The question of how many people in a given population have been vaccinated is a critical indicator of public health resilience, particularly in the context of global health crises such as pandemics. Vaccination rates provide insights into the effectiveness of public health campaigns, the accessibility of healthcare services, and the level of community immunity, which is essential for protecting vulnerable populations. Understanding these figures helps policymakers, healthcare providers, and the public gauge progress toward herd immunity, identify gaps in vaccine distribution, and address hesitancy or misinformation. As vaccination efforts continue to evolve, tracking these numbers remains a cornerstone of monitoring and improving global health outcomes.
Explore related products



$11.93 $21.99



What You'll Learn
![]()
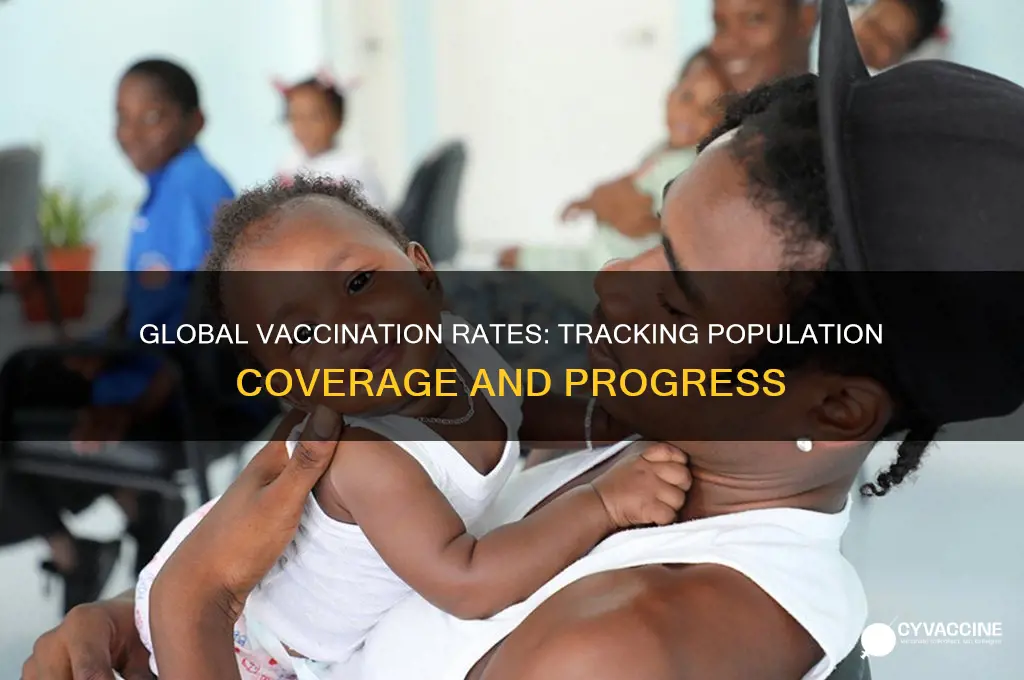
Global vaccination rates by country
As of the latest data, global vaccination rates against COVID-19 vary significantly by country, influenced by factors such as vaccine availability, healthcare infrastructure, and public health policies. High-income countries have generally achieved higher vaccination rates compared to low- and middle-income nations. For instance, countries like Canada, Portugal, and Singapore report that over 80% of their populations have received at least one dose of a COVID-19 vaccine. These nations have benefited from early access to vaccines, efficient distribution systems, and strong public health campaigns promoting vaccination.
In contrast, many African countries continue to face challenges in vaccinating their populations. As of recent reports, countries like Nigeria, Ethiopia, and the Democratic Republic of Congo have vaccinated less than 20% of their populations. Limited vaccine supply, logistical hurdles, and vaccine hesitancy have contributed to these lower rates. However, initiatives like COVAX, a global vaccine-sharing program, have aimed to bridge this gap by providing doses to lower-income countries, though distribution challenges persist.
Middle-income countries present a mixed picture. Some, like Brazil and India, have made significant progress, with over 70% of their populations vaccinated, thanks to domestic vaccine production and targeted campaigns. Others, such as Indonesia and the Philippines, have achieved moderate rates, with around 50-60% of their populations vaccinated. These countries often face challenges balancing vaccine distribution across diverse and geographically dispersed populations.
In Europe, vaccination rates vary widely. Western European countries like France, Germany, and the UK have vaccinated over 70% of their populations, while Eastern European nations like Bulgaria and Romania lag behind, with rates below 40%. Vaccine hesitancy and political factors have played a significant role in these disparities. Meanwhile, small European nations like Malta and Iceland have achieved some of the highest vaccination rates globally, with over 90% of their populations fully vaccinated.
In Asia, vaccination rates differ dramatically. Countries like the United Arab Emirates and Japan have vaccinated over 80% of their populations, while others like Pakistan and Myanmar have rates below 30%. Economic disparities, political instability, and access to vaccines are key factors influencing these variations. China, with its domestically produced vaccines, has vaccinated over 85% of its population, showcasing the impact of national vaccine production capabilities.
Overall, global vaccination rates highlight the inequities in vaccine access and distribution. While some countries have successfully vaccinated the majority of their populations, others continue to struggle. Addressing these disparities requires continued international cooperation, investment in healthcare infrastructure, and efforts to combat vaccine hesitancy. Monitoring these rates remains crucial for global health security and pandemic preparedness.
Vaccination Status: Rights and Workplace Disclosure
You may want to see also
Explore related products






![]()
Age group distribution of vaccinated individuals
As of the latest data, the distribution of vaccinated individuals across different age groups varies significantly, reflecting both the prioritization strategies implemented during vaccine rollouts and the evolving eligibility criteria. In most countries, the initial phases of vaccination campaigns prioritized older adults, typically those aged 65 and above, due to their higher risk of severe illness and mortality from COVID-19. As a result, this age group often shows the highest vaccination rates, with many countries reporting over 80-90% of seniors fully vaccinated. This targeted approach has been instrumental in reducing hospitalizations and deaths among the elderly population.
The next age group, typically those aged 50 to 64, also benefited from early vaccination drives, as they were often included in the second phase of rollouts. This group has seen substantial vaccination coverage, with rates frequently ranging between 70% and 85%. The focus on this demographic was driven by their increased vulnerability compared to younger adults, as well as their role in maintaining workforce stability and caring for older family members. The success in vaccinating these age groups has been a key factor in easing the burden on healthcare systems.
Among younger adults, aged 18 to 49, vaccination rates tend to be more variable. In many regions, this group was eligible for vaccination later in the rollout process, and uptake has been influenced by factors such as vaccine hesitancy, accessibility, and perceptions of personal risk. On average, vaccination rates in this age group range from 60% to 80%, depending on the country and local public health efforts. Targeted campaigns addressing misinformation and improving access have been crucial in boosting vaccination numbers among younger adults.
For adolescents and children, aged 12 to 17, and more recently, those aged 5 to 11, vaccination efforts are still ongoing. Initially, vaccines were not authorized for these age groups, but approvals have since been granted in many countries. Vaccination rates here are generally lower, often between 30% and 60%, as rollout efforts are newer and parental consent is required. Schools and pediatric healthcare providers have played a vital role in facilitating access and educating families about the benefits of vaccination for children.
Understanding the age group distribution of vaccinated individuals is essential for public health planning. It highlights successes in protecting the most vulnerable populations while identifying areas where additional efforts are needed. Disparities in vaccination rates across age groups can inform targeted interventions, such as mobile clinics, community outreach, and tailored communication strategies. By addressing these gaps, countries can move closer to achieving herd immunity and mitigating the impact of the pandemic on all segments of the population.
J&J Vaccine: Still Relevant?
You may want to see also
Explore related products




$9.99 $9.99


![]()
Vaccine hesitancy and refusal statistics
Vaccine hesitancy and refusal have become significant factors influencing global vaccination rates, with statistics revealing varying degrees of acceptance across different populations. According to the World Health Organization (WHO), vaccine hesitancy is among the top threats to global health, complicating efforts to achieve herd immunity and control preventable diseases. Recent data indicates that while many countries have successfully vaccinated a substantial portion of their populations, hesitancy and refusal persist, particularly in specific demographic and geographic groups. For instance, in the United States, as of 2023, approximately 68% of the population has received at least one dose of a COVID-19 vaccine, but surveys show that around 15-20% of adults remain unvaccinated due to hesitancy or refusal.
In Europe, vaccine hesitancy varies widely between countries. Nations like Portugal and Denmark report vaccination rates above 90%, while others, such as Bulgaria and Romania, struggle with rates below 50%. Studies suggest that hesitancy in these regions is often linked to misinformation, distrust in government or healthcare systems, and cultural beliefs. For example, a 2022 survey by the European Commission found that 27% of respondents across the EU expressed doubts about vaccine safety, with higher rates in Eastern European countries. This disparity highlights the need for targeted public health campaigns to address specific concerns in these populations.
Globally, low- and middle-income countries face unique challenges with vaccine hesitancy and refusal. In some African nations, vaccination rates for diseases like measles and polio remain below the WHO’s recommended threshold of 95% due to logistical barriers, misinformation, and historical mistrust stemming from unethical medical practices. For instance, in Nigeria, only about 57% of children are fully vaccinated against preventable diseases, with hesitancy driven by rumors and religious beliefs. Conversely, countries like Rwanda have achieved high vaccination rates through robust community engagement and education, demonstrating the effectiveness of tailored strategies.
Demographic factors also play a crucial role in vaccine hesitancy and refusal statistics. Younger adults, particularly those aged 18-29, are more likely to express hesitancy compared to older age groups. Additionally, political affiliation, educational level, and socioeconomic status significantly influence vaccination decisions. In the U.S., for example, unvaccinated adults are more likely to identify with conservative political views and have lower levels of formal education. Addressing these disparities requires culturally sensitive communication strategies and building trust within underserved communities.
Finally, the rise of social media has amplified vaccine hesitancy by spreading misinformation and conspiracy theories. A 2021 study published in *Nature* found that up to 60% of COVID-19-related content on platforms like Facebook and Twitter contained false or misleading information. This digital landscape complicates efforts to disseminate accurate health information, making it essential for governments and health organizations to collaborate with tech companies to combat misinformation. By understanding these statistics and their underlying causes, policymakers can design more effective interventions to increase vaccine uptake and protect public health.
MMR Vaccine and Autism: Separating Facts from Fiction
You may want to see also
Explore related products





![]()
Booster dose uptake percentages worldwide
As of the latest data available, the uptake of booster doses worldwide varies significantly across regions and countries, reflecting differences in vaccine availability, public health policies, and population willingness. Globally, approximately 40-50% of the eligible population has received at least one booster dose, though this figure is heavily skewed by high-income nations. For instance, countries like Canada, Denmark, and Singapore report booster uptake rates exceeding 70% among their eligible populations, driven by robust vaccination campaigns and high public trust in health systems. In contrast, many low- and middle-income countries (LMICs) struggle with booster coverage, often below 20%, due to limited vaccine supply, logistical challenges, and lower prioritization of boosters compared to primary series completion.
In Europe, booster dose uptake has been relatively high, with an average of 55-60% of the population receiving an additional dose. Countries like Portugal and Spain lead with rates above 80%, while Eastern European nations like Bulgaria and Romania lag behind with rates below 30%. This disparity is partly attributed to vaccine hesitancy and socioeconomic factors. The European Union’s digital COVID certificate system has also incentivized booster uptake by linking vaccination status to travel and social activities.
In North America, the United States reports a booster uptake of approximately 50% among its eligible population, though this varies widely by state and demographic group. Older adults and high-risk individuals are more likely to have received boosters, while younger populations show lower uptake. Canada, on the other hand, has achieved a higher rate of 65-70%, supported by strong public health messaging and accessible vaccination sites. Both countries have faced challenges in maintaining momentum as the urgency of the pandemic has waned.
In Asia, booster uptake is highly variable. High-income nations like Japan and South Korea have administered boosters to 60-70% of their populations, while LMICs such as India and Indonesia report rates of 30-40%. China, despite its zero-COVID policy, has seen booster uptake plateau at around 50%, partly due to public skepticism and the perceived lower risk of severe disease with domestic vaccine brands. Regional disparities within countries also highlight the impact of urban-rural divides on vaccine accessibility.
In Africa and parts of the Middle East, booster uptake remains critically low, with fewer than 10-15% of eligible individuals receiving additional doses in most countries. This is largely due to limited vaccine supply, weak health infrastructure, and competing public health priorities such as malaria and HIV. Initiatives like COVAX have aimed to address these gaps, but progress has been slow. South Africa stands as an exception, with booster coverage around 25%, driven by targeted campaigns and lessons learned from previous waves.
To improve global booster uptake, international collaboration, equitable vaccine distribution, and localized public health strategies are essential. Addressing hesitancy, improving access, and prioritizing at-risk populations will be key to closing the gap in booster coverage worldwide.
Elderly Vaccination Rates: Are Seniors Staying Up-to-Date on Shots?
You may want to see also
Explore related products




![]()
Vaccination disparities in urban vs. rural areas
Vaccination disparities between urban and rural areas have become a significant concern in the global effort to achieve widespread immunization against diseases like COVID-19. Urban areas, with their higher population densities and better access to healthcare infrastructure, often report higher vaccination rates compared to rural regions. For instance, in the United States, urban counties have consistently shown vaccination rates 10-15% higher than rural counties, according to data from the Centers for Disease Control and Prevention (CDC). This gap is largely attributed to the concentration of vaccination sites, hospitals, and clinics in cities, making it easier for urban residents to access vaccines.
In contrast, rural areas face numerous challenges that contribute to lower vaccination rates. One major issue is the lack of healthcare facilities and professionals in these regions. Rural communities often have fewer hospitals, clinics, and pharmacies, which limits the availability of vaccination services. Additionally, transportation barriers play a critical role, as many rural residents live far from vaccination sites and may lack reliable access to vehicles or public transit. These logistical hurdles disproportionately affect elderly individuals and low-income populations, who are already at higher risk from vaccine-preventable diseases.
Another factor exacerbating vaccination disparities is the digital divide. Urban residents generally have better access to the internet and digital tools, making it easier for them to schedule vaccine appointments and access information about vaccine availability. In rural areas, limited internet connectivity and lower digital literacy rates hinder residents' ability to navigate online registration systems. This has led to situations where rural populations are left behind in vaccination campaigns, even when vaccines are available in sufficient quantities at the national level.
Socioeconomic and cultural factors also contribute to the urban-rural vaccination gap. Rural communities often have higher rates of poverty, lower educational attainment, and greater reliance on industries like agriculture, which may not prioritize vaccination due to work demands. Moreover, vaccine hesitancy tends to be higher in rural areas, driven by misinformation, distrust of government or medical institutions, and cultural beliefs. Addressing these disparities requires tailored strategies, such as mobile vaccination clinics, community outreach programs, and localized public health messaging to build trust and improve access.
To bridge the vaccination gap, policymakers and health organizations must adopt targeted approaches that account for the unique challenges of rural areas. This includes increasing funding for rural healthcare infrastructure, deploying mobile vaccination units to remote locations, and partnering with local leaders and organizations to disseminate accurate information. Incentives for healthcare providers to work in rural areas and initiatives to improve digital access can also play a crucial role. By addressing these disparities, we can ensure that vaccination efforts are equitable and effective across all regions, regardless of geographic location.
US Childhood Vaccination Rates: How Many Kids Are Fully Protected?
You may want to see also
Frequently asked questions
The percentage is typically calculated by dividing the number of fully vaccinated individuals by the total population and multiplying by 100.
It usually refers to fully vaccinated individuals, but some reports may include partially vaccinated people, so it’s important to check the specific definition used.
The frequency varies by country or region, but many health authorities update vaccination data daily or weekly to reflect the latest numbers.
Differences arise due to varying vaccine availability, distribution strategies, public acceptance, and population size across countries.