As of the latest global health reports, the percentage of the world's population that has received at least one dose of a COVID-19 vaccine stands at approximately 65%, with significant variations across regions. High-income countries have achieved vaccination rates exceeding 80%, while many low-income nations struggle to reach 20% due to disparities in vaccine distribution, infrastructure, and hesitancy. Efforts by international organizations like COVAX aim to bridge this gap, but challenges persist in ensuring equitable access to vaccines worldwide. Monitoring these figures is crucial for understanding the progress and challenges in achieving global immunity against the pandemic.
Explore related products
![International Certificate of Vaccination with Vinyl Document Holder - World Health Organization Bilingual Version [cards] World Health Organization [Jan 01, 2007]](https://m.media-amazon.com/images/I/61SHjBP1VYL._AC_UY218_.jpg)





What You'll Learn
![]()
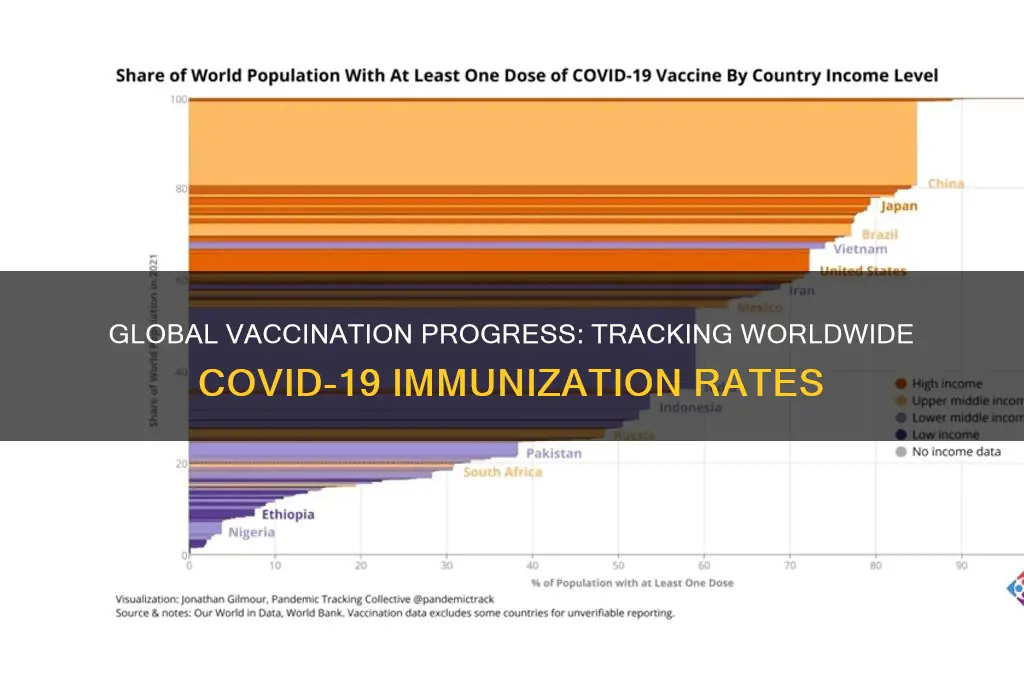
Global Vaccination Rates by Region
As of the latest data, global vaccination rates against COVID-19 reveal stark disparities across regions, with high-income countries outpacing low-income nations by significant margins. For instance, over 70% of the population in North America and Europe has received at least one dose, while in Africa, this figure hovers around 20%. This gap underscores the inequities in vaccine distribution and access, influenced by factors like funding, infrastructure, and political will. Such regional variations not only affect local health outcomes but also impact global efforts to control the pandemic.
Analyzing these disparities, it becomes clear that wealthier regions have leveraged their resources to secure vaccine supplies and implement efficient rollout strategies. For example, the European Union and the United States have administered booster doses to a substantial portion of their populations, with some countries offering fourth doses to vulnerable groups. In contrast, many African nations struggle to secure even initial doses due to limited funding and logistical challenges. This imbalance highlights the need for global initiatives like COVAX, which aims to provide equitable vaccine access but has faced hurdles in meeting its targets.
From a practical standpoint, regions with lower vaccination rates must prioritize targeted strategies to overcome barriers. For instance, mobile vaccination clinics have proven effective in reaching rural populations in South Asia, while community-led campaigns in Latin America have boosted trust in vaccines. Additionally, simplifying registration processes and offering flexible vaccination hours can improve uptake. For parents, ensuring children aged 5 and older receive their doses is critical, as many regions now approve vaccines for this age group.
Comparatively, regions with high vaccination rates offer lessons in coordination and public engagement. Countries like Singapore and the United Arab Emirates achieved over 90% vaccination rates through mandatory policies, incentives, and clear communication. However, these approaches may not be replicable everywhere, as cultural and political contexts vary. Instead, low-coverage regions can adapt strategies like leveraging local leaders to dispel myths or using digital tools to track and encourage vaccination, ensuring efforts are tailored to their unique challenges.
In conclusion, addressing global vaccination disparities requires a multi-faceted approach that considers regional realities. High-income nations must fulfill funding pledges and share surplus doses, while low-income regions need to focus on localized solutions that enhance accessibility and build trust. By learning from both successes and shortcomings across regions, the world can move closer to achieving equitable vaccine coverage and mitigating the pandemic’s impact.
Ebola Virus Vaccine: Is There Hope?
You may want to see also
Explore related products






![]()
Vaccination Progress in Low-Income Countries
As of recent data, approximately 68% of the global population has received at least one dose of a COVID-19 vaccine, but this figure masks stark disparities. In low-income countries, the vaccination rate plummets to around 20%, a statistic that underscores the persistent challenges these nations face in achieving equitable vaccine access. While high-income countries have administered booster doses and expanded eligibility to younger age groups, many low-income nations are still struggling to secure first doses for their most vulnerable populations, including healthcare workers and the elderly.
One critical factor hindering progress is the logistical complexity of vaccine distribution. Low-income countries often lack the infrastructure for cold-chain storage, particularly for mRNA vaccines that require ultra-low temperatures. For instance, the Pfizer-BioNTech vaccine must be stored at -70°C, a requirement that is nearly impossible to meet in regions with unreliable electricity or limited refrigeration capacity. In contrast, the Oxford-AstraZeneca vaccine, which can be stored at standard refrigerator temperatures (2–8°C), has been more widely distributed in these settings. However, even this option is constrained by supply shortages and funding gaps.
To address these challenges, global initiatives like COVAX aimed to provide 2 billion vaccine doses to low-income countries by the end of 2021. Yet, the program fell short of its target, delivering only 1.2 billion doses due to vaccine hoarding by wealthier nations and export restrictions by manufacturing countries. This disparity highlights the need for a more equitable global vaccine distribution framework, one that prioritizes the needs of low-income countries over profit-driven models. For example, waiving intellectual property rights for COVID-19 vaccines could enable local production in low-income regions, reducing dependency on imports and accelerating vaccination rates.
Another practical step is to tailor vaccination strategies to the unique contexts of low-income countries. Mobile vaccination clinics, for instance, have proven effective in reaching remote populations in countries like Rwanda and Ghana. These clinics often operate in partnership with community health workers who are trained to administer doses and educate locals about vaccine safety. Additionally, leveraging existing immunization programs, such as those for measles or polio, can streamline vaccine delivery and build public trust. For children aged 5–11, who are now eligible for vaccination in many countries, integrating COVID-19 vaccines into routine school health programs could be a viable strategy.
Despite these efforts, vaccine hesitancy remains a significant barrier. Misinformation, fueled by social media and cultural beliefs, has led to skepticism in some communities. Addressing this requires culturally sensitive communication campaigns that involve local leaders and trusted figures. For example, in India, community radio stations were used to disseminate accurate information in regional languages, increasing vaccine uptake in rural areas. Similarly, in Nigeria, religious leaders played a pivotal role in encouraging vaccination among their congregations.
In conclusion, while global vaccination efforts have made strides, low-income countries continue to lag behind due to systemic inequalities. Bridging this gap requires a multifaceted approach: improving infrastructure, ensuring equitable vaccine distribution, adapting strategies to local contexts, and combating misinformation. Without concerted global action, the goal of achieving widespread immunity remains elusive, leaving the door open for new variants and prolonged health crises.
Developing HIV and HCV Vaccines: A Global Health Imperative or Challenge?
You may want to see also
Explore related products






![]()
Impact of Vaccine Hesitancy on Coverage
As of recent data, approximately 68% of the world’s population has received at least one dose of a COVID-19 vaccine, yet disparities in coverage persist, particularly in low-income countries where the rate drops to around 25%. Vaccine hesitancy, defined by the WHO as the delay in acceptance or refusal of vaccines despite availability, plays a significant role in these gaps. In regions like Eastern Europe and parts of Africa, hesitancy rates exceed 30%, directly correlating with lower vaccination coverage. This reluctance isn’t confined to COVID-19; it affects routine immunizations, such as measles, where global coverage has dropped below the 95% threshold needed for herd immunity.
Consider the mechanics of vaccine hesitancy: it thrives on misinformation, cultural mistrust, and systemic barriers. For instance, in the Democratic Republic of Congo, polio vaccination campaigns faced resistance due to rumors linking vaccines to sterilization, reducing coverage to 60% in some areas. Similarly, in the U.S., counties with high social media consumption of anti-vaccine content saw COVID-19 vaccination rates 10-15% lower than national averages. Hesitancy doesn’t just lower individual protection; it weakens herd immunity, leaving vulnerable populations—infants, the immunocompromised, and the elderly—at risk. A 5% drop in measles vaccination coverage can lead to a 50% increase in cases, as seen in Europe in 2019.
To combat hesitancy, tailored strategies are essential. In India, the government partnered with local religious leaders to dispel myths, increasing vaccine uptake by 20% in rural areas. In Brazil, mobile clinics offering vaccines alongside health screenings improved coverage among hesitant populations by addressing accessibility and trust simultaneously. For parents, framing vaccines as a social responsibility rather than a personal choice has proven effective. For example, emphasizing that the MMR vaccine (two doses, typically given at 12-15 months and 4-6 years) protects not just the child but also classmates with weakened immune systems can shift perspectives.
However, addressing hesitancy requires more than education. Systemic issues, like inconsistent vaccine supply or healthcare worker shortages, must be resolved. In Nigeria, a 2021 initiative trained community health workers to administer vaccines, increasing coverage by 15% in underserved regions. Similarly, in Japan, simplifying registration processes for COVID-19 vaccines boosted participation among elderly populations by 25%. Practical tips for healthcare providers include using clear, non-technical language, offering flexible appointment times, and leveraging peer testimonials to build trust.
Ultimately, the impact of vaccine hesitancy on coverage is a solvable problem, but it demands a multi-faceted approach. By understanding local concerns, improving access, and fostering trust, even the most hesitant communities can be reached. The goal isn’t just to increase percentages but to ensure that vaccines serve their purpose: protecting everyone, everywhere.
Queen Elizabeth's Passing: Unraveling Vaccine Conspiracy Theories and Facts
You may want to see also
Explore related products

$22 $28


$19.95 $19.95



![]()
Distribution of COVID-19 Vaccines Worldwide
As of recent data, approximately 68% of the world’s population has received at least one dose of a COVID-19 vaccine, with significant disparities across regions. High-income countries, such as those in North America and Western Europe, have achieved vaccination rates exceeding 75%, while many low-income nations in Africa and parts of Asia struggle to reach 20%. This uneven distribution highlights the challenges of global vaccine equity, where access to doses remains a critical issue despite the availability of multiple vaccines.
One of the primary factors influencing vaccine distribution is the COVAX initiative, a global collaboration aimed at ensuring equitable access to COVID-19 vaccines. While COVAX has delivered over 2 billion doses to 146 countries, it has fallen short of its initial targets due to funding gaps, logistical hurdles, and vaccine hoarding by wealthier nations. For instance, Canada and the United States secured enough doses to vaccinate their populations multiple times over, while countries like Haiti and the Democratic Republic of Congo received only a fraction of their required doses. This disparity underscores the need for stronger international cooperation and resource allocation.
Another critical aspect of vaccine distribution is the role of local infrastructure and public health systems. In many low-income countries, inadequate cold chain facilities, limited healthcare workers, and vaccine hesitancy have hindered rollout efforts. For example, the Pfizer-BioNTech vaccine requires ultra-cold storage (-70°C), making it impractical for regions with unreliable electricity. In contrast, vaccines like AstraZeneca and Johnson & Johnson, which are more heat-stable, have been more widely distributed in resource-constrained settings. Tailoring vaccine choices to local conditions is essential for maximizing impact.
Practical steps to improve distribution include increasing dose-sharing commitments from high-income countries, investing in local manufacturing capacity, and addressing misinformation through community-based campaigns. For instance, India’s Serum Institute, the world’s largest vaccine manufacturer, played a pivotal role in supplying doses to low-income nations. Similarly, South Africa’s partnership with Johnson & Johnson to produce vaccines locally serves as a model for regional self-sufficiency. These efforts demonstrate that equitable distribution is not just a moral imperative but a practical solution to ending the pandemic.
In conclusion, the distribution of COVID-19 vaccines worldwide remains a complex and uneven process, shaped by economic disparities, logistical challenges, and political priorities. While progress has been made, achieving global immunity requires sustained commitment to equity, innovation, and collaboration. By learning from successful initiatives and addressing systemic barriers, the international community can ensure that vaccines reach those who need them most, regardless of geography or income.
Essential School Vaccines: What Kids Need Before Starting Classes
You may want to see also
Explore related products






![]()
Fully vs. Partially Vaccinated Population Statistics
As of the latest global health reports, approximately 68% of the world’s population has received at least one dose of a COVID-19 vaccine, while only 60% are fully vaccinated. This 8% gap highlights a critical distinction: partial vaccination offers some protection, but full vaccination significantly reduces severe illness, hospitalization, and death. For instance, a single dose of the Pfizer-BioNTech vaccine provides around 52% efficacy against symptomatic infection, whereas two doses boost this to 95%. This disparity underscores the importance of completing the recommended vaccine regimen, typically two doses for mRNA vaccines and one or two for viral vector or inactivated vaccines.
Consider the practical implications for different age groups. Children aged 5–11 often require two doses of a pediatric formulation (e.g., 10 micrograms per dose for Pfizer), while adolescents and adults receive higher dosages (30 micrograms). In regions with limited access to second doses, partially vaccinated individuals, especially the elderly or immunocompromised, remain at higher risk. For example, in low-income countries, where only 20% of the population is fully vaccinated, partial vaccination may still provide a temporary shield, but it’s insufficient for long-term protection. This emphasizes the need for equitable global vaccine distribution to ensure full coverage.
From a comparative perspective, the difference between partial and full vaccination is akin to wearing a seatbelt without buckling it—it offers some benefit but falls short of maximum safety. Partially vaccinated individuals may still transmit the virus, particularly with variants like Omicron, which evade immunity more easily. A study in *The Lancet* found that two doses of AstraZeneca reduced symptomatic infection by 70%, but this dropped to 40% after six months, reinforcing the need for boosters. Similarly, mixing vaccine types (e.g., AstraZeneca followed by Pfizer) has shown enhanced immune responses, providing a strategy for regions facing supply shortages.
To bridge the gap between partial and full vaccination, policymakers must address logistical challenges. Mobile vaccination units, community outreach, and digital reminders can improve second-dose uptake. In India, for instance, the CoWIN app sends automated notifications for follow-up doses, increasing compliance. Additionally, debunking misinformation about vaccine side effects is crucial. Mild symptoms like fatigue or fever after the first dose should not deter individuals from completing their regimen, as these are signs of immune activation, not danger.
In conclusion, the divide between partial and full vaccination is not just statistical—it’s a matter of life and death. While partial vaccination is a step in the right direction, it’s the second dose that completes the protective barrier. Governments, healthcare providers, and individuals must prioritize full vaccination to achieve herd immunity and curb the pandemic’s impact. As the saying goes, “Half measures avail us nothing”—a lesson that holds true in global health as much as anywhere else.
Fully Vaccinated and COVID-19: Rare Breakthrough Deaths Explained
You may want to see also
Frequently asked questions
As of 2023, approximately 68% of the world's population has received at least one dose of a COVID-19 vaccine, with around 60% fully vaccinated.
High-income regions, such as North America, Western Europe, and parts of Asia (e.g., Singapore and the UAE), have the highest vaccination rates, often exceeding 80% fully vaccinated.
Lower vaccination rates in low-income countries are primarily due to limited access to vaccines, inadequate healthcare infrastructure, vaccine hesitancy, and logistical challenges in distribution.
Higher global vaccination rates reduce severe illness, hospitalizations, and deaths, but uneven distribution and emerging variants continue to pose challenges to ending the pandemic.