveness. The key stages include pre-clinical testing, Phase I, II, and III clinical trials, and regulatory approval, followed by ongoing monitoring.
The first stage, pre-clinical testing, is conducted in laboratories and involves animal testing to assess the vaccine's safety and potential immune response. Researchers evaluate whether the vaccine produces antibodies and whether it causes any harmful effects. This stage is crucial for identifying potential risks before the vaccine is tested in humans. For COVID-19 vaccines, pre-clinical studies focused on understanding the virus's behavior and how the immune system responds to it. Once pre-clinical data demonstrates promise, the vaccine advances to human trials.
Phase I trials mark the beginning of human testing and typically involve a small group of healthy volunteers (20–100 participants). The primary goal is to assess the vaccine's safety, determine dosage levels, and identify potential side effects. Researchers closely monitor participants to ensure the vaccine does not cause serious harm. This phase also provides initial data on whether the vaccine elicits an immune response. For COVID-19 vaccines, Phase I trials were expedited but maintained strict safety protocols to ensure participant well-being.
Phase II trials expand the testing to a larger group (hundreds of participants), often including individuals who resemble the target population (e.g., older adults or those with underlying conditions). This phase further evaluates safety and begins to assess the vaccine's efficacy by measuring immune responses and monitoring for adverse effects. Researchers may also test different dosing regimens. In the case of COVID-19 vaccines, Phase II trials were crucial for understanding how the vaccine performed in diverse populations and refining its formulation.
Phase III trials are the largest and most critical, involving thousands to tens of thousands of participants across multiple locations. This phase rigorously tests the vaccine's efficacy by comparing a vaccinated group to a placebo group to determine how well it prevents disease. Safety monitoring continues on a larger scale. For COVID-19 vaccines, Phase III trials were conducted globally to ensure the vaccine's effectiveness across different populations and variants. Completion of this phase provides the data needed for regulatory approval.
The final stage before distribution is regulatory approval, where health authorities such as the FDA, EMA, or WHO review all data from pre-clinical and clinical trials to ensure the vaccine meets safety, efficacy, and manufacturing quality standards. For COVID-19 vaccines, emergency use authorizations (EUAs) were granted in many countries to expedite access during the pandemic, but full approvals followed after thorough reviews. Post-approval, vaccines undergo Phase IV monitoring (pharmacovigilance) to track long-term safety and effectiveness in the general population. This multi-stage process ensures that vaccines, including those for COVID-19, are both safe and effective for public use.
Vaccine Ingredients: Global Standardization or Customization?
You may want to see also
Explore related products






![]()
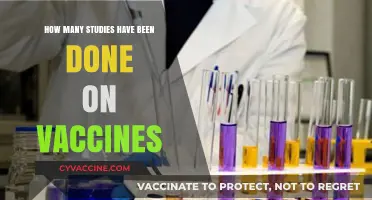
Dosing Schedule: Single-dose vs. multi-dose vaccines and their effectiveness timelines
The COVID-19 vaccination process involves multiple stages, from initial research and development to clinical trials and regulatory approval. Once a vaccine is authorized, the dosing schedule becomes a critical aspect of its deployment. COVID-19 vaccines are administered in either single-dose or multi-dose regimens, each with distinct effectiveness timelines. Understanding these differences is essential for individuals and healthcare providers to ensure optimal protection against the virus.
Single-dose vaccines, such as the Johnson & Johnson (Janssen) vaccine, offer a streamlined approach by providing full immunization after just one shot. This regimen is particularly advantageous for populations with limited access to healthcare or those who may face challenges in returning for a second dose. The effectiveness of single-dose vaccines typically begins to manifest within 2–4 weeks after vaccination. Studies have shown that the Johnson & Johnson vaccine provides approximately 66% efficacy against moderate to severe COVID-19 globally, with higher efficacy rates against severe disease and hospitalization. While the protection may be slightly lower compared to some multi-dose vaccines, the single-dose format ensures quicker population-wide coverage, which is crucial during outbreaks.
Multi-dose vaccines, including Pfizer-BioNTech and Moderna, require two or more doses to achieve maximum effectiveness. The Pfizer vaccine is administered in two doses, 3–4 weeks apart, while the Moderna vaccine is given in two doses, 4 weeks apart. These vaccines rely on mRNA technology, which stimulates a robust immune response after the second dose. Effectiveness begins to rise significantly about 1–2 weeks after the first dose, offering partial protection, but reaches its peak efficacy of around 94–95% after the second dose. This staggered dosing allows the immune system to build a stronger and more durable defense against the virus. Additionally, booster doses are often recommended for multi-dose vaccines to maintain long-term immunity, especially as new variants emerge.
The choice between single-dose and multi-dose vaccines often depends on logistical considerations, individual health needs, and public health goals. Single-dose vaccines are ideal for rapid immunization campaigns, while multi-dose vaccines provide higher initial efficacy and longer-lasting immunity. It’s important to note that the effectiveness timelines for both types of vaccines are influenced by factors such as age, underlying health conditions, and the prevalence of viral variants. Regardless of the regimen, adhering to the recommended dosing schedule is crucial for ensuring the best possible protection against COVID-19.
In summary, single-dose vaccines offer convenience and rapid immunity, making them suitable for broad population coverage, while multi-dose vaccines provide higher efficacy and sustained protection. Both play vital roles in the global effort to control the pandemic. Individuals should consult healthcare providers to determine the most appropriate vaccine and dosing schedule based on their specific circumstances. As research continues, ongoing monitoring of vaccine effectiveness and the need for additional doses will remain key components of the COVID-19 vaccination strategy.
Can You Safely Receive Multiple Vaccines Post-Stem Cell Transplant?
You may want to see also
Explore related products






![]()
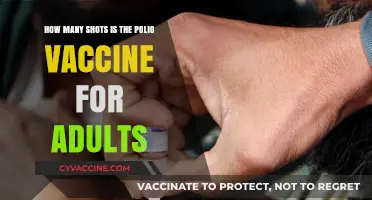
Booster Shots: Need, timing, and their role in prolonged immunity enhancement
The COVID-19 vaccination process typically involves multiple stages, with the initial series consisting of one or two doses, depending on the vaccine type. However, the concept of booster shots has become crucial in the fight against the coronavirus, especially as new variants emerge and immunity wanes over time. Booster shots are additional doses administered after the initial vaccine series to enhance and prolong immunity, ensuring continued protection against the virus. This strategy is not unique to COVID-19 vaccines; many other vaccines, such as those for tetanus and influenza, also require periodic boosters to maintain effectiveness.
The Need for Booster Shots:
The primary goal of booster shots is to reinforce the immune system's memory of the virus, thereby improving its ability to recognize and combat it. Over time, the immune response generated by the initial vaccine doses may decrease, leaving individuals more susceptible to infection. This is particularly concerning with the emergence of new SARS-CoV-2 variants, which can evade the immune protection provided by earlier vaccinations. Booster doses stimulate the production of antibodies and activate memory cells, ensuring a rapid and robust response if the virus is encountered. Studies have shown that booster shots significantly increase antibody levels, providing better protection against symptomatic infection, severe disease, and hospitalization.
Timing of Booster Administration:
Determining the optimal timing for booster shots is a critical aspect of vaccination strategies. Initially, boosters were recommended several months after the completion of the primary vaccine series. For instance, the Pfizer-BioNTech and Moderna mRNA vaccines' boosters were advised 6 months after the second dose, while the Johnson & Johnson (J&J) vaccine's booster was suggested 2 months after the initial shot. However, as the pandemic evolved, so did the booster guidelines. Health authorities now recommend additional boosters for specific populations, such as older adults and immunocompromised individuals, who are at higher risk of severe disease. The timing may vary based on factors like age, underlying health conditions, and the prevalence of new variants.
Prolonged Immunity and Public Health Impact:
Booster shots play a pivotal role in maintaining long-term immunity at both individual and population levels. By enhancing immune memory, boosters reduce the likelihood of breakthrough infections and severe outcomes, thereby decreasing the overall disease burden. This is especially important in preventing overwhelming healthcare systems and protecting vulnerable populations. Moreover, boosters contribute to reducing viral transmission, as individuals with higher antibody levels are less likely to spread the virus. As the pandemic transitions to an endemic phase, booster strategies will be essential in managing COVID-19 as a controllable respiratory disease, similar to the annual flu vaccination campaigns.
In the context of the COVID-19 vaccine stages, booster shots represent a critical phase in ensuring the long-term success of vaccination programs. They address the natural decline of immunity and adapt to the evolving nature of the virus. As research continues, public health officials can refine booster recommendations, considering factors like variant-specific boosters and personalized vaccination schedules. This dynamic approach to vaccination is key to staying ahead of the virus and minimizing its impact on global health. With ongoing studies and real-world data, the understanding of booster shots' role in prolonged immunity will further improve, guiding more effective vaccination strategies.
Polio Vaccine: Lifetime Protection or Not?
You may want to see also
Explore related products






![]()
Vaccine Platforms: mRNA, viral vector, protein subunit, and inactivated virus technologies
The development and deployment of COVID-19 vaccines have relied on several innovative vaccine platforms, each with distinct mechanisms and stages of production. These platforms include mRNA, viral vector, protein subunit, and inactivated virus technologies. Understanding these platforms is crucial to grasping the stages involved in creating a coronavirus vaccine. Each platform follows a unique process, but all share common stages such as research and development, preclinical testing, clinical trials, manufacturing, and distribution.
MRNA (Messenger RNA) technology is one of the most groundbreaking platforms used in COVID-19 vaccines, such as those developed by Pfizer-BioNTech and Moderna. In this platform, the vaccine delivers genetic material (mRNA) that instructs cells to produce a harmless piece of the SARS-CoV-2 spike protein, triggering an immune response. The stages here include designing the mRNA sequence, encapsulating it in lipid nanoparticles for stability, preclinical testing in animals, and three phases of clinical trials to ensure safety and efficacy. Once approved, large-scale manufacturing involves synthesizing the mRNA and formulating it with delivery agents, followed by distribution under specific storage conditions (e.g., ultra-cold temperatures for Pfizer’s vaccine).
Viral vector technology, used in vaccines like AstraZeneca and Johnson & Johnson, employs a modified, harmless virus (the vector) to deliver genetic material encoding the SARS-CoV-2 spike protein into cells. The stages begin with selecting and engineering the vector virus, followed by preclinical studies to assess safety and immunogenicity. Clinical trials then evaluate the vaccine’s effectiveness and side effects. Manufacturing involves growing the vector virus in cell cultures, purifying it, and formulating the final product. Distribution is relatively simpler compared to mRNA vaccines, as viral vector vaccines typically require standard refrigeration.
Protein subunit vaccines, such as Novavax, focus on delivering a specific piece of the virus (e.g., the spike protein) without introducing genetic material. The stages include identifying and synthesizing the protein antigen, often using recombinant DNA technology in insect or mammalian cells. Preclinical testing ensures the protein elicits a strong immune response. Clinical trials then assess safety and efficacy. Manufacturing involves large-scale protein production, purification, and formulation with adjuvants to enhance immunity. Distribution is straightforward, as these vaccines are stable at standard refrigeration temperatures.
Inactivated virus vaccines, such as Sinovac and Sinopharm, use a whole SARS-CoV-2 virus that has been killed or inactivated to prevent infection while still provoking an immune response. The stages start with growing the virus in cell cultures, inactivating it using chemicals or heat, and purifying the viral particles. Preclinical studies confirm the vaccine’s safety and immunogenicity. Clinical trials evaluate its effectiveness and potential side effects. Manufacturing involves large-scale virus cultivation, inactivation, and formulation. These vaccines are typically distributed under standard refrigeration conditions, making them accessible in resource-limited settings.
In summary, while the number of stages in developing a coronavirus vaccine remains consistent across platforms—research, preclinical testing, clinical trials, manufacturing, and distribution—the specific processes within each stage vary significantly depending on the technology used. mRNA and viral vector vaccines rely on genetic material delivery, protein subunit vaccines focus on specific antigens, and inactivated virus vaccines use the whole virus. Each platform offers unique advantages and challenges, contributing to the diverse global vaccine portfolio against COVID-19.
Polio Vaccine in the 1950s: Methods, Challenges, and Impact
You may want to see also
Explore related products




![]()
Global Distribution Stages: Manufacturing, allocation, and equitable access challenges worldwide
The global distribution of COVID-19 vaccines involves a complex process that spans multiple stages, each presenting unique challenges. The first critical stage is manufacturing, which requires a coordinated effort to produce vaccines at an unprecedented scale. Pharmaceutical companies and manufacturers face hurdles such as securing raw materials, scaling up production facilities, and maintaining quality control. For instance, mRNA vaccines like Pfizer-BioNTech and Moderna demand specialized materials like lipid nanoparticles, which are in high demand and limited supply. Additionally, manufacturing capacity varies widely between high-income and low-income countries, with many low-income nations lacking the infrastructure to produce vaccines domestically. This disparity has led to a heavy reliance on imports, often delayed due to logistical bottlenecks and export restrictions imposed by some countries.
The next stage is allocation, which involves distributing vaccines to countries based on agreements, purchasing power, and global initiatives. Wealthier nations have secured the majority of early vaccine doses through advance purchase agreements, leaving low- and middle-income countries at a disadvantage. Initiatives like COVAX, a global collaboration to ensure equitable access, have aimed to address this imbalance by pooling resources and negotiating deals on behalf of poorer nations. However, COVAX has faced challenges such as funding shortages, delayed deliveries, and limited vaccine supplies, particularly as wealthier countries prioritize their own populations. This has exacerbated vaccine inequity, with some countries administering booster doses while others struggle to vaccinate even their most vulnerable populations.
Equitable access is the final and most critical stage, ensuring vaccines reach all populations regardless of geographic, economic, or social barriers. This stage is fraught with challenges, including weak healthcare systems in many low-income countries, vaccine hesitancy, and logistical issues like cold chain requirements for certain vaccines. For example, the Pfizer-BioNTech vaccine requires ultra-cold storage, which is difficult to maintain in regions with unreliable electricity or limited infrastructure. Furthermore, political instability, corruption, and bureaucratic inefficiencies in some countries hinder effective vaccine rollout. Addressing these challenges requires international cooperation, financial support, and innovative solutions like mobile vaccination units and community engagement programs.
Another layer of complexity arises from intellectual property rights and technology transfer. High-income countries and pharmaceutical companies have been reluctant to waive patent protections, limiting the ability of low-income countries to produce vaccines locally. While the World Trade Organization (WTO) has discussed a temporary waiver, negotiations have been slow, delaying potential solutions. Meanwhile, efforts to transfer technology and know-how to manufacturers in low-income countries, such as the mRNA vaccine hub in South Africa, offer hope but are still in early stages. These challenges highlight the need for a more equitable global health framework that prioritizes collective well-being over profit.
In conclusion, the global distribution of COVID-19 vaccines is a multi-stage process that involves manufacturing, allocation, and ensuring equitable access. Each stage presents distinct challenges, from scaling up production and securing supplies to addressing logistical hurdles and systemic inequities. Overcoming these obstacles requires sustained international collaboration, innovative solutions, and a commitment to global solidarity. Without addressing these issues, the world risks prolonged pandemics, new variants, and deepened inequalities, underscoring the urgency of a coordinated and equitable approach to vaccine distribution.
Anti-Vaccine Movements: Undermining Public Health Progress and Global Safety
You may want to see also
Frequently asked questions
The development of a COVID-19 vaccine typically involves three main stages: preclinical testing (laboratory and animal studies), clinical trials (Phase 1, 2, and 3 involving human volunteers), and regulatory review and approval.
Yes, after approval, there are post-approval stages, including Phase 4 trials (post-market surveillance) to monitor long-term safety and efficacy, as well as manufacturing and distribution processes.
Yes, all COVID-19 vaccines must undergo the same rigorous stages of development, testing, and approval, though the timeline may vary depending on the manufacturer and regulatory requirements.