Malaria remains a significant global health challenge, particularly in tropical and subtropical regions, with millions of cases reported annually. The development of effective vaccines has been a long-standing goal in the fight against this mosquito-borne disease. As of recent advancements, there are currently only a few malaria vaccines approved or in advanced stages of development. The most notable is RTS,S/AS01 (Mosquirix), the first and only malaria vaccine to receive regulatory approval by the World Health Organization (WHO) in 2021, primarily for use in young children in sub-Saharan Africa. Additionally, R21/Matrix-M, developed by the University of Oxford, has shown promising results in clinical trials and is awaiting broader regulatory approval. Other candidates, such as PfSPZ, are in various stages of testing. Despite these advancements, the limited number of available vaccines underscores the ongoing need for continued research and innovation to combat malaria effectively.
Explore related products





What You'll Learn
- Approved Malaria Vaccines: Overview of currently approved vaccines and their development timelines
- Pipeline Candidates: Emerging vaccines in clinical trials and their progress
- Regional Availability: Distribution and accessibility of vaccines across different countries
- Efficacy Comparison: Analysis of effectiveness rates among existing and developing vaccines
- Challenges in Development: Key obstacles in creating and deploying malaria vaccines globally
![]()
Approved Malaria Vaccines: Overview of currently approved vaccines and their development timelines
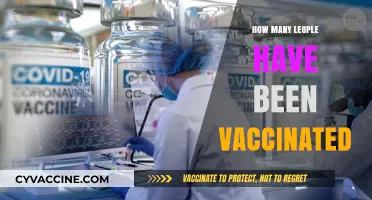
As of recent data, there are only a handful of malaria vaccines that have progressed through clinical trials and received regulatory approval, despite decades of research and development. Among these, RTS,S/AS01 (Mosquirix) stands out as the first and, for a long time, the only malaria vaccine to gain approval from the World Health Organization (WHO) in 2021. Developed by GSK in partnership with the PATH Malaria Vaccine Initiative, RTS,S targets the *Plasmodium falciparum* parasite, the deadliest malaria-causing pathogen. Its approval followed a pilot implementation program in Ghana, Kenya, and Malawi, where it demonstrated a 30% reduction in severe malaria cases among children aged 5–17 months, who receive a four-dose regimen starting at 5 months of age.
Another breakthrough came in 2023 with the approval of R21/Matrix-M, developed by the University of Oxford and manufactured by the Serum Institute of India. This vaccine has shown higher efficacy rates, approximately 77% in clinical trials, and is administered in a three-dose series for children aged 5–36 months, with a booster dose recommended after 12 months. Its approval was expedited due to its potential to address the limitations of RTS,S, particularly in regions with high malaria burden. The vaccine’s lower cost and scalability make it a promising tool in global malaria control efforts.
Comparing these two vaccines reveals distinct development timelines and strategies. RTS,S took over 30 years to move from concept to approval, reflecting the complexity of malaria vaccine development. In contrast, R21/Matrix-M progressed through trials and gained approval in less than a decade, benefiting from advancements in vaccine technology and lessons learned from RTS,S. Both vaccines, however, underscore the challenges of targeting a parasite with a complex life cycle and high genetic diversity.
Practical implementation of these vaccines requires careful consideration of local epidemiology, healthcare infrastructure, and community acceptance. For instance, RTS,S is recommended in areas with moderate to high *P. falciparum* transmission, while R21/Matrix-M’s broader efficacy may make it suitable for a wider range of settings. Healthcare providers must adhere to strict dosage schedules and monitor for rare side effects, such as fever or irritability, which are typically mild and resolve within days.
In conclusion, the approval of RTS,S and R21/Matrix-M marks a significant milestone in the fight against malaria, offering hope for millions at risk. However, their success hinges on equitable distribution, sustained funding, and integration into existing malaria control programs. As research continues, these vaccines serve as a foundation for future innovations, bringing the goal of malaria eradication closer to reality.
Bordetella in Puppy Vaccines: Common or Optional Protection?
You may want to see also
Explore related products






![]()
Pipeline Candidates: Emerging vaccines in clinical trials and their progress
As of recent data, there is only one malaria vaccine, RTS,S/AS01 (brand name Mosquirix), approved for use by the World Health Organization (WHO). However, the landscape of malaria vaccine development is dynamic, with several pipeline candidates in various stages of clinical trials. These emerging vaccines aim to address limitations of RTS,S, such as its moderate efficacy (around 30-40% in preventing clinical malaria) and the need for a four-dose regimen. Below, we explore key candidates, their mechanisms, and progress, offering a snapshot of the future of malaria prevention.
One promising candidate is R21/Matrix-M, developed by the University of Oxford and Serum Institute of India. In a Phase IIb trial involving 450 children in Burkina Faso, R21 demonstrated 77% efficacy over 12 months with a three-dose regimen, significantly outperforming RTS,S. Its adjuvant, Matrix-M, enhances immune response by stimulating both antibody and cellular immunity. Phase III trials are underway, with results expected in 2024. If approved, R21 could become a game-changer due to its higher efficacy and potentially lower cost, making it accessible to high-burden regions in sub-Saharan Africa.
Another notable candidate is PfSPZ Vaccine, developed by Sanaria. Unlike subunit vaccines like RTS,S and R21, PfSPZ is a whole-parasite vaccine composed of radiation-attenuated *Plasmodium falciparum* sporozoites. In a Phase II trial, it showed 48% efficacy over 18 months in Mali, with protection correlating to high antibody titers. However, its complex manufacturing process and the need for intravenous administration pose challenges. Ongoing trials are exploring intramuscular delivery and combination with other vaccines to improve feasibility and efficacy.
MK-2166 (VLA1553), developed by Valneva and Pfizer, is a subunit vaccine targeting the *P. falciparum* circumsporozoite protein. In a Phase I trial, it induced robust antibody responses after a three-dose regimen, with no serious adverse events. Its unique adjuvant, CP-870,893, enhances immunogenicity, potentially reducing the number of doses required. Phase II trials are ongoing, focusing on optimizing dosing schedules and evaluating efficacy in malaria-endemic populations.
Lastly, GMZ2, a transmission-blocking vaccine, takes a different approach by targeting gametocytes, the sexual stage of the parasite. In Phase I trials, GMZ2 induced antibodies that reduced parasite transmission in mosquitoes. While not designed to prevent infection in humans, it could complement other vaccines by interrupting disease spread. Its progress highlights the importance of multi-pronged strategies in malaria eradication efforts.
Practical considerations for these pipeline candidates include ensuring cold chain stability, especially for whole-parasite vaccines like PfSPZ, and addressing dosing logistics in resource-limited settings. Stakeholders must also prioritize affordability and equitable distribution to maximize impact. As these vaccines advance through clinical trials, their success could revolutionize malaria control, moving closer to the WHO’s goal of reducing global malaria cases by 90% by 2030.
Does the Rabies Vaccine Truly Prevent the Disease? Facts Revealed
You may want to see also
Explore related products






![]()
Regional Availability: Distribution and accessibility of vaccines across different countries
As of recent data, there is only one malaria vaccine approved for widespread use: RTS,S/AS01, commercially known as Mosquirix. Developed by GSK in partnership with the PATH Malaria Vaccine Initiative, it has been piloted in Ghana, Kenya, and Malawi since 2019, targeting children aged 5 months to 2 years. This vaccine requires a four-dose regimen, with the fourth dose administered 18 months after the third, offering modest efficacy of approximately 30% against severe malaria. Despite its limitations, RTS,S represents a breakthrough in malaria prevention, particularly in high-burden regions.
The distribution of RTS,S is heavily concentrated in sub-Saharan Africa, where malaria accounts for over 90% of global cases and deaths. The World Health Organization (WHO) has prioritized this region due to its disproportionate disease burden, with countries like Ghana, Kenya, and Malawi serving as pilot implementation sites. However, accessibility remains a challenge. Supply chain constraints, cold storage requirements, and the need for multiple doses complicate rollout, particularly in rural or resource-limited areas. For instance, maintaining the vaccine’s efficacy requires a consistent cold chain at 2–8°C, a logistical hurdle in regions with unreliable electricity.
In contrast, regions with lower malaria prevalence, such as Southeast Asia and Latin America, have limited access to RTS,S. While these areas also face malaria transmission, the disease burden is lower, and control strategies often rely on insecticide-treated nets, indoor residual spraying, and antimalarial drugs. The vaccine’s rollout in these regions is not a priority, as global health organizations focus resources on the highest-burden areas. This disparity highlights the challenge of balancing global health equity with practical implementation constraints.
Efforts to expand vaccine accessibility are underway, with Gavi, the Vaccine Alliance, playing a pivotal role in financing and distribution. In October 2023, Gavi approved funding to support the introduction of RTS,S in eligible countries, aiming to reach millions of children by 2025. However, this initiative faces competition for resources, as countries must also address other health priorities like COVID-19 vaccination and routine immunizations. Practical tips for improving accessibility include integrating malaria vaccination into existing child health programs, such as routine immunization clinics, to streamline delivery and reduce costs.
Looking ahead, the regional availability of malaria vaccines will likely expand with the development of new candidates. For example, the R21/Matrix-M vaccine, developed by the University of Oxford and Serum Institute of India, demonstrated 77% efficacy in phase II trials and is awaiting WHO prequalification. If approved, its lower cost and potentially simpler distribution requirements could make it a game-changer for broader accessibility. Until then, targeted distribution of RTS,S in high-burden areas remains the cornerstone of malaria vaccine strategy, underscoring the need for continued investment in infrastructure and health systems to ensure equitable access.
Kiwi Vaccination Rates: Tracking New Zealand's COVID-19 Immunization Progress
You may want to see also
Explore related products






![]()
Efficacy Comparison: Analysis of effectiveness rates among existing and developing vaccines
As of recent data, there are only a handful of malaria vaccines in existence, with the most prominent being RTS,S/AS01 (brand name Mosquirix) and the more recent R21/Matrix-M. The limited number of available vaccines underscores the complexity of developing effective immunization against the Plasmodium parasite, which causes malaria. Efficacy rates among these vaccines vary significantly, influenced by factors such as dosage regimens, target age groups, and the specific strains of the parasite they aim to combat.
Analyzing the efficacy of RTS,S/AS01, the first malaria vaccine to receive regulatory approval, reveals a modest effectiveness rate of approximately 36% in preventing clinical malaria in children aged 5–17 months over a 4-year period. This vaccine requires a 4-dose schedule, with the fourth dose administered 18 months after the third. While its efficacy is lower than many other vaccines for infectious diseases, it still represents a significant milestone in malaria prevention, particularly in high-burden regions. For instance, in pilot implementation programs in Ghana, Kenya, and Malawi, RTS,S/AS01 prevented approximately 1 in 3 cases of clinical malaria and 1 in 5 cases of severe malaria, highlighting its real-world impact despite its limitations.
In contrast, the R21/Matrix-M vaccine, developed by the University of Oxford, has demonstrated higher efficacy rates in phase IIb trials, reaching up to 77% in children aged 5–17 months after a 3-dose regimen. This vaccine’s improved performance is attributed to its novel adjuvant system, which enhances the immune response. However, it is important to note that R21/Matrix-M is still in the late stages of development and has not yet received widespread regulatory approval. Its higher efficacy rate positions it as a promising candidate for broader use, particularly if it can maintain these results in larger, phase III trials and real-world settings.
Comparing these vaccines, the difference in efficacy rates raises questions about their optimal use in different populations and regions. For instance, RTS,S/AS01 may be more suitable for immediate deployment in areas with high malaria transmission, given its existing approval and established safety profile, despite its lower efficacy. Conversely, R21/Matrix-M could be prioritized for regions where higher efficacy is critical, such as areas with emerging drug resistance or lower transmission rates. Practical considerations, such as the number of doses required and the logistical challenges of administering them, also play a crucial role in determining which vaccine is most appropriate for a given context.
For healthcare providers and policymakers, understanding these efficacy differences is essential for making informed decisions. For example, in regions with limited healthcare infrastructure, a vaccine with fewer required doses, like R21/Matrix-M, may be more feasible. Additionally, combining vaccines with other preventive measures, such as insecticide-treated bed nets and antimalarial drugs, can maximize their impact. As new vaccines continue to emerge, ongoing monitoring and comparative studies will be vital to ensure that the most effective tools are deployed where they are needed most.
Vaccines and Transmission: Do They Reduce Spread of Diseases?
You may want to see also
Explore related products






![]()
Challenges in Development: Key obstacles in creating and deploying malaria vaccines globally
As of recent data, there is only one malaria vaccine approved for widespread use: RTS,S/AS01, also known as Mosquirix. This vaccine, developed by GSK in partnership with the PATH Malaria Vaccine Initiative, received a green light from the World Health Organization (WHO) in 2021 for children in sub-Saharan Africa and other regions with moderate to high P. falciparum malaria transmission. Its approval marked a historic milestone, yet it is just the beginning of a complex journey. The limited number of available vaccines underscores the immense challenges in their development and deployment, which range from biological complexities to logistical hurdles.
One of the most significant obstacles in creating malaria vaccines is the parasite’s biological sophistication. Unlike viruses or bacteria, *Plasmodium falciparum*—the deadliest malaria parasite—has a complex life cycle involving multiple stages and forms. This makes it difficult to identify a single, effective target for vaccination. For instance, RTS,S targets the parasite’s circumsporozoite protein during the pre-erythrocytic stage, but its efficacy wanes over time, requiring a four-dose regimen for children aged 5–17 months. Even then, it provides only partial protection, reducing severe malaria cases by about 30%. Developing a vaccine that targets multiple life stages or induces long-lasting immunity remains a daunting scientific challenge.
Deployment of malaria vaccines is equally fraught with difficulties, particularly in resource-limited settings. Cold chain requirements, for example, pose a critical barrier. RTS,S must be stored between 2°C and 8°C, a logistical nightmare in regions with unreliable electricity or inadequate infrastructure. Additionally, the vaccine’s multi-dose schedule demands robust healthcare systems to ensure timely administration. In rural areas of sub-Saharan Africa, where malaria is most prevalent, reaching eligible children often requires mobile clinics or community health workers, adding layers of complexity and cost.
Another challenge lies in affordability and accessibility. While Gavi, the Vaccine Alliance, has committed to funding RTS,S, the vaccine’s price remains a concern for cash-strapped governments. Moreover, the global health community must compete for attention and resources in regions burdened by multiple diseases. For instance, in 2022, only 1.3 million children received the first dose of RTS,S, a fraction of the estimated 25 million annual births in malaria-endemic areas. Scaling up vaccination programs while ensuring equitable access requires sustained political will, innovative financing, and global collaboration.
Despite these challenges, ongoing research offers hope. The R21/Matrix-M vaccine, developed by the University of Oxford and Serum Institute of India, demonstrated 77% efficacy in phase IIb trials and is awaiting WHO approval. Its lower cost and potential for easier distribution could revolutionize malaria prevention. However, even with promising candidates, the path from lab to field is fraught with regulatory, manufacturing, and cultural hurdles. Public acceptance, for instance, is critical; misinformation or mistrust can derail vaccination efforts, as seen in other public health campaigns. Addressing these challenges requires not just scientific innovation but also community engagement, education, and tailored strategies that respect local contexts.
Smallpox Vaccine: A Historic Triumph in Eradicating a Deadly Disease
You may want to see also
Frequently asked questions
As of now, there is one malaria vaccine approved for widespread use: RTS,S (brand name Mosquirix).
Yes, several other malaria vaccine candidates are in clinical trials, including R21/Matrix-M, which has shown promising results in recent studies.
Developing a malaria vaccine is challenging due to the complexity of the parasite's life cycle and its ability to evade the immune system.
No, RTS,S provides moderate protection, reducing malaria cases by about 30-40% in young children, who are the primary target group.
It is likely, as ongoing research and clinical trials aim to develop more effective and widely applicable vaccines against malaria.