The dosage of anti-rabies vaccine for humans is a critical aspect of post-exposure prophylaxis, which is administered to prevent rabies infection after potential exposure to the virus. The volume of the vaccine typically ranges from 0.5 to 1.0 ml per dose, depending on the specific vaccine formulation and the manufacturer's guidelines. For instance, the intramuscular administration of vaccines like Verorab or Rabipur usually involves a 1.0 ml dose, while the intradermal route may require smaller volumes, such as 0.1 ml per site. The total number of doses and the schedule of administration, however, depend on factors like the individual's vaccination history, the severity of the exposure, and the recommendations of health authorities, such as the World Health Organization (WHO) or the Centers for Disease Control and Prevention (CDC). It is essential to consult a healthcare professional for accurate dosing and administration instructions to ensure effective protection against rabies.
Explore related products






What You'll Learn
- Standard Adult Dose: 1 mL per dose, typically administered intramuscularly in the deltoid area
- Pediatric Dosage: Children receive the same 1 mL dose as adults, regardless of age or weight
- Vaccine Schedule: 5 doses over 28 days: days 0, 3, 7, 14, and 28
- Intramuscular vs. Intradermal: 1 mL intramuscularly or 0.1 mL intradermally per dose for adults
- Booster Shots: 1 mL booster given 1 year after initial series for high-risk individuals
![]()
Standard Adult Dose: 1 mL per dose, typically administered intramuscularly in the deltoid area
The standard adult dose for the anti-rabies vaccine is a critical component of post-exposure prophylaxis (PEP) following potential rabies exposure. According to widely accepted guidelines, the dose is 1 mL per injection, typically administered intramuscularly (IM) into the deltoid muscle of the upper arm. This route ensures optimal absorption and immune response while minimizing discomfort. The deltoid area is preferred for adults due to its accessibility and the presence of well-developed muscle tissue, which facilitates proper vaccine delivery. It is essential to avoid administering the vaccine into the gluteal (buttock) muscle, as this can lead to reduced immunogenicity due to the higher fat content in that area.
The 1 mL dose is standardized across various rabies vaccines, including those manufactured by different pharmaceutical companies. This consistency ensures that healthcare providers can confidently administer the vaccine without confusion regarding volume. The intramuscular administration is crucial because rabies vaccines are inactivated and require direct delivery into muscle tissue to stimulate an effective immune response. Subcutaneous or intravenous administration is not recommended, as it may compromise the vaccine's efficacy and increase the risk of adverse reactions.
For the initial PEP regimen, the 1 mL dose is administered as part of a series of injections. The standard protocol involves administering the vaccine on days 0, 3, 7, 14, and 28 following exposure. Each dose is 1 mL, and all injections are given intramuscularly in the deltoid area. This schedule is designed to rapidly induce protective antibody levels in the body, neutralizing the rabies virus before it can cause infection. Adherence to this dosing and administration protocol is vital for ensuring the vaccine's effectiveness.
Healthcare providers must be trained in proper intramuscular injection techniques to administer the 1 mL dose correctly. The deltoid muscle is located in the lateral aspect of the upper arm, and the injection site should be cleaned with an antiseptic solution before administration. The needle should be inserted at a 90-degree angle to the skin surface, ensuring it penetrates the muscle tissue. After injection, gentle pressure can be applied to the site if bleeding occurs, but massaging the area is discouraged, as it may affect vaccine absorption.
In summary, the standard adult dose of the anti-rabies vaccine is 1 mL per dose, administered intramuscularly in the deltoid area. This dosing and administration method is universally accepted and ensures maximum vaccine efficacy while minimizing risks. Strict adherence to the recommended volume, route, and injection site is essential for successful post-exposure prophylaxis and prevention of rabies, a nearly always fatal disease if untreated.
Polio Vaccine: Egg-Free or Not?
You may want to see also
Explore related products





![]()
Pediatric Dosage: Children receive the same 1 mL dose as adults, regardless of age or weight
When it comes to administering the anti-rabies vaccine to children, it is crucial to understand that pediatric dosage guidelines specify that children receive the same 1 mL dose as adults, regardless of age or weight. This standardization ensures consistency in protection across all age groups. The rationale behind this dosing is rooted in the vaccine's formulation, which is designed to elicit an adequate immune response in both children and adults with a single milliliter dose. Parents and caregivers should be reassured that this dosage is safe and effective for children, as it has been rigorously tested and approved by health authorities.
The uniformity of the 1 mL dose simplifies the vaccination process for healthcare providers, eliminating the need for complex calculations based on a child's age or weight. This is particularly important in emergency situations, such as post-exposure prophylaxis after a suspected rabid animal bite, where quick and accurate administration is critical. By adhering to the pediatric dosage guideline of 1 mL, medical professionals can ensure that children receive the full protective benefits of the vaccine without delay. It is essential to follow the recommended schedule, which typically involves multiple doses over several weeks, to achieve optimal immunity.
One common concern among parents is whether a child’s smaller body size necessitates a reduced dose. However, studies have confirmed that the 1 mL dose is appropriate for children, as the vaccine's antigen content is sufficient to stimulate the immune system effectively, regardless of the recipient's size. This approach aligns with global vaccination standards, ensuring that children are not under-vaccinated and remain protected against rabies. Healthcare providers should educate parents about this aspect to alleviate any apprehensions and encourage timely vaccination.
In cases of rabies exposure, the 1 mL dose for children is administered as part of a comprehensive treatment protocol, which may include wound cleaning, passive immunization with rabies immunoglobulin, and the vaccine series. The consistency in dosage across age groups streamlines this process, allowing healthcare teams to focus on other critical aspects of care. It is imperative to emphasize that delaying or altering the dose can compromise the vaccine's effectiveness, making strict adherence to the 1 mL pediatric dosage non-negotiable.
Finally, while the 1 mL dose is standard for children, the location of vaccine administration differs between age groups. For children, the vaccine is typically injected into the deltoid muscle (upper arm), whereas infants may receive it in the thigh muscle. This distinction ensures optimal absorption and minimizes discomfort. Regardless of the injection site, the pediatric dosage remains 1 mL, reinforcing the principle that children and adults receive the same volume for maximum protection against rabies.
Nome's Diphtheria Vaccine Survival: The Science Behind Its Freeze Resistance
You may want to see also
Explore related products






![]()
Vaccine Schedule: 5 doses over 28 days: days 0, 3, 7, 14, and 28
The standard vaccine schedule for post-exposure prophylaxis against rabies in humans typically involves administering 5 doses of the anti-rabies vaccine over a 28-day period. This regimen is designed to ensure the body produces an adequate immune response to neutralize the rabies virus before it can cause disease. The schedule is as follows: Day 0, 3, 7, 14, and 28. Each dose is crucial and must be administered at the specified intervals to maximize effectiveness. The volume of each dose is typically 1 mL for most rabies vaccines used in humans, such as Verorab, Rabipur, or RabAvert. This standardized dosage ensures consistency in protection across different individuals.
On Day 0, the first dose of the vaccine is administered as soon as possible after exposure to the rabid animal. This initial dose is critical in stimulating the immune system to begin producing antibodies. Alongside the vaccine, rabies immunoglobulin (if available) is also given to provide immediate passive immunity, especially if the exposure is severe. The immunoglobulin is administered at a dose of 20 IU/kg body weight, but it does not replace the need for the vaccine. The vaccine is given into the deltoid muscle (for adults) or the anterolateral thigh muscle (for children), while the immunoglobulin is injected at a different site to avoid interference.
The second dose is administered on Day 3, followed by the third dose on Day 7. These early doses are essential to build upon the initial immune response and ensure the body continues to produce antibodies against the rabies virus. It is important not to delay these doses, as the timing is critical for the vaccine's efficacy. Each dose remains 1 mL and is given intramuscularly, following the same injection site guidelines as the first dose.
The fourth dose is given on Day 14, further reinforcing the immune response. By this stage, the body should have begun producing a significant number of antibodies, but the additional dose ensures sustained immunity. The final dose is administered on Day 28, completing the vaccination series. This last dose is vital for long-term immunity and ensures the individual remains protected against rabies. Again, each dose is 1 mL and follows the same administration protocol.
Adhering strictly to the 5-dose schedule over 28 days is essential for the vaccine to be effective. Missing or delaying doses can compromise immunity, leaving the individual vulnerable to rabies. Healthcare providers must educate patients about the importance of completing the full course and ensure follow-up appointments are kept. While the vaccine is generally safe, mild side effects such as pain at the injection site, headache, or fever may occur. These are typically manageable and do not interfere with the completion of the schedule. In summary, the 1 mL dose per injection, administered on days 0, 3, 7, 14, and 28, is the cornerstone of rabies prevention in humans.
Coronavirus Vaccine: Can It Stop Virus Transmission?
You may want to see also
Explore related products





![]()
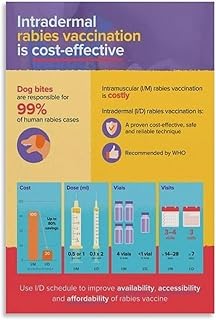
Intramuscular vs. Intradermal: 1 mL intramuscularly or 0.1 mL intradermally per dose for adults
When administering the anti-rabies vaccine to humans, the dosage and route of administration are critical factors that determine the vaccine's efficacy and safety. The two primary methods of administration are intramuscular (IM) and intradermal (ID), each with specific dosage requirements. For adults, the recommended volume is 1 mL intramuscularly or 0.1 mL intradermally per dose. This distinction is essential because it affects the vaccine's delivery, immune response, and potential side effects. The intramuscular route involves injecting the full dose directly into the muscle, typically in the deltoid or thigh, ensuring rapid absorption and a robust immune response. In contrast, the intradermal route delivers a smaller volume just beneath the skin's surface, utilizing the skin's immune-rich environment to stimulate a similar response with less antigen.
The intramuscular approach is the more conventional and widely used method for rabies vaccination. Administering 1 mL of the vaccine into the muscle ensures that the antigen is quickly distributed into the bloodstream, triggering a strong systemic immune response. This method is preferred for its reliability and ease of administration, especially in emergency post-exposure prophylaxis (PEP) scenarios. However, it may cause more localized pain, swelling, or discomfort at the injection site compared to the intradermal route. Healthcare providers must ensure proper needle placement to avoid subcutaneous administration, which could reduce vaccine efficacy.
On the other hand, the intradermal approach involves injecting 0.1 mL of the vaccine into the dermis, the layer of skin just below the epidermis. This method leverages the skin's dense network of antigen-presenting cells to elicit an immune response comparable to the intramuscular route but with a significantly smaller dose. The intradermal method is particularly useful in resource-limited settings where vaccine supply is constrained, as it reduces antigen usage by 90%. However, it requires skilled administration to ensure the vaccine is deposited correctly in the dermis, as improper technique can lead to reduced efficacy. Additionally, the intradermal route may cause less pain and fewer adverse reactions at the injection site.
Choosing between intramuscular and intradermal administration depends on several factors, including vaccine availability, patient characteristics, and healthcare setting. The World Health Organization (WHO) has endorsed both methods, with the intradermal route being a cost-effective alternative in mass vaccination campaigns or areas with limited vaccine supply. However, the intramuscular route remains the standard for individual post-exposure treatment due to its simplicity and proven effectiveness. Regardless of the route, adherence to the correct dosage (1 mL IM or 0.1 mL ID) is crucial to ensure adequate protection against rabies.
In summary, the anti-rabies vaccine for adults can be administered either intramuscularly (1 mL) or intradermally (0.1 mL), each with distinct advantages and considerations. The intramuscular route is straightforward and highly effective, while the intradermal route conserves vaccine and minimizes side effects but requires precise technique. Healthcare providers must weigh these factors to determine the most appropriate method for each patient, ensuring optimal protection against this deadly disease. Always refer to local guidelines and WHO recommendations for specific vaccination protocols.
Rand Paul: A Doctor's Paradoxical Stance on Vaccinations Explored
You may want to see also
Explore related products





![]()
Booster Shots: 1 mL booster given 1 year after initial series for high-risk individuals
For individuals at high risk of rabies exposure, such as veterinarians, animal handlers, or those living in regions with a high prevalence of rabies, a booster shot is a critical component of ongoing protection. The recommended protocol involves administering a 1 mL booster dose of the anti-rabies vaccine one year after the completion of the initial vaccine series. This booster is designed to reinforce the immune response and ensure continued immunity against the rabies virus. High-risk individuals should strictly adhere to this schedule, as delays or omissions can compromise their protection.
The 1 mL dose for the booster shot is consistent across most anti-rabies vaccines approved for human use, including those manufactured by major pharmaceutical companies. This standardized dosage ensures efficacy while minimizing the risk of adverse reactions. It is important to note that the booster should be administered intramuscularly, typically in the deltoid muscle for adults and the anterolateral thigh for children. Healthcare providers must follow proper injection techniques to ensure the vaccine’s effectiveness and patient comfort.
High-risk individuals should consult their healthcare provider to confirm their eligibility for the booster shot and to schedule the appointment accordingly. The timing of the booster—one year after the initial series—is crucial, as it aligns with the natural waning of immunity over time. Failure to receive the booster within this timeframe may necessitate a full vaccine series restart, depending on the individual’s risk level and exposure history. Therefore, maintaining a vaccination record and setting reminders can be helpful.
After receiving the 1 mL booster, individuals may experience mild side effects similar to those of the initial series, such as pain at the injection site, headache, or fatigue. These symptoms are generally transient and resolve within a few days. Serious adverse reactions are rare but should be reported to a healthcare provider immediately. It is also essential to monitor for any signs of allergic reaction, such as difficulty breathing or swelling, although these are extremely uncommon.
In summary, the 1 mL booster shot given one year after the initial anti-rabies vaccine series is a vital measure for high-risk individuals to maintain immunity against rabies. Adhering to this schedule, ensuring proper administration, and staying informed about potential side effects are key steps in safeguarding health. High-risk individuals should prioritize this booster as part of their ongoing preventive care strategy.
Pregnant in Europe? Vaccines You Need to Know About
You may want to see also
Frequently asked questions
The standard dose of anti-rabies vaccine for adults is 1 ml per injection, usually given intramuscularly in the deltoid muscle.
Children receive the same dose as adults, which is 1 ml per injection, regardless of age or weight.
No, the volume remains the same—1 ml per dose—for both the initial vaccination and any subsequent booster doses.
No, the standard volume of 1 ml per dose is consistent across different brands and manufacturers of anti-rabies vaccines. Always follow the specific product guidelines and healthcare provider instructions.