The Gardasil vaccine, primarily used to prevent human papillomavirus (HPV) infections and associated cancers, has been widely administered globally since its approval in 2006. As of recent data, hundreds of millions of doses have been distributed worldwide, with significant uptake in countries with robust vaccination programs. In the United States alone, over 120 million doses have been administered, primarily to adolescents and young adults. Global figures indicate that the vaccine has reached over 300 million individuals, reflecting its importance in public health efforts to reduce HPV-related diseases. However, vaccination rates vary widely by region, influenced by factors such as accessibility, awareness, and cultural attitudes toward HPV prevention. Understanding the scale of Gardasil administration is crucial for assessing its impact on public health and identifying gaps in coverage.
Explore related products






What You'll Learn
- Global Gardasil Vaccination Rates: Overview of worldwide HPV vaccine administration statistics and trends
- Age Group Vaccination Coverage: Breakdown of Gardasil doses by age, focusing on adolescents
- Gender-Based Vaccination Data: Comparison of male vs. female Gardasil vaccination rates globally
- Regional Vaccination Disparities: Analysis of Gardasil distribution differences across countries and continents
- Vaccination Trends Over Time: Yearly increase or decrease in Gardasil doses administered since its introduction
![]()
Global Gardasil Vaccination Rates: Overview of worldwide HPV vaccine administration statistics and trends
As of recent data, over 300 million doses of Gardasil, the HPV vaccine, have been administered globally since its introduction in 2006. This milestone underscores its widespread adoption as a critical tool in preventing human papillomavirus (HPV)-related cancers and diseases. However, vaccination rates vary dramatically across regions, influenced by factors such as healthcare infrastructure, policy support, and public awareness. High-income countries like Australia and the United States report coverage exceeding 70% among eligible adolescents, while many low-income nations struggle to reach 10% due to limited access and vaccine hesitancy.
Analyzing trends reveals a clear disparity between urban and rural areas, even within the same country. For instance, in India, urban vaccination rates for Gardasil are nearly double those in rural regions, highlighting the impact of accessibility and education. Age-specific data also shows that the vaccine is most commonly administered to adolescents aged 9–14, aligning with global health recommendations for optimal immune response. However, catch-up programs for older age groups remain underutilized, leaving a gap in protection for those who missed early vaccination.
Persuasively, the success of Gardasil vaccination programs hinges on policy frameworks that prioritize affordability and accessibility. Countries like Rwanda and Australia have demonstrated that school-based vaccination drives and public funding can dramatically increase uptake. Conversely, nations reliant on out-of-pocket payments or lacking structured health education campaigns often see stagnant or declining rates. Practical tips for improving global coverage include integrating HPV vaccination into routine immunization schedules, leveraging community health workers to dispel myths, and subsidizing costs in low-resource settings.
Comparatively, the HPV vaccine’s global rollout mirrors challenges seen in other immunization campaigns, such as those for measles or COVID-19. However, Gardasil’s unique focus on cancer prevention offers a compelling case for sustained investment. For example, Australia’s near-elimination of cervical cancer among vaccinated cohorts serves as a powerful testament to its efficacy. Yet, replicating this success globally requires addressing logistical hurdles, such as cold chain storage in tropical climates, and cultural barriers, like misconceptions linking the vaccine to promiscuity.
Descriptively, the landscape of Gardasil vaccination is a patchwork of progress and stagnation. In Latin America, countries like Brazil and Mexico have made strides through regional partnerships and public campaigns, while Central American nations lag due to political instability and resource constraints. Similarly, Africa’s uptake remains low, though pilot programs in countries like Botswana show promise. Europe presents a mixed picture, with Nordic countries achieving high coverage through robust healthcare systems, while Eastern Europe faces skepticism and funding shortfalls.
In conclusion, while Gardasil has reached hundreds of millions, its full potential remains untapped. Bridging the gap requires tailored strategies that address local barriers, from cost to cultural beliefs. By learning from successful models and adapting them to diverse contexts, the global community can move closer to the WHO’s goal of eliminating cervical cancer—a vision where HPV vaccination is not a privilege but a universal right.
Strangles Vaccination Schedule: How Often Should Horses Be Vaccinated?
You may want to see also
Explore related products

![]()
Age Group Vaccination Coverage: Breakdown of Gardasil doses by age, focusing on adolescents
Adolescents aged 11 to 12 are the primary target for Gardasil vaccination, yet coverage rates reveal a concerning gap. According to the CDC, only 54% of adolescents in this age group have received at least one dose of the HPV vaccine as of 2022. This falls short of the Healthy People 2030 goal of 80% coverage. The recommended regimen is two doses, administered 6 to 12 months apart, for those who start the series before their 15th birthday. Despite its proven efficacy in preventing HPV-related cancers, uptake remains uneven, influenced by factors like parental awareness, healthcare access, and regional disparities.
Breaking down the data further, coverage increases incrementally with age but plateaus prematurely. By age 17, only 68% of adolescents have completed the series, leaving a significant portion vulnerable during their most at-risk years. Boys lag slightly behind girls, with 50% versus 58% initiating the series by age 13. This gender gap persists, though it narrows by late adolescence. Catch-up vaccination for those aged 15 to 26 requires three doses, complicating adherence and highlighting the importance of early initiation.
Practical strategies to improve adolescent coverage include school-based vaccination programs, which have shown success in states like Rhode Island, where HPV vaccination rates exceed 90%. Pediatricians play a critical role by recommending the vaccine as routinely as Tdap or meningococcal vaccines. Addressing parental hesitancy through education about HPV’s link to six types of cancer can also boost acceptance. Additionally, leveraging technology, such as text message reminders for follow-up doses, has proven effective in some populations.
Comparatively, countries with robust vaccination infrastructure, like Australia and the UK, achieve higher adolescent coverage through national immunization programs integrated into school systems. The U.S. could emulate these models by standardizing HPV vaccination as a school entry requirement, where legally feasible. Until then, targeted interventions in underserved communities, such as mobile clinics and reduced-cost vaccines, are essential to bridge the gap. The goal is clear: ensure adolescents receive Gardasil before sexual debut, maximizing its preventive potential.
Why the NHS Doesn't Offer the Chickenpox Vaccine: Explained
You may want to see also
![]()
Gender-Based Vaccination Data: Comparison of male vs. female Gardasil vaccination rates globally
Global Gardasil vaccination rates reveal a striking gender disparity, with females consistently outpacing males in uptake. This trend is rooted in the vaccine's initial marketing as a cervical cancer preventive, primarily targeting adolescent girls. Data from the World Health Organization (WHO) indicates that in countries with established HPV vaccination programs, female coverage often exceeds 70%, while male coverage hovers around 20-40%. For instance, in Australia, where the vaccine is offered free to both genders, 78.6% of eligible females have received at least one dose compared to 68.5% of males, despite equal access.
This gap persists despite growing evidence that HPV vaccination benefits both genders equally. HPV causes cancers of the penis, anus, and oropharynx in males, yet public health messaging has been slower to emphasize these risks. In the United States, the CDC recommends Gardasil for all adolescents aged 11-12, with catch-up doses up to age 26. However, only 54% of males aged 17 have initiated the series, versus 72% of females, according to 2022 data. Cost, cultural stigma, and provider bias contribute to this divide, as healthcare providers are less likely to recommend HPV vaccination to boys during routine visits.
To address this imbalance, countries like Sweden and Canada have implemented gender-neutral vaccination programs, offering Gardasil to all adolescents regardless of sex. Sweden’s program, launched in 2012, achieved over 80% coverage in both males and females by 2020, demonstrating the effectiveness of inclusive policies. Practical steps for improving male uptake include integrating HPV vaccination into routine pediatric care, educating parents about gender-neutral benefits, and leveraging school-based immunization drives. For instance, a two-dose regimen (0, 6-12 months) is recommended for those starting the series before age 15, simplifying adherence.
Critics argue that prioritizing females was a necessary first step due to the higher burden of cervical cancer. However, this approach inadvertently reinforced gender stereotypes, framing HPV prevention as a "female issue." A comparative analysis of Australia and Japan highlights the impact of policy: Australia’s gender-neutral program has reduced HPV-related cancers in both sexes, while Japan’s female-focused approach has seen slower progress in male-specific cancers. This underscores the need for global health strategies to prioritize equity over expediency.
In conclusion, closing the gender gap in Gardasil vaccination requires targeted interventions and policy shifts. Public health campaigns must reframe HPV vaccination as a universal health measure, not a gendered intervention. Providers should proactively offer the vaccine to all eligible adolescents, regardless of sex, and address parental hesitancy with clear, evidence-based messaging. By doing so, we can maximize the vaccine’s potential to eliminate HPV-related cancers globally, ensuring no gender is left behind.
Are Allergy Shots Vaccines? Understanding Immunotherapy vs. Vaccination
You may want to see also
![]()
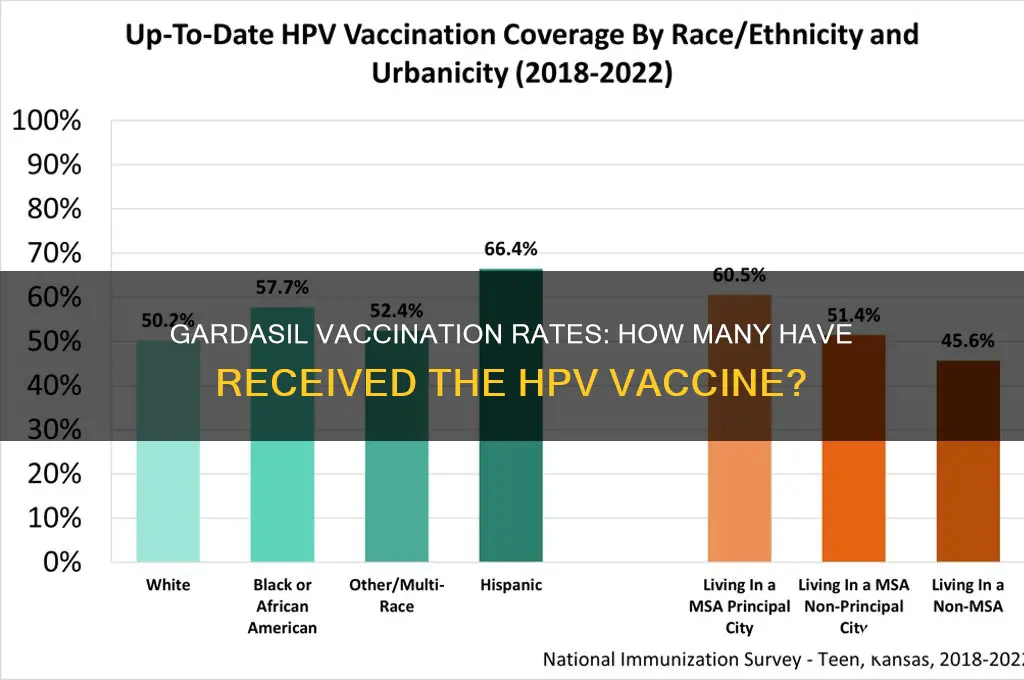
Regional Vaccination Disparities: Analysis of Gardasil distribution differences across countries and continents
The global distribution of Gardasil, a vaccine primarily targeting Human Papillomavirus (HPV), reveals stark disparities across regions, influenced by economic status, healthcare infrastructure, and policy priorities. High-income countries like the United States, Canada, and most of Western Europe have achieved widespread coverage, with over 70% of eligible adolescents receiving at least one dose. In contrast, low- and middle-income countries (LMICs) in Africa, Southeast Asia, and parts of Latin America report coverage rates below 20%, often due to limited access and affordability. For instance, while Australia boasts a 78% vaccination rate among 15-year-olds, Nigeria struggles with less than 5% coverage, highlighting the divide.
Analyzing these disparities requires examining both supply and demand factors. On the supply side, LMICs face challenges such as high vaccine costs, inadequate cold chain infrastructure, and limited healthcare worker training. Gardasil’s recommended three-dose regimen, priced at $120–$180 in high-income countries, becomes prohibitively expensive in regions where annual healthcare budgets are constrained. On the demand side, cultural misconceptions about HPV vaccination, particularly in conservative societies, contribute to hesitancy. For example, in India, rumors linking the vaccine to infertility have deterred uptake, despite its inclusion in some state immunization programs.
To address these disparities, targeted strategies are essential. For LMICs, leveraging Gavi, the Vaccine Alliance, can reduce costs through negotiated pricing and financial support. Single-dose regimens, now endorsed by the WHO as effective, offer a cost-effective alternative, reducing logistical burdens and increasing feasibility in resource-limited settings. Additionally, community-based education campaigns can combat misinformation, as seen in Rwanda’s successful HPV vaccination drive, which achieved 93% coverage through school-based programs and public awareness.
Comparatively, regional collaborations can amplify impact. The Pan American Health Organization’s (PAHO) revolving fund has enabled bulk purchasing for Latin American countries, lowering costs and ensuring steady supply. Such models could be replicated in other regions, particularly in Africa, where HPV-related cervical cancer rates are highest globally. Meanwhile, high-income countries must prioritize global equity by supporting technology transfers and waiving patents, as seen during the COVID-19 pandemic, to scale up local vaccine production.
In conclusion, bridging Gardasil distribution gaps demands a multifaceted approach—combining affordability, infrastructure, education, and collaboration. Without concerted global efforts, millions of adolescents, particularly in LMICs, will remain vulnerable to HPV-related diseases, perpetuating health inequities. The lessons from successful regional initiatives underscore the feasibility of progress, provided political will and resources align with need.
California's 1975 Mandatory Vaccines: A Historical Overview of Required Immunizations
You may want to see also
![]()
Vaccination Trends Over Time: Yearly increase or decrease in Gardasil doses administered since its introduction
Since its approval in 2006, Gardasil, the HPV vaccine, has seen fluctuating administration rates, reflecting shifting public health priorities, awareness campaigns, and evolving medical recommendations. Initial uptake was rapid, with over 1.5 million doses administered in the United States within the first year. This surge was driven by its promise to prevent cervical cancer and other HPV-related diseases, primarily targeting adolescent girls and young women aged 9 to 26. However, growth plateaued by 2010, as vaccine hesitancy, cost barriers, and limited public awareness tempered enthusiasm. Despite these challenges, annual doses have gradually increased over the past decade, reaching approximately 10 million globally in 2021, according to the World Health Organization.
Analyzing the data reveals distinct trends tied to policy changes and public health initiatives. For instance, the CDC’s 2011 recommendation to include boys and young men in vaccination efforts initially had a modest impact, with only a 5% increase in doses administered to males by 2013. However, by 2019, this figure had risen to 45%, signaling growing acceptance of HPV vaccination as a gender-neutral preventive measure. Similarly, the FDA’s 2018 approval of Gardasil 9 for adults aged 27 to 45 sparked a 20% increase in doses within this age group by 2020, though overall numbers remain lower compared to adolescents. These shifts underscore the importance of targeted campaigns and expanded eligibility in driving vaccination rates.
Persuasively, the case for sustained growth lies in addressing persistent barriers. Cost remains a significant hurdle, particularly in low-income regions, where vaccination rates are as low as 5% compared to 70% in high-income countries. School-based vaccination programs, as implemented in Australia and the UK, have proven effective, with completion rates exceeding 80%. Such initiatives, combined with public education campaigns debunking myths about vaccine safety, could further accelerate uptake. For parents and caregivers, practical steps include scheduling vaccinations during routine check-ups, leveraging reminders from healthcare providers, and exploring financial assistance programs like the Vaccines for Children (VFC) program in the U.S.
Comparatively, Gardasil’s trajectory contrasts with vaccines like measles or influenza, which often see sharp spikes during outbreaks. HPV vaccination, being preventive rather than reactive, relies on long-term behavioral changes and trust in medical science. While annual increases average 3-5% globally, this pales in comparison to the 20-30% growth rates seen in vaccines with immediate, visible impacts. However, the cumulative effect of steady HPV vaccination is profound: countries with high coverage, such as Australia, have reported a 90% reduction in genital warts and a 50% decline in cervical cancer precursors. This highlights the value of persistence in public health efforts, even when progress seems incremental.
Descriptively, the landscape of Gardasil administration is a patchwork of successes and gaps. In Rwanda, a nationwide campaign achieved 93% coverage among adolescent girls in 2011, a testament to what’s possible with political will and community engagement. Conversely, in the U.S., only 54% of adolescents were up to date on HPV vaccination as of 2022, despite widespread availability. Such disparities reflect broader challenges in healthcare access and health literacy. Moving forward, leveraging technology—such as SMS reminders or digital health records—could streamline vaccination processes, while partnerships with schools and workplaces could expand reach. The goal is clear: transform Gardasil from a sporadically administered vaccine to a universal safeguard against HPV-related diseases.
Post-Vaccine Soreness: Understanding How Long the Discomfort Typically Lasts
You may want to see also
Frequently asked questions
As of recent estimates, over 300 million doses of the Gardasil vaccine have been distributed globally since its approval in 2006.
According to the CDC, approximately 50-60% of adolescents aged 13-17 in the U.S. have received at least one dose of the Gardasil vaccine as of 2023.
Over 100 countries have incorporated the Gardasil vaccine into their national immunization schedules to prevent HPV-related diseases.
The standard regimen is 2 or 3 doses, depending on the age at which vaccination begins. Younger individuals (under 15) typically receive 2 doses, while older individuals receive 3 doses.