As of the latest data, there are over 30 coronavirus vaccines that have been authorized for use in various countries around the world, with more than 150 additional candidates in different stages of development. These vaccines have been developed using diverse technologies, including mRNA (e.g., Pfizer-BioNTech, Moderna), viral vector (e.g., AstraZeneca, Johnson & Johnson), and inactivated virus (e.g., Sinopharm, Sinovac) platforms. The global rollout of these vaccines has been instrumental in combating the COVID-19 pandemic, with billions of doses administered worldwide. However, disparities in vaccine distribution and access persist, particularly between high-income and low-income countries, highlighting ongoing challenges in achieving equitable global immunization.
| Characteristics | Values |
|---|---|
| Total Number of COVID-19 Vaccines Approved Globally | Over 30 vaccines have been authorized for use in various countries. |
| Vaccines Approved by WHO for Emergency Use | 13 vaccines (as of October 2023), including Pfizer-BioNTech, Moderna, Oxford-AstraZeneca, Johnson & Johnson, Sinopharm, Sinovac, Covaxin, etc. |
| Vaccines in Clinical Trials | Over 100 vaccine candidates in clinical trials globally. |
| Vaccines in Preclinical Development | Approximately 180 vaccine candidates in preclinical stages. |
| Vaccine Types | mRNA (e.g., Pfizer, Moderna), Viral Vector (e.g., AstraZeneca, J&J), Inactivated (e.g., Sinopharm, Sinovac), Protein Subunit (e.g., Novavax), DNA, etc. |
| Global Vaccine Doses Administered | Over 13 billion doses administered worldwide (as of October 2023). |
| Countries with Vaccines | Over 220 countries and territories have initiated vaccination campaigns. |
| Vaccine Equity Issues | Significant disparities in vaccine distribution between high-income and low-income countries. |
| Booster Doses Administered | Over 2 billion booster doses administered globally. |
| Vaccine Efficacy Range | 50% to 95% depending on the vaccine and variant. |
Explore related products






What You'll Learn
- Total vaccines developed globally: Number of COVID-19 vaccines created and approved worldwide by health authorities
- Vaccines by technology type: Breakdown of vaccines by mRNA, viral vector, protein subunit, and inactivated virus types
- Vaccine distribution by country: Global distribution and accessibility of coronavirus vaccines across different nations
- Vaccine efficacy rates: Comparison of effectiveness rates among various approved coronavirus vaccines
- Vaccines in clinical trials: Number of COVID-19 vaccines currently undergoing testing in clinical trials
![]()
Total vaccines developed globally: Number of COVID-19 vaccines created and approved worldwide by health authorities
As of the latest data, over 30 COVID-19 vaccines have been authorized for use by at least one country, with more than 15 receiving approval from stringent regulatory authorities like the World Health Organization (WHO), the U.S. Food and Drug Administration (FDA), or the European Medicines Agency (EMA). These vaccines represent a diverse array of technologies, including mRNA (e.g., Pfizer-BioNTech, Moderna), viral vector (e.g., AstraZeneca, Johnson & Johnson), and inactivated virus (e.g., Sinovac, Sinopharm) platforms. Each vaccine has undergone rigorous clinical trials to ensure safety and efficacy, though approval criteria and rollout strategies vary by region. For instance, the Pfizer-BioNTech vaccine is typically administered in a two-dose regimen, 3–4 weeks apart, while Johnson & Johnson’s single-dose approach offers a logistical advantage in hard-to-reach areas.
Analyzing the global distribution reveals disparities in access and approval. High-income countries have predominantly approved mRNA vaccines due to their high efficacy rates (around 95% for Pfizer-BioNTech and Moderna), while low- and middle-income countries often rely on more cost-effective options like AstraZeneca or Sinopharm. The WHO’s Emergency Use Listing (EUL) has been instrumental in standardizing approvals for global use, with vaccines like Covaxin (India) and Abdala (Cuba) gaining recognition. However, the pace of approval varies; some countries prioritize local production, such as Russia’s Sputnik V, which has been authorized in over 70 nations despite limited initial data sharing.
From a practical standpoint, understanding vaccine dosages and age restrictions is crucial. Most vaccines are approved for adults aged 18 and above, but several, including Pfizer-BioNTech and Moderna, have expanded their use to adolescents (12–17 years) and, more recently, children as young as 6 months. Booster doses are recommended 3–6 months after the primary series to maintain immunity, particularly against emerging variants. For travelers, verifying which vaccines are recognized by their destination country is essential, as some nations only accept WHO-approved vaccines for entry.
A comparative analysis highlights the trade-offs between vaccine types. mRNA vaccines offer superior efficacy but require ultra-cold storage, making them less accessible in resource-limited settings. In contrast, viral vector and inactivated vaccines are more stable but may have slightly lower efficacy rates. For example, AstraZeneca’s vaccine has an average efficacy of 70–80%, but its ease of storage and lower cost make it a preferred choice in many developing countries. Johnson & Johnson’s single-dose format simplifies distribution, though rare side effects like thrombosis have limited its use in certain demographics.
In conclusion, the global COVID-19 vaccine landscape is a testament to unprecedented scientific collaboration and innovation. With over 30 approved vaccines, the focus has shifted from development to equitable distribution and public acceptance. Practical considerations, such as dosage schedules, age approvals, and storage requirements, play a critical role in maximizing their impact. As new variants emerge, ongoing research and regulatory flexibility will be key to adapting vaccines and ensuring global protection.
Vaccine Safety Concerns: Historical Cases of Failed Immunizations Explored
You may want to see also
Explore related products






![]()
Vaccines by technology type: Breakdown of vaccines by mRNA, viral vector, protein subunit, and inactivated virus types
As of the latest data, there are over 30 approved COVID-19 vaccines globally, each developed using distinct technological platforms. These vaccines fall into four primary categories: mRNA, viral vector, protein subunit, and inactivated virus types. Understanding these technologies is crucial for informed decision-making, as each has unique mechanisms, efficacy rates, and administration protocols.
MRNA Vaccines: Pioneers in Speed and Efficacy
The mRNA vaccines, exemplified by Pfizer-BioNTech and Moderna, revolutionized the vaccine landscape. These vaccines deliver genetic instructions to cells, prompting them to produce a harmless spike protein that triggers an immune response. Notably, Pfizer’s vaccine requires two doses, 21 days apart, while Moderna’s doses are administered 28 days apart. Both boast efficacy rates above 90% against severe disease, with booster shots recommended 6 months post-primary series. Storage is a key consideration: Pfizer requires ultra-cold temperatures (-70°C), whereas Moderna can be stored at -20°C, easing distribution challenges.
Viral Vector Vaccines: Versatile and Accessible
Viral vector vaccines, such as AstraZeneca and Johnson & Johnson (J&J), use a modified virus (e.g., adenovirus) to deliver genetic material encoding the spike protein. AstraZeneca’s vaccine is administered in two doses, 4–12 weeks apart, with an efficacy of around 70–80%. J&J offers a single-dose regimen, making it a practical choice for hard-to-reach populations, though its efficacy is slightly lower at 66–72%. Rare but serious side effects, such as thrombosis with thrombocytopenia syndrome (TTS), have been reported, primarily in younger adults, prompting age-specific recommendations in some countries.
Protein Subunit Vaccines: Safe and Targeted
Protein subunit vaccines, like Novavax, contain purified pieces of the virus (e.g., the spike protein) to stimulate an immune response. Novavax’s vaccine is administered in two doses, 3–4 weeks apart, with an efficacy of approximately 90%. This type is particularly appealing for those hesitant about newer technologies, as it uses a more traditional approach. Additionally, it can be stored at standard refrigerator temperatures (2–8°C), simplifying logistics.
Inactivated Virus Vaccines: Tried and True
Inactivated virus vaccines, such as Sinovac (CoronaVac) and Sinopharm, use viruses that have been killed to trigger immunity. These vaccines typically require two doses, 2–4 weeks apart, with booster shots advised for sustained protection. Efficacy varies widely, with Sinovac reporting 50–90% effectiveness depending on the study. Their stability at standard refrigeration temperatures makes them suitable for low-resource settings, though multiple doses are often needed to achieve robust immunity.
Practical Takeaways for Vaccine Selection
Choosing a vaccine depends on availability, individual health conditions, and logistical constraints. mRNA vaccines offer high efficacy but require careful storage, while viral vector vaccines provide flexibility with single-dose options. Protein subunit vaccines combine safety with ease of distribution, and inactivated virus vaccines are accessible but may necessitate additional doses. Always consult healthcare providers for personalized advice, especially regarding boosters and age-specific recommendations.
NHS Pneumonia Vaccine Eligibility: Who Qualifies for Protection?
You may want to see also
Explore related products






![]()
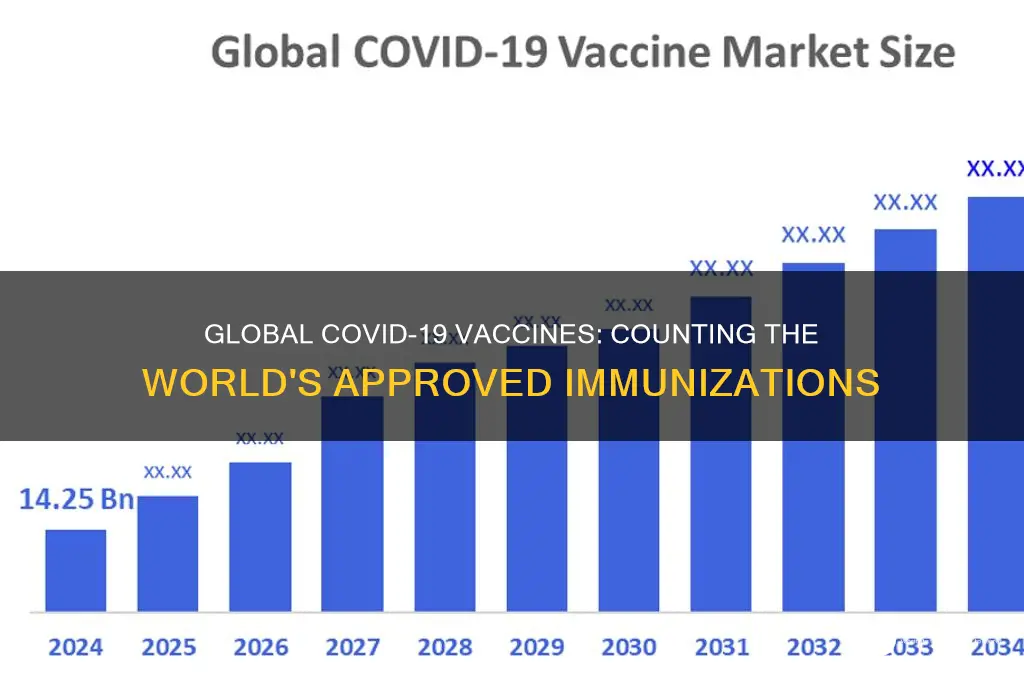
Vaccine distribution by country: Global distribution and accessibility of coronavirus vaccines across different nations
As of recent data, over 13 billion COVID-19 vaccine doses have been administered globally, yet the distribution remains starkly uneven. High-income countries, such as the United States, Canada, and those in Western Europe, have secured and administered a disproportionate share of these doses, often achieving vaccination rates above 70% of their populations. In contrast, many low-income nations in Africa and parts of Asia struggle with single-digit vaccination rates, highlighting a glaring disparity in global health equity. This imbalance is not merely a statistic but a reflection of systemic inequalities in access to life-saving resources.
Consider the logistical challenges that exacerbate this divide. Wealthier nations have invested heavily in cold chain infrastructure, ensuring vaccines like Pfizer-BioNTech (requiring -70°C storage) remain viable. Poorer countries, lacking such resources, often rely on vaccines like AstraZeneca or Johnson & Johnson, which are more heat-stable but less readily available due to supply chain priorities. For instance, while the U.S. has donated over 600 million doses abroad, many of these have expired before reaching arms, underscoring the need for coordinated distribution strategies rather than ad hoc donations.
A persuasive argument emerges when examining the role of vaccine nationalism and intellectual property rights. Wealthy nations and pharmaceutical companies have resisted waiving patents, limiting the ability of low-income countries to produce vaccines locally. The World Health Organization’s COVAX initiative, designed to address this, has fallen short of its targets, delivering only 1.4 billion doses against a goal of 2 billion by 2022. Without structural changes, such as technology transfer and patent waivers, global accessibility will remain a distant goal, leaving billions vulnerable to new variants.
Comparatively, success stories like India and China offer instructive models. India, despite initial challenges, scaled up domestic production of the Oxford-AstraZeneca vaccine (branded as Covishield) and administered over 2 billion doses, achieving 90% adult vaccination. China, with its Sinovac and Sinopharm vaccines, has vaccinated over 85% of its population and exported doses to 100+ countries. These examples demonstrate that localized production and political will can overcome distribution barriers, even in resource-constrained settings.
Practically, improving accessibility requires a multi-faceted approach. First, high-income nations must fulfill their dose-sharing pledges without attaching conditions. Second, low-income countries should prioritize last-mile delivery strategies, such as mobile clinics and community health workers, to reach rural populations. Third, global health organizations must advocate for patent waivers and technology transfer to enable regional vaccine production. Finally, individuals in privileged nations can advocate for equitable policies and support organizations like Gavi, the Vaccine Alliance, which funds immunization programs worldwide. Without collective action, the promise of vaccines as a global public good will remain unfulfilled.
Hepatitis B Vaccine and Mercury: Debunking Myths and Facts
You may want to see also
Explore related products






![]()
Vaccine efficacy rates: Comparison of effectiveness rates among various approved coronavirus vaccines
As of the latest data, over 15 coronavirus vaccines have been approved for use worldwide, each with varying efficacy rates and mechanisms of action. This diversity in vaccine development has been crucial in combating the global pandemic, but it also raises questions about which vaccines offer the highest protection. Efficacy rates, typically measured in clinical trials, indicate the percentage reduction in disease occurrence among vaccinated individuals compared to those who receive a placebo. Understanding these rates is essential for informed decision-making, both at the individual and policy levels.
Analytically speaking, the Pfizer-BioNTech and Moderna vaccines, both mRNA-based, have consistently demonstrated high efficacy rates. Pfizer-BioNTech reported an initial efficacy of 95% in preventing symptomatic COVID-19 in individuals aged 16 and older, with a two-dose regimen administered 21 days apart. Moderna’s vaccine closely follows, with an efficacy rate of 94.1% after two doses given 28 days apart. These vaccines have also shown robust protection against severe disease and hospitalization, even as new variants emerge. However, their storage requirements—ultra-cold temperatures for Pfizer-BioNTech and standard freezer temperatures for Moderna—pose logistical challenges in some regions.
In contrast, viral vector vaccines like Oxford-AstraZeneca and Johnson & Johnson offer different efficacy profiles and practical advantages. Oxford-AstraZeneca’s vaccine has an average efficacy of around 70%, but it is highly effective in preventing severe illness and hospitalization. Its storage at standard refrigerator temperatures makes it more accessible in low-resource settings. Johnson & Johnson’s single-dose vaccine provides approximately 66% protection against moderate to severe COVID-19 globally, rising to 85% against severe disease. This one-shot approach simplifies vaccination campaigns, particularly in hard-to-reach populations.
Persuasively, it’s important to note that efficacy rates are not the sole measure of a vaccine’s value. Factors like dosage schedules, age-specific responses, and real-world effectiveness play critical roles. For instance, some vaccines, like Sinopharm and Sinovac, have lower reported efficacy rates (around 78% and 51%, respectively) but have been widely deployed in many countries due to their ease of distribution and cost-effectiveness. Additionally, booster doses have proven essential in maintaining high protection levels, particularly against variants like Delta and Omicron.
Practically, individuals should follow local health guidelines for vaccine selection and dosing. For example, those with access to mRNA vaccines may opt for Pfizer-BioNTech or Moderna for higher initial efficacy, while others might prioritize single-dose options like Johnson & Johnson for convenience. Age-specific recommendations also matter; some vaccines, like Pfizer-BioNTech, are approved for children as young as 5, while others are limited to adults. Regularly updating vaccinations with boosters is crucial, as immunity wanes over time. Ultimately, the goal is not to compare vaccines in a competitive sense but to maximize global coverage and protection against COVID-19.
Respectfully Addressing Vaccine Hesitancy: Strategies for Compassionate Conversations
You may want to see also
Explore related products






![]()
Vaccines in clinical trials: Number of COVID-19 vaccines currently undergoing testing in clinical trials
As of the latest data, over 200 COVID-19 vaccine candidates are in various stages of development worldwide, with a significant portion currently undergoing clinical trials. These trials are critical to ensuring the safety, efficacy, and optimal dosage of vaccines before they receive regulatory approval and become available to the public. Among these, approximately 50 vaccines are in Phase III trials, the final stage before potential authorization, where large-scale testing in thousands of volunteers assesses real-world effectiveness and monitors side effects.
Analyzing the diversity of these candidates reveals a mix of traditional and cutting-edge technologies. mRNA vaccines, like those from Pfizer-BioNTech and Moderna, have already proven successful, but trials continue to refine dosing for specific populations, such as children under 5, who typically receive a lower dose (e.g., 10 micrograms per shot compared to 30 micrograms for adults). Meanwhile, protein subunit vaccines, like Novavax, and viral vector vaccines, such as AstraZeneca’s, are being tested for booster efficacy and cross-protection against emerging variants.
For those considering participation in clinical trials, understanding the process is key. Volunteers are often grouped by age, health status, and geographic location to ensure diverse representation. Trials typically involve multiple visits, including screenings, vaccinations, and follow-up assessments. Participants may receive a placebo or the actual vaccine, but all are closely monitored for adverse reactions. Practical tips include keeping a symptom diary, staying hydrated, and reporting any unusual symptoms immediately to trial coordinators.
Comparatively, the pace of vaccine development for COVID-19 has been unprecedented, thanks to global collaboration and expedited regulatory processes. However, challenges remain, such as ensuring equitable access to vaccines and addressing hesitancy fueled by misinformation. Ongoing trials also focus on combination vaccines that protect against COVID-19 and other respiratory viruses, like influenza, which could streamline immunization schedules in the future.
In conclusion, the number of COVID-19 vaccines in clinical trials reflects a robust global effort to combat the pandemic. Each candidate brings unique advantages, from improved storage conditions to enhanced variant protection. For individuals, staying informed about trial opportunities and understanding the science behind these vaccines can empower better health decisions. As research progresses, these trials will not only expand our vaccine arsenal but also lay the groundwork for tackling future infectious diseases.
Prevnar 20 vs. RSV Vaccine: Understanding the Key Differences
You may want to see also
Frequently asked questions
As of October 2023, over 20 different COVID-19 vaccines have been authorized for use in various countries, including mRNA vaccines (e.g., Pfizer-BioNTech, Moderna), viral vector vaccines (e.g., AstraZeneca, Johnson & Johnson), and inactivated vaccines (e.g., Sinopharm, Sinovac).
As of October 2023, over 13 billion doses of COVID-19 vaccines have been administered worldwide, with varying distribution rates across regions.
Over 10 countries have developed and authorized their own COVID-19 vaccines, including the United States, China, Russia, India, and the United Kingdom, with collaborations often involving multiple nations and organizations.