The topic of COVID-19 vaccine-related deaths has been a subject of significant public interest and scrutiny since the vaccines were first rolled out. While COVID-19 vaccines have proven to be highly effective in preventing severe illness, hospitalization, and death from the virus, rare instances of adverse events, including fatalities, have been reported. Health authorities, such as the Centers for Disease Control and Prevention (CDC) and the World Health Organization (WHO), continuously monitor vaccine safety through systems like the Vaccine Adverse Event Reporting System (VAERS) and the Vaccine Safety Datalink (VSD). Data from these systems indicate that serious side effects, including deaths, are extremely rare, with the benefits of vaccination far outweighing the risks. As of the latest reports, the number of deaths potentially linked to COVID-19 vaccines is minuscule compared to the billions of doses administered globally, underscoring the vaccines' overall safety profile.
Explore related products

$18.99 $18.99

$29.95 $25.48

$20.41 $29.99



What You'll Learn
- Reported Deaths Post-Vaccination: Tracking fatalities temporally linked to COVID-19 vaccine administration globally
- Vaccine Safety Studies: Research on rare adverse events, including mortality, from clinical trials
- Causality Assessment: Evaluating if reported deaths are directly caused by the vaccine
- Global Death Statistics: Comparing vaccine-related deaths to overall COVID-19 mortality rates
- Misinformation Impact: Analyzing false claims about vaccine-induced fatalities and their effects
![]()
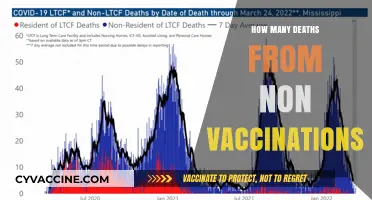
Reported Deaths Post-Vaccination: Tracking fatalities temporally linked to COVID-19 vaccine administration globally
The global rollout of COVID-19 vaccines has been accompanied by rigorous monitoring systems to track adverse events, including fatalities temporally linked to vaccination. As of recent data, the number of reported deaths post-vaccination remains extremely low relative to the billions of doses administered worldwide. For instance, the Vaccine Adverse Event Reporting System (VAERS) in the United States has documented fewer than 0.002% of vaccine recipients experiencing severe outcomes, with even fewer attributed directly to the vaccine. This underscores the vaccines' safety profile, though each report is scrutinized to ensure public trust and continuous improvement.
Analyzing these reports reveals a critical distinction: temporal association does not imply causation. Many post-vaccination fatalities occur due to underlying health conditions, coincidental events, or other factors unrelated to the vaccine. For example, in the elderly population (ages 65+), who received a significant portion of early doses, pre-existing conditions like cardiovascular disease or cancer often contribute to mortality. Health agencies emphasize that the risk of severe COVID-19 outcomes far outweighs the minimal risks associated with vaccination, particularly for vulnerable age groups.
To accurately track these events, global health organizations employ passive and active surveillance systems. Passive systems, like VAERS or the UK’s Yellow Card scheme, rely on voluntary reporting from healthcare providers and the public. Active systems, such as the CDC’s V-safe program, proactively monitor vaccinated individuals via smartphone-based health checks. These tools collectively ensure that any potential safety signals are identified promptly, allowing for rapid investigation and public communication. For individuals, understanding these systems can demystify how vaccine safety is maintained and why reported deaths are thoroughly vetted before drawing conclusions.
Comparatively, the fatality rate from COVID-19 itself dwarfs that of vaccine-related deaths. Studies show that the risk of death from COVID-19 is approximately 1 in 1,000 for unvaccinated individuals, whereas the risk of a fatal vaccine reaction is estimated at less than 1 in 1 million. This stark contrast highlights the vaccines' role in preventing far greater harm. For those hesitant due to safety concerns, consulting healthcare providers and reviewing data from trusted sources like the WHO or CDC can provide clarity and reassurance.
Practically, individuals can contribute to accurate tracking by reporting any adverse events post-vaccination, regardless of perceived severity. This includes symptoms like persistent headaches, chest pain, or unusual bruising, which could signal rare conditions like vaccine-induced immune thrombotic thrombocytopenia (VITT). Prompt reporting aids in identifying patterns and refining vaccine protocols, such as the adjusted dosing recommendations for younger age groups to minimize risks. Ultimately, transparency in tracking and reporting fatalities post-vaccination strengthens global vaccine confidence and ensures ongoing safety for all recipients.
Vaccine Mercury: Does It Accumulate in the Body?
You may want to see also
Explore related products


$20.41 $29.99




![]()
Vaccine Safety Studies: Research on rare adverse events, including mortality, from clinical trials
Clinical trials for COVID-19 vaccines rigorously monitored adverse events, including mortality, to ensure safety before regulatory approval. These trials, involving tens of thousands of participants across diverse age groups, systematically tracked outcomes after vaccination with precise dosages—typically 30 µg for mRNA vaccines like Pfizer-BioNTech and Moderna. Post-trial surveillance continued through Phase 4 studies and pharmacovigilance systems like VAERS and V-safe, capturing rare events that might not surface in smaller trials. For instance, the rare association between the Johnson & Johnson vaccine and thrombosis with thrombocytopenia syndrome (TTS) emerged only after millions of doses were administered, highlighting the importance of ongoing monitoring.
Analyzing mortality data from these trials requires distinguishing between vaccine-related deaths and coincidental fatalities in a global population under pandemic stress. Clinical trial results for Pfizer-BioNTech and Moderna showed no significant difference in mortality between vaccine and placebo groups, with deaths occurring at rates consistent with background mortality. For example, in Pfizer’s trial, 6 deaths occurred in the vaccine group (n=21,720) versus 4 in the placebo group (n=21,728), none attributed to the vaccine. Such findings underscore the challenge of attributing rare deaths to vaccination without robust causality assessment, a task handled by expert panels and regulatory bodies.
Instructively, vaccine safety studies employ active surveillance and risk-benefit frameworks to evaluate rare adverse events. Passive reporting systems, while valuable, often overestimate risks due to underreporting biases and lack of denominators. Active surveillance, such as the CDC’s V-safe program, proactively collects data from vaccine recipients via smartphone, enabling rapid detection of signals. For instance, V-safe’s monitoring of over 10 million doses identified no unexpected patterns of mortality, reinforcing trial findings. Practical tips for healthcare providers include reporting suspected adverse events promptly and counseling patients on the rarity of severe outcomes, using data-driven examples to build trust.
Comparatively, COVID-19 vaccine mortality risks pale against the risks of COVID-19 itself, particularly in vulnerable populations. Studies show that unvaccinated individuals face a 10- to 50-fold higher risk of death from COVID-19 than vaccinated individuals experience from rare vaccine-related events. For example, TTS occurred in approximately 7 per 1 million Johnson & Johnson vaccine recipients, while COVID-19 mortality rates in unvaccinated older adults exceeded 10% in some regions. This stark contrast emphasizes the critical role of vaccines in preventing far more deaths than they could ever cause, a key takeaway for public health messaging.
Descriptively, the process of identifying and investigating vaccine-related mortality involves multidisciplinary teams, including epidemiologists, clinicians, and statisticians. Case reviews examine medical histories, autopsy reports, and temporal relationships to establish causality. For instance, the investigation into TTS cases linked to adenoviral vector vaccines combined clinical data with laboratory findings to confirm the mechanism of platelet-activating antibodies. Such meticulous analysis ensures that rare events are understood and mitigated, as evidenced by the restriction of Johnson & Johnson’s vaccine to specific populations. This scientific rigor exemplifies how vaccine safety studies balance transparency with public health imperatives.
Unvaccinated Threats: Exploring Diseases Without Available Vaccines
You may want to see also
Explore related products






![]()
Causality Assessment: Evaluating if reported deaths are directly caused by the vaccine
Reports of deaths following COVID-19 vaccination have sparked public concern, but determining causality is complex. A causality assessment systematically evaluates whether a reported death is directly attributable to the vaccine or coincidental. This process involves analyzing temporal relationships, medical history, autopsy findings, and known vaccine side effects. For instance, if a death occurs within hours of vaccination, it might suggest anaphylaxis, a rare but severe allergic reaction. However, most reported deaths post-vaccination occur days or weeks later, making causality harder to establish. Understanding this process is crucial for distinguishing genuine vaccine-related fatalities from unrelated events.
The first step in causality assessment is establishing a clear timeline. Document the time between vaccination and death, as well as any symptoms reported in between. For example, the Pfizer and Moderna mRNA vaccines have a recommended dosage of 30 µg and 100 µg, respectively, and adverse events are more likely to occur within the first 48 hours. If a death occurs weeks later in an elderly individual with pre-existing conditions, such as cardiovascular disease, the vaccine may not be the primary cause. Age is a critical factor; individuals over 65 are more likely to experience coincidental health events due to comorbidities, making causality assessments in this group particularly challenging.
Next, consider the biological plausibility of the vaccine causing death. COVID-19 vaccines have known side effects, such as myocarditis (inflammation of the heart muscle), which is more common in young males after the second dose. However, fatal cases of vaccine-induced myocarditis are extremely rare, with estimates ranging from 1 to 2 cases per million vaccinations. Autopsy reports and toxicology tests can provide critical evidence. For example, if a deceased individual had no history of heart issues but showed signs of myocarditis post-vaccination, a causal link might be more plausible.
Comparative analysis is another essential tool. Compare the rate of deaths in vaccinated populations to baseline mortality rates in similar unvaccinated groups. If the death rate post-vaccination does not significantly exceed the expected rate, it suggests the vaccine is not a major contributor. For instance, a study in *The Lancet* found no increase in overall mortality among vaccinated individuals aged 16–64, reinforcing the safety profile of the vaccines. This comparative approach helps differentiate between correlation and causation.
Finally, transparency and communication are key. Public health agencies must clearly explain the causality assessment process to build trust. For example, the CDC and FDA use the Vaccine Adverse Event Reporting System (VAERS) to monitor reports, but emphasize that VAERS data alone cannot prove causality. Practical tips for the public include reporting any severe symptoms immediately and consulting healthcare providers for personalized advice. By understanding the rigor of causality assessments, individuals can make informed decisions and avoid misinformation.
NJ Teachers' Vaccine Phase: Where Do Educators Stand in Rollout?
You may want to see also
Explore related products






![]()
Global Death Statistics: Comparing vaccine-related deaths to overall COVID-19 mortality rates
The COVID-19 pandemic has prompted an unprecedented global vaccination campaign, with billions of doses administered worldwide. Amid this effort, concerns about vaccine safety, particularly regarding mortality, have surfaced. To address these concerns, it’s essential to compare vaccine-related deaths to overall COVID-19 mortality rates, using data from reputable sources like the World Health Organization (WHO), Centers for Disease Control and Prevention (CDC), and peer-reviewed studies. This comparison provides context and highlights the risk-benefit balance of vaccination.
Analyzing the Numbers: Vaccine-Related Deaths vs. COVID-19 Fatalities
Data from the CDC’s Vaccine Adverse Event Reporting System (VAERS) and the WHO’s Global Advisory Committee on Vaccine Safety show that vaccine-related deaths are extremely rare. For instance, as of late 2023, the CDC reported approximately 20 confirmed deaths linked to the Johnson & Johnson vaccine (out of 17 million doses) due to rare blood clots, and fewer than 100 deaths potentially associated with mRNA vaccines (Pfizer and Moderna) out of over 600 million doses administered in the U.S. In contrast, COVID-19 has caused over 6.5 million deaths globally, with a mortality rate of approximately 1% among unvaccinated populations, particularly in older age groups (65+ years) and those with comorbidities. This stark disparity underscores the vaccines’ safety profile relative to the virus’s lethality.
Practical Context: Risk Assessment for Different Age Groups
For individuals aged 65 and older, COVID-19 poses a mortality risk 50 times higher than any vaccine-related risk. For example, a 70-year-old unvaccinated individual has a 1 in 20 chance of dying if infected, compared to a 1 in 1 million risk of severe vaccine side effects. Even in younger populations, where COVID-19 mortality is lower (0.01% for those under 40), the vaccine remains significantly safer. Public health officials recommend completing the primary vaccine series (two doses of mRNA or one dose of J&J) and staying updated with boosters, especially for high-risk groups, to maximize protection.
Persuasive Argument: The Societal Impact of Vaccination
Beyond individual risks, vaccination reduces overall mortality by curbing viral transmission and preventing healthcare systems from being overwhelmed. Countries with high vaccination rates, such as Portugal (90% fully vaccinated) and Singapore (85%), have seen dramatic declines in COVID-19 deaths compared to nations with lower uptake. For instance, Portugal’s COVID-19 mortality rate dropped by 80% post-vaccination, while unvaccinated populations in low-income countries continue to face higher death rates. This evidence reinforces the vaccines’ role in saving lives on a global scale.
Takeaway: Informed Decision-Making with Data
While no medical intervention is entirely risk-free, the data unequivocally show that COVID-19 vaccines are far safer than the disease they prevent. Vaccine-related deaths are vanishingly rare, occurring at rates orders of magnitude lower than COVID-19 fatalities. By focusing on evidence-based comparisons, individuals and policymakers can make informed decisions that prioritize public health. Always consult healthcare providers for personalized advice, especially regarding dosage adjustments for immunocompromised individuals or those with specific medical histories.
Optimal Timing for West Nile Vaccination in Horses: A Guide
You may want to see also
Explore related products






![]()
Misinformation Impact: Analyzing false claims about vaccine-induced fatalities and their effects
Misinformation about COVID-19 vaccines has proliferated, with false claims of vaccine-induced fatalities being among the most damaging. A cursory search reveals alarming headlines and social media posts alleging thousands of deaths directly caused by the vaccines. However, these claims often lack credible sources, relying instead on anecdotal evidence or misinterpreted data from passive surveillance systems like the Vaccine Adverse Event Reporting System (VAERS). It’s critical to understand that VAERS is an open-access database where anyone can submit reports, unverified and unproven, making it a fertile ground for misinformation. Genuine vaccine safety monitoring involves rigorous analysis by health authorities, which consistently shows that serious adverse events, including deaths, are exceedingly rare.
To illustrate, consider the Pfizer-BioNTech and Moderna mRNA vaccines, administered in billions of doses globally. According to the Centers for Disease Control and Prevention (CDC), severe allergic reactions occur in approximately 2 to 5 cases per million doses. Fatalities directly linked to the vaccine are even rarer, with myocarditis (a heart inflammation condition) occurring primarily in adolescent males and young adults after the second dose, yet resulting in death in only a handful of cases worldwide. Contrast this with the risk of severe COVID-19, which has claimed over 6 million lives globally, and the protective benefits of vaccination become undeniable. Misinformation obscures this life-saving reality, sowing doubt where clarity is needed.
The impact of such false claims extends beyond individual hesitancy. In communities where misinformation spreads unchecked, vaccination rates plummet, leaving populations vulnerable to outbreaks. For instance, in regions with low vaccine uptake due to misinformation, hospitals have been overwhelmed with preventable cases, straining healthcare systems and increasing mortality rates. This ripple effect underscores the societal cost of disinformation. Public health campaigns must counter these narratives with transparent, data-driven communication, emphasizing the rigorous testing and ongoing monitoring of vaccines.
Practical steps can mitigate the spread of misinformation. First, verify sources: rely on reputable organizations like the World Health Organization (WHO), CDC, or peer-reviewed journals. Second, understand vaccine safety protocols: vaccines undergo Phase III trials involving tens of thousands of participants and are continuously monitored post-approval. Third, engage in constructive dialogue: when encountering misinformation, approach the conversation with empathy, focusing on shared concerns for health and safety. Finally, report false claims on social media platforms to limit their reach. By taking these actions, individuals can contribute to a more informed and resilient society.
In conclusion, false claims about vaccine-induced fatalities exploit fear and uncertainty, but their impact is far from inevitable. Armed with accurate information and critical thinking, individuals and communities can dismantle misinformation and uphold the life-saving potential of vaccines. The stakes are high, but so is our capacity to respond effectively.
Understanding Japanese Encephalitis Vaccine Risks: What You Need to Know
You may want to see also
Frequently asked questions
As of the latest data, the number of deaths directly attributed to COVID-19 vaccines is extremely low compared to the billions of doses administered. Reports of deaths are thoroughly investigated, and most are found to be unrelated or coincidental.
No, COVID-19 vaccines have saved millions of lives and are significantly safer than contracting the virus. The risk of severe illness or death from COVID-19 far outweighs the rare risks associated with vaccination.
The majority of reported deaths after vaccination are due to underlying health conditions or other causes, not the vaccine itself. Rare side effects like blood clots or myocarditis have been reported but are extremely uncommon.
The CDC uses systems like VAERS (Vaccine Adverse Event Reporting System) and V-safe to monitor and investigate reports of adverse events, including deaths, following vaccination. These systems help identify potential safety concerns.
Rare serious side effects, such as myocarditis, have been observed more frequently in younger males, particularly after the second dose of mRNA vaccines. However, the overall risk of death from these side effects is extremely low across all age groups.