The question of how many human vaccines exist is a complex one, as the number can vary depending on how vaccines are categorized and counted. Broadly, there are over 100 licensed vaccines available globally, targeting a wide range of infectious diseases. These vaccines can be grouped into several categories, including routine childhood immunizations, travel vaccines, and those recommended for specific populations or conditions. Routine childhood vaccines, such as measles, mumps, rubella (MMR), diphtheria, tetanus, and pertussis (DTaP), are widely recognized and administered, while others, like the Ebola vaccine or certain types of influenza vaccines, are used more selectively based on geographic location, age, or health status. Additionally, new vaccines are continually being developed and approved, further expanding the list of available immunizations. Understanding the full scope of human vaccines requires considering both the diversity of diseases they prevent and the varying needs of different populations around the world.
Explore related products






What You'll Learn
- Vaccine Types Overview: Categorizing vaccines by disease prevention, technology, and administration methods
- Global Vaccine Count: Estimating total human vaccines available worldwide, including regional variations
- Historical Vaccine Development: Tracing the timeline of vaccine creation from early to modern innovations
- Vaccine Approval Process: Understanding regulatory steps for vaccine validation and public distribution
- Emerging Vaccine Technologies: Exploring advancements like mRNA, viral vectors, and personalized vaccines
![]()
Vaccine Types Overview: Categorizing vaccines by disease prevention, technology, and administration methods
As of recent data, there are over 100 human vaccines approved for use worldwide, targeting a wide range of infectious diseases. However, understanding vaccines goes beyond mere numbers. Categorizing them by disease prevention, technology, and administration methods provides a clearer picture of their diversity and application. This classification not only highlights their unique characteristics but also aids in their development, distribution, and effective use.
Disease Prevention Categories: Targeted Immunity
Vaccines are primarily categorized by the diseases they prevent, ranging from common illnesses like influenza to life-threatening conditions such as measles or COVID-19. For instance, conjugate vaccines, like the pneumococcal conjugate vaccine (PCV13), protect against bacterial infections by linking a weak antigen to a strong one, enhancing immune response. In contrast, live-attenuated vaccines, such as the MMR (measles, mumps, rubella) vaccine, use weakened pathogens to stimulate long-term immunity, typically requiring 2 doses spaced 4–8 weeks apart for children over 12 months. Understanding these categories helps healthcare providers tailor vaccination schedules to specific age groups, such as administering the Tdap vaccine (tetanus, diphtheria, pertussis) to adolescents and pregnant women to ensure continued protection.
Technological Innovations: From Traditional to Cutting-Edge
Vaccine technology has evolved significantly, with each method offering distinct advantages. Inactivated vaccines, like the injectable polio vaccine (IPV), use killed pathogens and are safer for immunocompromised individuals but often require multiple doses (e.g., 3–4 doses starting at 2 months of age). Meanwhile, mRNA vaccines, exemplified by Pfizer-BioNTech and Moderna’s COVID-19 vaccines, represent a breakthrough by delivering genetic instructions for cells to produce viral proteins, eliciting a robust immune response. These vaccines typically require 2 doses, 3–4 weeks apart, with boosters recommended every 6–12 months for sustained protection. Such technological diversity ensures adaptability to emerging pathogens and varying population needs.
Administration Methods: Beyond the Needle
While intramuscular injections (e.g., flu shots) are common, vaccines are administered via diverse routes. Oral vaccines, like the rotavirus vaccine (Rotarix), offer convenience and are particularly effective in low-resource settings, requiring 2–3 doses starting at 6 weeks of age. Nasal sprays, such as the live-attenuated influenza vaccine (FluMist), provide needle-free alternatives, though they are contraindicated for individuals with weakened immune systems. Even transdermal patches are being explored, potentially revolutionizing vaccine delivery by eliminating needles altogether. Choosing the right administration method depends on factors like patient age, immune status, and the vaccine’s stability.
Practical Takeaways: Maximizing Vaccine Efficacy
Understanding vaccine categories empowers individuals and healthcare providers to make informed decisions. For example, knowing that subunit vaccines, like the hepatitis B vaccine, contain only specific pathogen fragments makes them ideal for those with allergies to traditional vaccine components. Similarly, recognizing that viral vector vaccines, such as Johnson & Johnson’s COVID-19 vaccine, use harmless viruses to deliver genetic material can address hesitancy by explaining their safety profile. Always follow dosage schedules (e.g., 0, 1, 6-month intervals for hepatitis B) and storage guidelines (e.g., mRNA vaccines require ultra-cold storage) to ensure efficacy. By categorizing vaccines, we not only appreciate their complexity but also optimize their use in safeguarding global health.
Fetal Tissue in Vaccines: Ethical Concerns and the Right to Life
You may want to see also
Explore related products






![]()
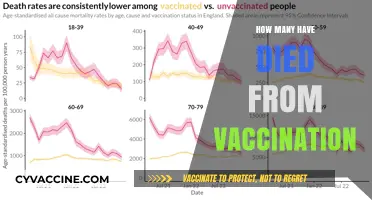
Global Vaccine Count: Estimating total human vaccines available worldwide, including regional variations
The global vaccine landscape is a complex mosaic, with over 100 distinct human vaccines licensed for use across various regions. However, estimating the total number of vaccines available worldwide is not merely about counting individual products. It involves understanding regional variations in vaccine accessibility, regulatory approvals, and public health priorities. For instance, while high-income countries may have access to the latest mRNA vaccines for COVID-19, low-income regions often rely on more traditional vaccines like the oral polio vaccine or the measles-mumps-rubella (MMR) combination. This disparity highlights the need for a nuanced approach to estimating the global vaccine count.
To accurately estimate the total number of human vaccines available, one must consider the role of regulatory bodies such as the World Health Organization (WHO), the U.S. Food and Drug Administration (FDA), and the European Medicines Agency (EMA). These organizations approve vaccines based on safety, efficacy, and regional health needs. For example, the WHO’s prequalification program ensures vaccines meet international standards, particularly for distribution in low-resource settings. In contrast, the FDA’s approval process focuses on vaccines tailored to the U.S. population, such as the annual influenza vaccine, which is updated to target specific strains circulating in North America. This regional specificity means that the global vaccine count is not uniform but rather a sum of localized vaccine portfolios.
A practical approach to estimating the global vaccine count involves categorizing vaccines by disease type, target population, and administration schedule. For instance, childhood immunization schedules in Africa often include vaccines for tuberculosis (BCG), diphtheria-tetanus-pertussis (DTP), and yellow fever, while schedules in Europe may prioritize rotavirus and pneumococcal vaccines. Additionally, some vaccines require multiple doses, such as the three-dose hepatitis B series or the two-dose HPV vaccine for adolescents. By accounting for these variations, one can build a more comprehensive estimate of the total vaccines available worldwide, recognizing that the count is not just a number but a reflection of global health equity.
Regional variations in vaccine availability also stem from economic and logistical factors. High-income countries often have robust cold chain infrastructure, enabling the distribution of temperature-sensitive vaccines like the Pfizer-BioNTech COVID-19 vaccine, which requires storage at -70°C. In contrast, low-income regions may rely on heat-stable vaccines, such as the MenAfriVac meningitis vaccine, designed specifically for use in the “meningitis belt” of sub-Saharan Africa. These adaptations underscore the importance of tailoring vaccine development and distribution to regional needs, further complicating a straightforward global vaccine count.
Ultimately, estimating the total number of human vaccines available worldwide requires a multifaceted analysis that accounts for regional regulatory approvals, disease prevalence, and logistical capabilities. While a precise count may remain elusive due to these complexities, the effort to quantify global vaccine availability serves as a critical tool for identifying gaps in access and guiding future public health initiatives. By focusing on both the number and distribution of vaccines, stakeholders can work toward a more equitable global immunization landscape, ensuring that life-saving vaccines reach those who need them most.
Koch's Contribution: Did He Develop the Rabies Vaccine?
You may want to see also
Explore related products






![]()
Historical Vaccine Development: Tracing the timeline of vaccine creation from early to modern innovations
The journey of vaccine development is a testament to human ingenuity and our relentless battle against infectious diseases. From rudimentary beginnings to cutting-edge biotechnology, the timeline of vaccine creation reflects both scientific evolution and societal necessity. Early efforts, such as Edward Jenner’s 1796 smallpox vaccine, laid the foundation by introducing the concept of using a milder pathogen to induce immunity. This breakthrough, though simple by today’s standards, revolutionized disease prevention and set the stage for future innovations.
By the late 19th and early 20th centuries, vaccine development accelerated with the advent of germ theory and improved laboratory techniques. Louis Pasteur’s rabies vaccine in 1885 and the diphtheria antitoxin in the 1890s demonstrated the power of targeted immunization. These vaccines were not just scientific achievements but lifesaving tools, reducing mortality rates dramatically. For instance, the diphtheria vaccine, often administered as part of the DTaP (diphtheria, tetanus, pertussis) shot for children under 7 years old, remains a cornerstone of pediatric immunization schedules, with doses given at 2, 4, 6, and 15–18 months, followed by boosters at 4–6 years.
The mid-20th century marked a golden age of vaccine development, driven by global health crises and technological advancements. Jonas Salk’s inactivated polio vaccine in 1955 and Albert Sabin’s oral polio vaccine in 1961 eradicated a disease that once paralyzed millions. Similarly, the measles vaccine, introduced in 1963, transformed a common childhood illness into a preventable condition. Today, the MMR (measles, mumps, rubella) vaccine is administered in two doses, typically at 12–15 months and 4–6 years, offering lifelong immunity to most recipients.
Modern vaccine innovations, particularly in the 21st century, showcase the fusion of biotechnology and immunology. The development of mRNA vaccines, such as Pfizer-BioNTech and Moderna’s COVID-19 vaccines, represents a paradigm shift. These vaccines, authorized for individuals aged 5 and older, deliver genetic instructions to cells, prompting them to produce a harmless protein that triggers an immune response. This technology not only expedited the response to a global pandemic but also holds promise for tackling other diseases, including HIV and cancer.
Tracing the timeline of vaccine creation reveals a clear pattern: each innovation builds on the last, driven by the dual forces of scientific curiosity and public health need. From Jenner’s cowpox inoculation to mRNA platforms, vaccines have evolved from empirical discoveries to precision tools. Understanding this history not only highlights the progress made but also underscores the ongoing challenges, such as vaccine hesitancy and equitable distribution. As we look to the future, the lessons of the past remind us that vaccines are not just medical interventions—they are a shared legacy of human resilience.
Military Vaccine Requirements: Understanding Mandatory Immunizations for Service Members
You may want to see also
Explore related products






![]()
Vaccine Approval Process: Understanding regulatory steps for vaccine validation and public distribution
As of recent data, there are over 100 human vaccines licensed for use worldwide, targeting a range of diseases from measles and polio to COVID-19 and influenza. Each of these vaccines has undergone a rigorous approval process to ensure safety, efficacy, and quality before reaching the public. Understanding this regulatory journey is crucial for appreciating the science and safeguards behind every dose administered.
The vaccine approval process begins with preclinical testing, where potential vaccines are studied in laboratories and animal models to assess their safety and immune response. This phase is critical for identifying any red flags before human trials commence. For example, the COVID-19 mRNA vaccines underwent extensive preclinical studies to confirm their ability to trigger antibody production without causing harm. Once preclinical data is promising, developers submit an Investigational New Drug (IND) application to regulatory bodies like the FDA or EMA, detailing the vaccine’s composition, manufacturing process, and proposed clinical trial design.
Next comes clinical trials, a three-phase process that evaluates the vaccine in humans. Phase 1 trials involve small groups (20–100 volunteers) to test safety, dosage, and immune response. Phase 2 expands to several hundred participants to further assess safety and efficacy, often including specific demographics like children or the elderly. Phase 3 trials involve thousands of participants and are designed to confirm efficacy, monitor side effects, and compare the vaccine to a placebo or existing vaccine. For instance, the Pfizer-BioNTech COVID-19 vaccine’s Phase 3 trial included over 43,000 participants, demonstrating 95% efficacy in preventing symptomatic infection. Throughout these phases, independent Data Safety Monitoring Boards (DSMBs) oversee the trials to ensure participant safety and data integrity.
After successful clinical trials, manufacturers submit a Biologics License Application (BLA) or Marketing Authorization Application (MAA) to regulatory agencies. This submission includes all data from preclinical and clinical studies, manufacturing details, and proposed labeling. Regulators then conduct a thorough review, often consulting external advisory committees. For example, the FDA’s Vaccines and Related Biological Products Advisory Committee (VRBPAC) publicly reviews vaccine data before approval. Emergency Use Authorization (EUA) may be granted during public health crises, as seen with COVID-19 vaccines, but this still requires robust evidence of safety and efficacy.
Finally, post-approval surveillance ensures ongoing safety and effectiveness. Programs like the CDC’s Vaccine Adverse Event Reporting System (VAERS) and the Vaccine Safety Datalink (VSD) monitor for rare side effects that may not have appeared in clinical trials. Manufacturers are also required to conduct Phase 4 studies, gathering additional long-term data. Practical tips for the public include reporting any adverse reactions to healthcare providers and staying informed about vaccine updates through trusted sources like the WHO or CDC. This multi-layered process ensures that every vaccine, from childhood immunizations to pandemic responses, meets the highest standards before distribution.
Who Needs Rabies Vaccination: Essential Guidelines for At-Risk Individuals
You may want to see also
Explore related products






![]()
Emerging Vaccine Technologies: Exploring advancements like mRNA, viral vectors, and personalized vaccines
As of recent estimates, there are over 100 human vaccines licensed for use worldwide, targeting a range of infectious diseases from measles and polio to COVID-19 and influenza. However, the landscape of vaccine development is rapidly evolving, driven by groundbreaking technologies that promise greater efficacy, speed, and personalization. Among these, mRNA, viral vectors, and personalized vaccines stand out as transformative advancements reshaping the future of immunization.
Consider mRNA vaccines, which gained global prominence during the COVID-19 pandemic. Unlike traditional vaccines that use weakened or inactivated pathogens, mRNA vaccines deliver genetic instructions to cells, prompting them to produce a harmless protein that triggers an immune response. This technology allows for rapid development—the COVID-19 mRNA vaccines were created in record time—and offers potential applications for diseases like HIV, malaria, and cancer. For instance, a typical mRNA vaccine dose contains 30 micrograms of mRNA, administered in two shots spaced 3–4 weeks apart for adults. The key advantage lies in its adaptability: mRNA sequences can be quickly modified to target new variants or entirely different pathogens, making it a versatile tool in the fight against emerging diseases.
Viral vector vaccines, another innovative approach, use a harmless virus (the vector) to deliver genetic material into cells, similar to mRNA vaccines but with a different delivery mechanism. The Johnson & Johnson COVID-19 vaccine, for example, employs an adenovirus vector and requires just a single 0.5 mL dose for individuals aged 18 and older. This technology has shown promise in combating diseases like Ebola and is being explored for HIV and tuberculosis. However, one caution is the potential for pre-existing immunity to the vector virus, which can reduce vaccine efficacy. To mitigate this, researchers are engineering novel vectors and optimizing dosing strategies to ensure robust immune responses.
Personalized vaccines represent the frontier of vaccine technology, tailoring immunizations to individual genetic profiles, immune histories, or specific disease risks. For instance, neoantigen-based cancer vaccines identify unique mutations in a patient’s tumor and create a customized vaccine to target those cells. While still in early stages, this approach has shown promise in clinical trials, with some patients experiencing prolonged remission. Practical implementation, however, requires advancements in genomic sequencing and bioinformatics to identify suitable targets efficiently. For now, personalized vaccines remain a high-cost, specialized option, but their potential to revolutionize treatment for cancers and infectious diseases is undeniable.
In summary, emerging vaccine technologies like mRNA, viral vectors, and personalized vaccines are expanding the boundaries of what immunization can achieve. Each offers unique advantages—speed, adaptability, and precision—but also presents challenges that require careful navigation. As these technologies mature, they hold the potential to address not only existing diseases but also future threats, ensuring a more resilient global health landscape. For individuals, staying informed about these advancements and adhering to recommended dosing schedules will be key to maximizing their benefits.
Can We Develop a Vaccine to Prevent Gangrene?
You may want to see also
Frequently asked questions
There are over 100 licensed human vaccines available globally, targeting a wide range of diseases, though the exact number varies by region and availability.
In many countries, children receive around 14–16 different vaccines as part of routine immunization schedules, protecting against diseases like measles, polio, and whooping cough.
Adults may receive 5–10 vaccines depending on age, health, and travel needs, including flu, tetanus, shingles, and COVID-19 vaccines.
As of recent data, there are hundreds of vaccine candidates in development or clinical trials, targeting diseases like HIV, malaria, and emerging pathogens.