The global vaccination effort against COVID-19 has been one of the most significant public health initiatives in history, with billions of doses administered worldwide. As of recent data, over 13 billion vaccine doses have been given, covering a substantial portion of the global population. However, the distribution of vaccines remains uneven, with disparities between high-income and low-income countries. While many developed nations have achieved high vaccination rates, with some populations receiving booster shots, many low-income countries still struggle to vaccinate even a small fraction of their citizens. Tracking the number of vaccinated individuals is crucial for understanding the progress of immunization campaigns, identifying gaps in coverage, and guiding public health policies to control the spread of the virus and its variants.
Explore related products



$18.59 $19.95



What You'll Learn
![]()
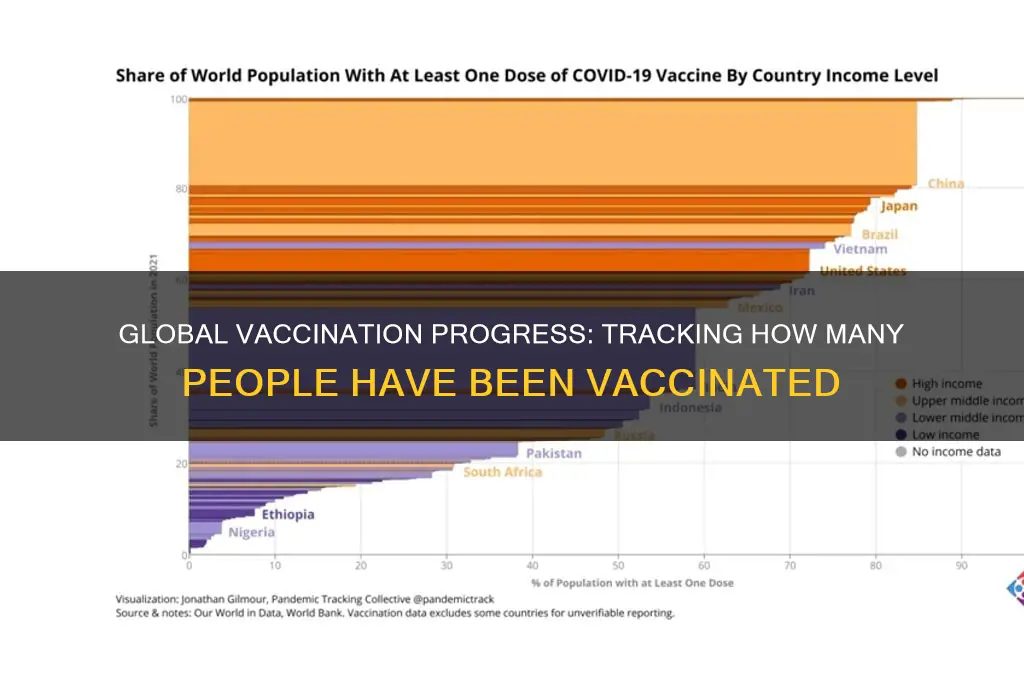
Global vaccination rates by region
As of the latest data, global vaccination rates vary significantly by region, influenced by factors such as healthcare infrastructure, economic resources, and public health policies. North America and Europe lead with vaccination rates exceeding 70% for at least one dose, driven by robust distribution networks and early access to vaccines. For instance, the United States has administered over 670 million doses, with 80% of adults receiving at least one shot. In contrast, Africa lags behind, with only 24% of its population partially vaccinated, largely due to supply chain challenges and vaccine hesitancy.
Analyzing these disparities reveals a stark divide in global health equity. High-income regions like Western Europe have not only achieved high vaccination rates but also begun administering booster doses, with countries like Portugal and Denmark leading at over 60% booster coverage. Meanwhile, low-income regions, particularly in sub-Saharan Africa, struggle to secure even initial doses. For example, in Nigeria, only 4% of the population is fully vaccinated, despite being Africa’s most populous nation. This gap underscores the need for targeted global initiatives like COVAX, which aims to distribute 2 billion doses to low-income countries by 2022.
Instructively, regions like Southeast Asia demonstrate how strategic planning can bridge vaccination gaps. Countries such as Singapore and Malaysia have achieved over 80% full vaccination rates through mass vaccination sites, digital health passes, and public awareness campaigns. Conversely, South Asia faces challenges, with India partially vaccinating 60% of its population but struggling with rural access. Practical tips for improving regional rates include leveraging local leaders to combat misinformation, using mobile clinics for hard-to-reach areas, and prioritizing dose-sharing agreements between high- and low-income nations.
Comparatively, the Middle East and Latin America present mixed progress. The United Arab Emirates boasts one of the highest global vaccination rates at 99%, thanks to aggressive procurement and mandatory vaccination policies. In contrast, Latin America averages 65% partial vaccination, with Brazil at 80% and Haiti at a mere 1%, highlighting disparities within regions. Age-specific strategies, such as prioritizing elderly populations in Latin America, have proven effective, while the Middle East’s focus on expat communities has ensured broader coverage.
Persuasively, closing the regional vaccination gap requires a multifaceted approach. Wealthier nations must fulfill dose-sharing pledges, while low-income regions should invest in cold chain infrastructure and community health workers. For instance, Rwanda’s 60% vaccination rate, achieved through drone deliveries and village-level campaigns, offers a replicable model. Ultimately, global health security depends on equitable access, not just regional successes. As new variants emerge, the world must act collectively, ensuring no region is left behind in the fight against the pandemic.
Vaccinating Teachers First: A Key to Safe School Reopenings?
You may want to see also
Explore related products






![]()
Age-specific vaccination coverage data
As of the latest global health reports, vaccination coverage varies significantly across age groups, reflecting disparities in access, awareness, and policy focus. For instance, in many countries, children under 5 years old often achieve higher vaccination rates for diseases like measles and polio due to robust immunization programs targeting this vulnerable demographic. However, adolescents and young adults (ages 15–24) frequently lag in coverage for vaccines such as HPV and meningitis, partly due to lower prioritization in public health campaigns. Understanding these age-specific trends is critical for tailoring interventions to close gaps and ensure equitable protection across all life stages.
Analyzing age-specific vaccination coverage data reveals both successes and challenges. For example, the COVID-19 vaccine rollout highlighted stark differences: in the U.S., over 90% of individuals aged 65 and older received at least one dose by mid-2022, driven by early eligibility and targeted outreach. In contrast, only 60% of 18–29-year-olds were vaccinated during the same period, attributed to hesitancy, misinformation, and lower perceived risk. Such data underscores the need for age-tailored strategies, such as leveraging social media for younger audiences or partnering with senior centers for older adults, to address unique barriers to uptake.
To improve age-specific vaccination coverage, public health officials must adopt a multi-pronged approach. For children, integrating vaccines into routine pediatric care and school enrollment requirements remains effective. For adults, workplace vaccination drives and reminders tied to annual health checks can boost participation. Specific age groups, like pregnant women, require targeted education on the safety and benefits of vaccines such as Tdap and influenza. Practical tips include offering flexible clinic hours for working-age adults and providing mobile vaccination units in underserved areas to reach all age demographics.
Comparatively, countries with high overall vaccination rates often excel in age-specific coverage by embedding immunization across life stages. For instance, Japan’s elderly population has near-universal influenza vaccination due to government subsidies and public awareness campaigns. Conversely, low-income nations struggle with adolescent vaccination, as seen in sub-Saharan Africa, where only 20% of girls receive the HPV vaccine. These examples illustrate that successful age-specific strategies depend on resource allocation, cultural sensitivity, and sustained political commitment.
In conclusion, age-specific vaccination coverage data is a powerful tool for identifying vulnerabilities and optimizing public health efforts. By dissecting trends, implementing targeted interventions, and learning from global examples, societies can ensure that no age group is left behind in the pursuit of herd immunity. Whether through policy adjustments, community engagement, or innovative delivery methods, the goal remains clear: to protect every individual, regardless of age, through timely and equitable vaccination.
Empowering Conversations: Strategies to Engage and Educate Anti-Vaxxers on Vaccines
You may want to see also
Explore related products






![]()
Vaccine distribution disparities worldwide
As of the latest data, over 13 billion COVID-19 vaccine doses have been administered globally, yet this staggering number masks a stark reality: vaccine distribution remains deeply inequitable. High-income countries, representing just 16% of the world’s population, have secured nearly 50% of all vaccine doses. In contrast, low-income countries, home to 9% of the global population, have received less than 1% of doses. This disparity is not merely a statistic but a reflection of systemic failures in global health governance, where profit motives and geopolitical interests often overshadow equitable access.
Consider the COVAX initiative, a global effort to ensure fair vaccine distribution, which aimed to deliver 2 billion doses by the end of 2021. It fell short, distributing only 1.4 billion doses by that deadline. Wealthy nations hoarded vaccines, with some purchasing doses up to three times their population size, while many African countries struggled to vaccinate even 10% of their populations. For instance, as of late 2023, countries like Canada and the U.S. had administered booster doses to over 50% of their populations, whereas in low-income nations like Chad and South Sudan, less than 10% had received even a single dose. This imbalance exacerbates health crises, allowing variants to emerge in under-vaccinated regions and prolonging the pandemic globally.
The root of this disparity lies in the global vaccine supply chain, dominated by pharmaceutical giants in high-income countries. Patents and intellectual property rights restrict low-income nations from producing vaccines locally, forcing them to rely on donations or overpriced imports. For example, the mRNA technology used in Pfizer and Moderna vaccines remains inaccessible to most of the Global South, despite calls for patent waivers. Meanwhile, logistical challenges—such as cold chain requirements for certain vaccines—further marginalize regions with limited infrastructure. A practical solution would involve transferring technology and waiving patents to enable local production, as seen in India’s success with the Oxford-AstraZeneca vaccine.
To address this inequity, a multi-faceted approach is essential. First, high-income nations must fulfill their dose-sharing pledges without delay. Second, global health organizations should prioritize funding for local vaccine manufacturing in low-income countries. Third, governments and NGOs must invest in strengthening healthcare systems to ensure vaccines reach remote populations. For instance, mobile vaccination clinics and community health workers have proven effective in countries like Rwanda and Bangladesh. Finally, individuals in wealthy nations can advocate for policy changes and support organizations like Gavi, the Vaccine Alliance, which works to improve vaccine access in underserved regions.
In conclusion, while billions have been vaccinated, the global effort remains incomplete without addressing distribution disparities. The pandemic has underscored the interconnectedness of global health—no one is safe until everyone is safe. By dismantling barriers to equitable access, the world can not only end this pandemic but also build a more resilient health system for future crises. The question is not whether we can achieve equity, but whether we have the collective will to do so.
RTS,S Vaccine: Unique Features Compared to Traditional Vaccines
You may want to see also
Explore related products






![]()
Booster shot administration statistics
As of the latest global health reports, booster shot administration has become a critical component in maintaining immunity against COVID-19, with over 60% of fully vaccinated individuals in high-income countries having received at least one booster dose. This statistic highlights a significant disparity compared to low-income nations, where less than 20% of the population has accessed boosters due to supply chain limitations and vaccine hesitancy.
Analyzing the data reveals that booster uptake is highest among individuals aged 65 and older, with nearly 80% in this demographic receiving additional doses in countries like the United States and the United Kingdom. This trend is driven by targeted public health campaigns emphasizing the heightened risk of severe illness in older adults. Conversely, younger age groups (18–40) show lower booster acceptance rates, often due to misconceptions about reduced vulnerability or concerns over side effects.
Practical implementation of booster programs varies widely. In Israel, a pioneering country in vaccine rollout, a fourth dose was offered to immunocompromised individuals and those over 60, with a 500-microgram mRNA dose administered at least four months after the third shot. In contrast, the European Union recommends a 30-microgram dose for boosters, aligning with initial vaccine regimens. These differences underscore the importance of localized strategies based on population health needs and vaccine availability.
Persuasively, booster statistics also reflect the evolving nature of vaccine efficacy. Studies show that while initial doses provide robust protection against severe disease for 6–8 months, antibody levels wane over time, particularly against variants like Omicron. Boosters restore efficacy to over 90% against hospitalization and death, making them indispensable in regions with high transmission rates.
To optimize booster administration, public health officials should prioritize clear communication about dosage intervals, eligibility criteria, and the safety profile of repeated vaccinations. Mobile clinics, workplace vaccination drives, and digital reminders can improve accessibility, especially in underserved communities. By addressing logistical barriers and misinformation, countries can bridge the booster gap and sustain collective immunity.
Meningococcal Vaccine Record: What Should Be Documented After Your Shot?
You may want to see also
Explore related products






![]()
Vaccination rates by vaccine type
As of the latest global health reports, COVID-19 vaccines have dominated vaccination discussions, but other vaccine types—such as influenza, measles, and HPV—show vastly different uptake rates. For instance, annual influenza vaccination rates in the U.S. hover around 45-50% for adults, compared to over 70% for at least one COVID-19 dose. This disparity highlights how vaccine type, perceived urgency, and public health messaging influence behavior. While COVID-19 vaccines were rapidly adopted due to pandemic pressures, routine immunizations like HPV (human papillomavirus) lag, with only 54% of U.S. adolescents completing the series. Understanding these variations is critical for tailoring public health strategies to specific vaccine challenges.
Consider the measles vaccine, a cornerstone of childhood immunization, which boasts a global first-dose coverage of approximately 83%. However, this figure masks regional disparities: high-income countries often achieve 95% coverage, while low-income nations struggle to reach 70%. The measles vaccine requires two doses for full protection, yet only 71% of children worldwide receive the second dose. This gap underscores the logistical and economic barriers in distributing multi-dose vaccines, particularly in resource-constrained settings. For parents, ensuring timely second doses—typically administered between ages 4-6—is crucial to closing this immunity gap.
In contrast, the HPV vaccine, which prevents cancers caused by human papillomavirus, faces unique adoption hurdles. Despite its proven efficacy, global coverage remains low, with only 45% of girls and 17% of boys receiving at least one dose. Misconceptions about HPV as solely a sexual health issue, coupled with higher costs and limited availability in low-income countries, contribute to this lag. Public health campaigns emphasizing HPV vaccination as a cancer prevention tool, not just an STI measure, could shift perceptions. Clinicians should recommend the vaccine for adolescents aged 11-12, with a catch-up window up to age 26, to maximize impact.
The influenza vaccine exemplifies seasonal variability in uptake, influenced by factors like vaccine efficacy predictions and public fatigue. In the 2022-2023 season, only 48.3% of U.S. adults received the flu shot, despite its annual reformulation to match circulating strains. Employers and schools can boost rates by offering on-site vaccination clinics and educating on the vaccine’s 40-60% efficacy in preventing illness. For older adults, the high-dose flu vaccine, containing four times the antigen of standard doses, is recommended to enhance immune response, yet only 35% opt for this version.
Finally, the COVID-19 vaccine rollout demonstrates how rapid development and distribution can achieve high initial uptake but struggle with long-term adherence. Globally, 69% of the population has received at least one dose, but booster rates plummet to 30-40% in many countries. Hesitancy, access issues, and misinformation about side effects contribute to this drop. Health systems must prioritize equitable access to boosters, particularly for immunocompromised individuals requiring three primary doses plus annual boosters. Clear communication about evolving variants and updated formulations is essential to sustain trust and participation.
Original COVID-19 Vaccines: Omicron Protection Efficacy Explained
You may want to see also
Frequently asked questions
As of 2023, over 13 billion COVID-19 vaccine doses have been administered globally, with more than 5 billion people receiving at least one dose.
As of 2023, countries like Portugal, Singapore, and the United Arab Emirates have some of the highest vaccination rates, with over 90% of their populations fully vaccinated against COVID-19.
As of 2023, over 265 million people in the United States have received at least one dose of a COVID-19 vaccine, with more than 225 million fully vaccinated.