When considering the administration of live vaccines such as MMR (measles, mumps, and rubella) and varicella (chickenpox), it is important to follow specific guidelines to ensure optimal immune response and safety. According to the Centers for Disease Control and Prevention (CDC) and the Advisory Committee on Immunization Practices (ACIP), if these live vaccines are not administered on the same day, they should be separated by at least 4 weeks (28 days). This interval is recommended because administering live vaccines too closely together may result in reduced effectiveness of one or both vaccines. However, if the vaccines are given less than 4 weeks apart, the dose administered second should be repeated, maintaining the appropriate interval to ensure proper immunity. This spacing is crucial for both routine immunization schedules and catch-up vaccinations.
| Characteristics | Values |
|---|---|
| Minimum Interval Between MMR and Varicella Vaccines | 28 days (if not administered simultaneously) |
| Simultaneous Administration | MMR and varicella vaccines can be given on the same day |
| Reason for Interval | Both are live attenuated vaccines; spacing reduces potential interference |
| Age Group Affected | Children and adults receiving both vaccines |
| Source of Guidelines | CDC (Centers for Disease Control and Prevention) |
| Revaccination if Interval Not Met | If given <28 days apart, the dose administered second should be repeated |
| Exceptions | No exceptions; interval applies to all recipients |
| Last Updated Guidelines | As of 2023 (based on latest CDC recommendations) |
Explore related products






What You'll Learn
![]()
Recommended Interval Between MMR and Varicella Vaccines
The recommended interval between administering the Measles, Mumps, and Rubella (MMR) vaccine and the Varicella (chickenpox) vaccine is an important consideration for healthcare providers and parents alike. According to the Centers for Disease Control and Prevention (CDC) and the World Health Organization (WHO), if these vaccines are not administered on the same day, a minimum interval of 4 weeks (28 days) should be observed between the two live attenuated vaccines. This guideline is based on the potential for interference between live vaccines, which could reduce their effectiveness if given too closely together.
The rationale behind this recommendation stems from the nature of live attenuated vaccines. Both the MMR and Varicella vaccines contain weakened forms of the viruses they protect against. When administered simultaneously, the immune response is robust and effective. However, if given too close together, the immune system might not mount an optimal response to one or both vaccines, potentially leading to suboptimal immunity. The 28-day interval ensures that the immune system has sufficient time to respond adequately to the first vaccine before being challenged by the second.
In situations where the MMR and Varicella vaccines are given on the same day, there is no need for concern about interference. This is a common practice, especially in childhood immunization schedules, as it reduces the number of visits required and ensures timely protection against these diseases. However, if they are not administered concurrently, adhering to the 4-week interval is crucial. If this interval is inadvertently shortened, the vaccine that was given second may need to be repeated to ensure full protection.
It is important to note that this interval applies specifically to live attenuated vaccines like MMR and Varicella. Other types of vaccines, such as inactivated or subunit vaccines, do not have the same interference concerns and can be administered at any time relative to live vaccines. Healthcare providers should carefully review a patient’s vaccination history to ensure compliance with these guidelines and make informed decisions about scheduling.
Parents and caregivers should communicate openly with healthcare providers about their child’s vaccination schedule to avoid errors. If there is uncertainty about the timing of previous vaccines, it is always best to consult immunization records or the healthcare provider who administered the vaccines. Adhering to the recommended interval between MMR and Varicella vaccines maximizes their effectiveness, providing strong protection against measles, mumps, rubella, and chickenpox.
Vaccines and Autism: Exploring the Link
You may want to see also
Explore related products






![]()
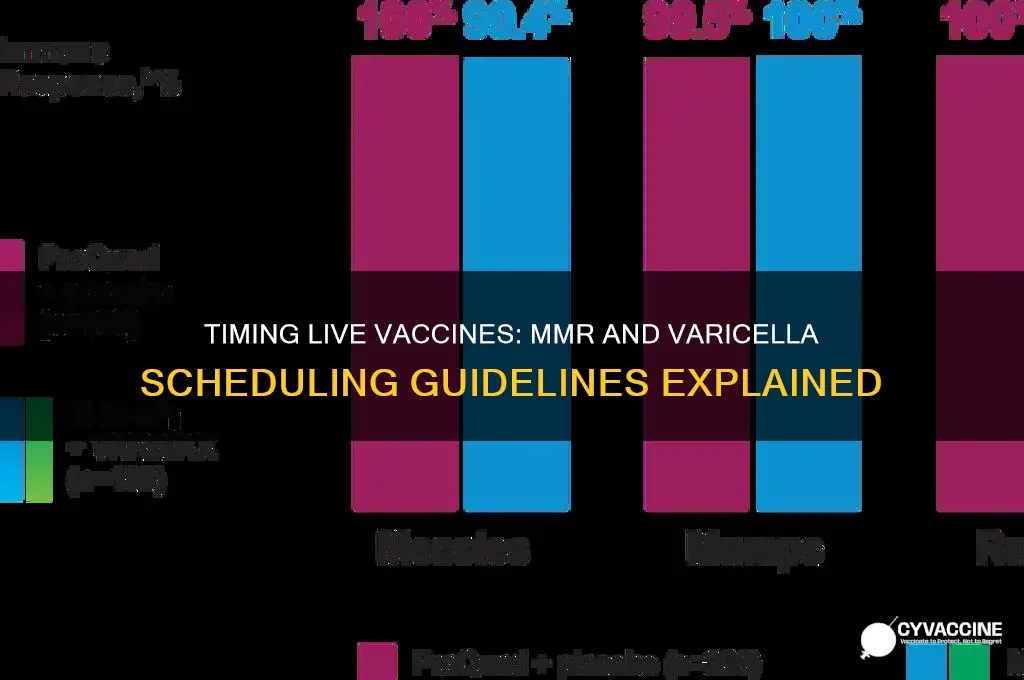
Immune Response and Vaccine Efficacy Timing
The timing between administering live vaccines, such as the Measles, Mumps, and Rubella (MMR) vaccine and the Varicella (chickenpox) vaccine, is crucial for optimizing immune response and vaccine efficacy. According to the Centers for Disease Control and Prevention (CDC), if these vaccines are not administered simultaneously, they should be given at least 28 days apart. This interval is based on the understanding of how the immune system responds to live attenuated vaccines. When a live vaccine is administered, it stimulates the immune system to produce antibodies and memory cells, which provide protection against the targeted disease. Administering another live vaccine too soon can potentially interfere with the immune response, leading to reduced efficacy of one or both vaccines.
The 28-day interval is rooted in the immune system's need to mount a robust response to the first vaccine before being challenged by another. Live vaccines mimic natural infection, albeit in a weakened form, and require time for the immune system to process and respond effectively. If the vaccines are given too close together, the immune system might not have sufficient time to develop a strong memory response to the first vaccine, potentially compromising its efficacy. This timing also minimizes the risk of vaccine-related adverse events, as the immune system is not overwhelmed by simultaneous responses to multiple live pathogens.
Immune response timing is particularly important for vaccines like MMR and Varicella, which are both live attenuated and target different but critical childhood diseases. The MMR vaccine provides protection against three viral diseases, while the Varicella vaccine prevents chickenpox. Both vaccines are highly effective when administered according to the recommended schedule. However, the immune system's ability to respond to these vaccines can be influenced by factors such as age, underlying health conditions, and previous exposure to the diseases. Adhering to the 28-day interval ensures that the immune system can focus on one vaccine at a time, maximizing the production of specific antibodies and memory cells for each disease.
Vaccine efficacy is also closely tied to the timing of administration. Studies have shown that administering live vaccines too close together can result in lower antibody titers and reduced protection. For example, if the Varicella vaccine is given less than 28 days after the MMR vaccine, the immune response to Varicella may be suboptimal. Conversely, if the MMR vaccine is given shortly after the Varicella vaccine, the efficacy of MMR could be compromised. This is why healthcare providers strictly follow the recommended intervals to ensure that each vaccine has the best chance of inducing a strong and lasting immune response.
In cases where both vaccines are administered simultaneously, the immune system is capable of mounting effective responses to both without interference. This is because the immune system has the capacity to handle multiple antigens at once, especially in healthy individuals. However, if simultaneous administration is not feasible, the 28-day interval remains the gold standard to ensure optimal immune response and vaccine efficacy. Parents and caregivers should work closely with healthcare providers to schedule vaccinations appropriately, taking into account the timing requirements for live vaccines like MMR and Varicella.
Understanding the immune response and vaccine efficacy timing is essential for both healthcare providers and the public. It highlights the importance of adhering to vaccination schedules to achieve the best possible protection against preventable diseases. By respecting the 28-day interval between live vaccines, we can ensure that the immune system functions optimally, providing long-term immunity and reducing the risk of disease outbreaks. This approach not only protects individuals but also contributes to herd immunity, safeguarding communities as a whole.
Smallpox Vaccine: Transforming the New World's Health and History
You may want to see also
Explore related products



![]()
Simultaneous Administration Guidelines for MMR and Varicella
When considering the simultaneous administration of live vaccines such as MMR (Measles, Mumps, and Rubella) and Varicella (Chickenpox), healthcare providers must adhere to specific guidelines to ensure optimal immune response and minimize potential interference between vaccines. The Centers for Disease Control and Prevention (CDC) and the World Health Organization (WHO) provide recommendations to address the timing and administration of these live attenuated vaccines. The primary concern is the theoretical risk of one vaccine interfering with the immune response to the other if given too closely together. However, extensive research has shown that administering MMR and Varicella vaccines simultaneously is both safe and effective, eliminating the need for a minimum interval between these vaccines.
Simultaneous administration of MMR and Varicella vaccines is the preferred approach when both vaccines are due. This practice not only ensures timely protection against these diseases but also reduces the number of visits required for vaccination, improving compliance and coverage rates. The combined measles, mumps, rubella, and varicella (MMRV) vaccine is an option for children aged 12 months through 12 years, further simplifying the vaccination process. When using separate MMR and Varicella vaccines, they can be administered at the same visit in different anatomical sites (e.g., one in each arm) without compromising their efficacy.
If simultaneous administration is not feasible or is deferred for any reason, the minimum interval between live vaccines, including MMR and Varicella, is generally 28 days. This interval is based on historical caution rather than evidence of significant interference. However, waiting 28 days is not necessary if the vaccines are given simultaneously or if the MMRV combination vaccine is used. It is important to note that if a dose of a live vaccine is given within 28 days of another live vaccine, the dose does not need to be repeated, as the likelihood of interference is minimal.
Healthcare providers should carefully document the administration of MMR and Varicella vaccines, ensuring that both the date and the specific vaccine given are recorded. This documentation is crucial for maintaining accurate immunization records and facilitating future vaccination decisions. Parents and caregivers should also be informed about the benefits of simultaneous administration and the rationale behind the timing guidelines to address any concerns and encourage adherence to the vaccination schedule.
In summary, the simultaneous administration of MMR and Varicella vaccines is strongly recommended when both are due, as it provides timely protection and simplifies the vaccination process. If separate vaccines are used, they should be given in different anatomical sites during the same visit. While a 28-day interval is traditionally observed between live vaccines, it is not required for MMR and Varicella when given simultaneously or as the MMRV combination vaccine. Adhering to these guidelines ensures effective immunization and supports public health efforts to control measles, mumps, rubella, and varicella.
Delta Variant Risks: What Vaccinated Individuals Need to Know
You may want to see also
![]()
Potential Risks of Shortened Vaccine Intervals
The recommended interval between live vaccines, such as MMR (measles, mumps, rubella) and varicella (chickenpox), is typically 28 days. This spacing is advised by health organizations like the CDC and WHO to ensure optimal immune response and minimize potential risks. Shortening this interval can lead to several adverse outcomes, primarily related to the way live vaccines interact with the immune system. Live vaccines contain weakened forms of the virus, which stimulate the body to produce immunity. When administered too closely together, the immune response to one vaccine may interfere with the response to the other, potentially reducing the effectiveness of both.
One of the primary risks of shortened vaccine intervals is reduced immunogenicity. Studies suggest that if live vaccines are given too close together, the immune system may not mount a full response to either vaccine. For example, the varicella vaccine might not induce sufficient antibodies if given shortly after the MMR vaccine, leaving the individual partially unprotected against chickenpox. Similarly, the MMR vaccine’s efficacy could be compromised, increasing the risk of breakthrough infections for measles, mumps, or rubella. This reduced immunity defeats the purpose of vaccination and leaves individuals vulnerable to preventable diseases.
Another concern is the potential for vaccine interference. Live vaccines compete for the same immune resources, and administering them too closely can result in one vaccine dominating the immune response, thereby suppressing the response to the other. This interference can lead to suboptimal protection and may require additional doses to achieve adequate immunity. For instance, if the MMR vaccine is given too soon before or after the varicella vaccine, the body might prioritize one over the other, resulting in incomplete immunity to both diseases.
Shortened intervals may also increase the risk of adverse reactions. While live vaccines are generally safe, administering them too closely together could overwhelm the immune system, potentially leading to more frequent or severe side effects, such as fever, rash, or discomfort. These reactions, though usually mild, can cause unnecessary distress and may deter individuals from completing their vaccination schedules. Additionally, there is a theoretical risk of viral interference, where the weakened viruses in the vaccines could interact in unpredictable ways, though this is less common and not well-documented.
Finally, deviating from the recommended vaccine schedule can complicate public health efforts. Standardized intervals ensure consistency in immunity across populations, which is crucial for herd immunity. Shortened intervals may lead to inconsistent protection, making it harder to control outbreaks of diseases like measles or chickenpox. Healthcare providers rely on established guidelines to administer vaccines safely and effectively, and disregarding these intervals can undermine trust in vaccination programs and create confusion among patients.
In summary, shortening the interval between live vaccines like MMR and varicella poses risks such as reduced immunogenicity, vaccine interference, increased adverse reactions, and challenges to public health efforts. Adhering to the recommended 28-day interval is essential to ensure optimal protection and maintain the integrity of vaccination programs. Always consult healthcare professionals for guidance on vaccine scheduling to minimize risks and maximize benefits.
COVID-19 Vaccine Progress: How Close Are We to a Solution?
You may want to see also
![]()
CDC and WHO Recommendations on Vaccine Spacing
The Centers for Disease Control and Prevention (CDC) and the World Health Organization (WHO) provide clear guidelines on the spacing of live vaccines, including the Measles, Mumps, and Rubella (MMR) vaccine and the Varicella (chickenpox) vaccine. These recommendations are designed to ensure optimal immune response and minimize potential interference between vaccines. According to the CDC, if the MMR and Varicella vaccines are administered on the same day, they can be given simultaneously in separate syringes at different injection sites. However, if they are not given on the same day, the CDC advises that these live vaccines should be spaced at least 28 days apart. This interval is crucial because administering live vaccines too closely together may result in one vaccine interfering with the immune response to the other, potentially reducing their effectiveness.
The WHO aligns closely with the CDC's recommendations, emphasizing the importance of a 28-day interval between live vaccines when they are not administered simultaneously. This spacing guideline applies to both children and adults receiving live attenuated vaccines, such as MMR and Varicella. The rationale behind this recommendation is rooted in immunological principles, as the immune system needs adequate time to mount a robust response to each vaccine without interference. Both organizations stress that if the 28-day interval is not followed, the vaccine administered second may need to be repeated to ensure full protection. This is particularly important in regions with high disease prevalence, where immunity gaps could lead to outbreaks.
In situations where the 28-day interval is not feasible, the CDC and WHO provide flexibility. For example, if there is an immediate risk of disease exposure, such as during an outbreak, the vaccines may be given at any time, even if less than 28 days have passed since the previous live vaccine. However, in such cases, the second vaccine should be repeated after the recommended interval to ensure long-term immunity. This exception highlights the balance between immediate protection and long-term immune response, a key consideration in public health decision-making.
For healthcare providers, adhering to these spacing guidelines is essential for effective vaccination programs. The CDC and WHO recommend documenting vaccine administration dates carefully to avoid errors in scheduling. Additionally, providers should educate patients and caregivers about the importance of following the recommended intervals to maximize vaccine efficacy. In cases where multiple live vaccines are due, planning ahead to administer them on the same day, when possible, can simplify the vaccination schedule and ensure compliance with guidelines.
Lastly, it is important to note that these recommendations are based on extensive research and clinical trials. While the 28-day interval is standard, studies have shown that even if live vaccines are given closer together, they generally still provide protection, though the response may be suboptimal. However, adhering strictly to the guidelines ensures the highest level of immunity and reduces the need for revaccination. Both the CDC and WHO regularly review and update their recommendations based on new scientific evidence, ensuring that vaccine spacing guidelines remain effective and relevant in global health practice.
RFK's Anti-Vax Agenda: A Dangerous Threat to Public Health
You may want to see also
Frequently asked questions
The CDC recommends that if the MMR and Varicella vaccines are not administered on the same day, they should be given at least 28 days apart.
Yes, the MMR and Varicella vaccines can be administered simultaneously without any interval, as they are often combined into a single shot called the MMRV vaccine.
If the vaccines are given less than 28 days apart, the immune response may be suboptimal. In such cases, the dose given too soon is considered invalid, and the vaccine should be repeated after the appropriate interval.
Yes, the 28-day interval between live MMR and Varicella vaccines applies to both children and adults if the vaccines are not given on the same day.