Childhood vaccines are a cornerstone of public health, protecting children from serious and potentially life-threatening diseases. The number of vaccines administered during childhood varies by country and healthcare guidelines, but in the United States, the Centers for Disease Control and Prevention (CDC) recommends a comprehensive schedule that includes vaccines against 14 preventable diseases. These vaccines are typically administered in a series of doses starting at birth and continuing through adolescence, with the goal of building immunity before exposure to pathogens. Common vaccines include those for measles, mumps, rubella, polio, hepatitis B, and influenza, among others. Understanding the number and timing of these vaccines is crucial for parents and caregivers to ensure children receive optimal protection and contribute to herd immunity.
Explore related products


$11.93 $21.99




What You'll Learn
- Vaccine Schedule Overview: Standard timelines for childhood vaccinations, including age-specific recommendations
- Common Childhood Vaccines: List of essential vaccines (e.g., MMR, DTaP, polio)
- Number by Age: Breakdown of vaccine counts by age group (infants to teens)
- Global Variations: Differences in vaccine administration across countries and regions
- Combination Vaccines: How multiple vaccines are often combined to reduce administration frequency
![]()
Vaccine Schedule Overview: Standard timelines for childhood vaccinations, including age-specific recommendations
Childhood vaccination schedules are meticulously designed to protect infants and young children when they are most vulnerable to infectious diseases. The Centers for Disease Control and Prevention (CDC) and the American Academy of Pediatrics (AAP) recommend a standardized timeline that begins at birth, with the first dose of the hepatitis B vaccine typically administered within 24 hours of life. This early intervention sets the stage for a series of vaccinations that continue through adolescence, ensuring immunity is built during critical developmental stages.
By the age of 2, children should receive multiple doses of vaccines protecting against diseases such as diphtheria, tetanus, pertussis (DTaP), polio (IPV), measles, mumps, rubella (MMR), and varicella (chickenpox). For instance, the DTaP vaccine is given in a series of 5 doses, starting at 2 months and concluding between 4–6 years. Similarly, the MMR vaccine is administered in two doses, the first at 12–15 months and the second at 4–6 years. This staggered approach allows the immune system to develop robust immunity without overwhelming it.
Adolescence introduces new vaccines tailored to emerging health risks. At age 11–12, preteens receive the Tdap booster to reinforce protection against tetanus, diphtheria, and pertussis, as well as the meningococcal conjugate vaccine (MenACWY) and the human papillomavirus (HPV) vaccine series. The HPV vaccine, for example, is given in 2 or 3 doses depending on the age at initiation—a critical measure in preventing cancers linked to HPV infection. These vaccines highlight the evolving nature of immunization schedules to address changing disease landscapes.
Practical adherence to the vaccine schedule is essential but can be challenging. Parents should maintain a vaccination record, utilize reminder systems offered by healthcare providers, and schedule appointments well in advance to avoid delays. Catch-up schedules are available for children who fall behind, ensuring they still receive the full protective benefits. For families with concerns about vaccine safety or timing, consulting a pediatrician for personalized guidance is strongly recommended. This proactive approach ensures children remain on track to receive the approximately 14–16 vaccinations that comprise the standard childhood immunization regimen.
Understanding AAHS Control in Gardasil Vaccine Research: Key Insights
You may want to see also
Explore related products






![]()
Common Childhood Vaccines: List of essential vaccines (e.g., MMR, DTaP, polio)
Childhood vaccination schedules are meticulously designed to protect against serious, preventable diseases. Among the most critical vaccines are the MMR (Measles, Mumps, Rubella), DTaP (Diphtheria, Tetanus, Pertussis), and polio vaccines. These immunizations are typically administered in a series of doses starting as early as 2 months of age, with boosters given at specific intervals to ensure lasting immunity. For instance, the MMR vaccine is first given between 12 and 15 months, followed by a second dose between 4 and 6 years, while the DTaP series begins at 2 months, with doses at 4 months, 6 months, 15-18 months, and 4-6 years.
The MMR vaccine is a cornerstone of childhood immunization, preventing three highly contagious diseases. Measles, known for its rash and high fever, can lead to pneumonia and encephalitis, while mumps causes swollen glands and potential complications like deafness. Rubella, though mild in children, poses severe risks to pregnant women, including miscarriage and congenital rubella syndrome. Administered as a two-dose series, the MMR vaccine is 97% effective after both doses. Parents should be aware that mild side effects, such as fever or rash, are common but far less severe than the diseases themselves.
DTaP is another vital vaccine, protecting against diphtheria, tetanus, and pertussis (whooping cough). Diphtheria causes a thick coating in the throat, leading to breathing difficulties, while tetanus, or lockjaw, results from bacterial infection through wounds. Pertussis is particularly dangerous for infants, causing violent coughing fits that can lead to pneumonia or rib fractures. The DTaP series consists of five doses, with the first three given at 2, 4, and 6 months, followed by boosters at 15-18 months and 4-6 years. Adolescents and adults require a Tdap booster to maintain immunity and protect vulnerable populations.
Polio vaccination has nearly eradicated this once-feared disease, which can cause paralysis and death. The inactivated polio vaccine (IPV) is administered in four doses: at 2 months, 4 months, 6-18 months, and 4-6 years. Unlike the oral polio vaccine (OPV), IPV cannot cause vaccine-derived polio, making it the safer choice for routine immunization. Parents in regions with ongoing polio transmission should ensure their children receive all doses, as even a single case can reignite outbreaks in unvaccinated communities.
Practical tips for parents include keeping a detailed record of vaccine doses and dates, as this information is crucial for school enrollment and travel. Scheduling well-child visits in advance ensures timely administration, and discussing any concerns with a healthcare provider can address hesitations. While vaccine side effects like soreness or low-grade fever are normal, severe reactions are extremely rare. By adhering to the recommended schedule, parents play a vital role in safeguarding their children and contributing to herd immunity, protecting those who cannot be vaccinated due to medical reasons.
Did Robert Malone Invent mRNA Vaccines? Separating Fact from Fiction
You may want to see also
Explore related products





![]()
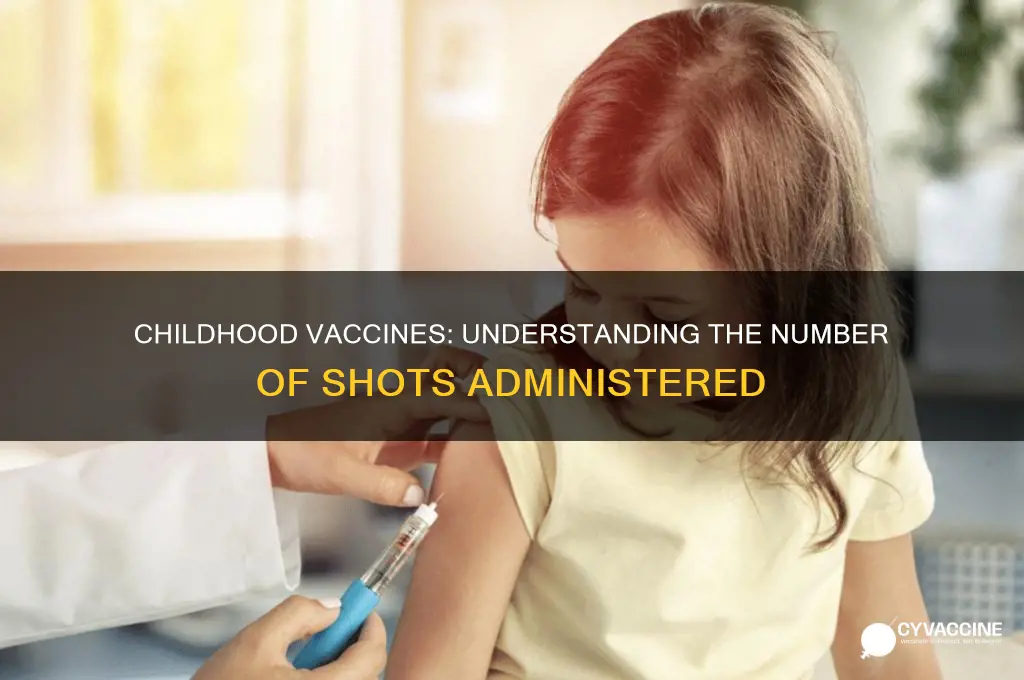
Number by Age: Breakdown of vaccine counts by age group (infants to teens)
Childhood vaccination schedules are meticulously designed to protect against serious diseases at the most vulnerable stages of life. From birth to adolescence, the number of vaccines administered varies significantly, tailored to the immune system’s development and disease risk at each age. Understanding this breakdown by age group ensures parents and caregivers can follow the recommended timeline effectively.
Infants (0–12 months): The Foundation Phase
In the first year, infants receive the highest number of vaccines to build immunity during a critical window of susceptibility. By 6 months, most babies will have received doses of the DTaP (diphtheria, tetanus, pertussis), Hib (Haemophilus influenzae type b), IPV (inactivated polio vaccine), and pneumococcal conjugate vaccine (PCV). The hepatitis B vaccine series often begins at birth, with doses at 1 and 6 months. Notably, the rotavirus vaccine, given orally in 2 or 3 doses, is completed by 8 months. This phase is intensive, with up to 15 doses of vaccines administered to protect against 9 diseases. Parents should adhere to well-child visits at 2, 4, 6, and 12 months to stay on track, ensuring gaps between doses are no longer than 4 weeks for combination vaccines.
Toddlers (1–2 years): Reinforcement and Expansion
Between 12 and 24 months, the focus shifts to reinforcing immunity and introducing new vaccines. Toddlers receive booster doses of DTaP, Hib, and PCV, along with the first dose of the MMR (measles, mumps, rubella) and varicella (chickenpox) vaccines. The hepatitis A vaccine series may also begin at this age, depending on risk factors. This phase typically involves 5–7 additional doses, bringing the cumulative total to around 20–24 doses by age 2. Caregivers should monitor for mild side effects like fever or soreness, which are normal and manageable with acetaminophen or cool compresses.
Preschool to Early School Age (3–6 years): Bridging the Gap
From ages 3 to 6, vaccination slows but remains crucial. Children receive booster doses of DTaP, IPV, MMR, and varicella, often combined into a single visit to minimize stress. This period typically adds 4–5 doses, bringing the total to approximately 25–30 doses by age 6. Parents should ensure all vaccines are up to date before entering kindergarten, as schools often require proof of immunization. This stage is also an opportunity to discuss vaccine safety with healthcare providers, addressing any concerns about ingredients like thimerosal or adjuvants.
Preteens and Teens (11–18 years): Transition to Adulthood
Adolescence marks a shift toward vaccines that protect against diseases prevalent in older age groups. At 11–12 years, preteens receive the Tdap booster (tetanus, diphtheria, pertussis), meningococcal conjugate vaccine (MenACWY), and HPV vaccine series (2–3 doses). The HPV vaccine, ideally started at age 11–12, is most effective before potential exposure to the virus. Teens may also receive a serogroup B meningococcal vaccine (MenB) and a final booster of MenACWY at age 16. This phase adds 5–8 doses, bringing the cumulative total to around 35–40 doses by age 18. Parents should use this period to educate teens about the importance of lifelong immunization, including future adult vaccines like tetanus boosters and flu shots.
Practical Tips for Every Age Group
Consistency is key across all age groups. Utilize immunization records or apps to track doses and schedule reminders. For infants and toddlers, breastfeeding during vaccination can reduce discomfort. School-age children may benefit from distraction techniques, like storytelling or toys. Teens should be involved in the process, understanding the rationale behind each vaccine. Always consult healthcare providers for personalized advice, especially for children with chronic conditions or immunocompromised states. By following these age-specific guidelines, caregivers can ensure comprehensive protection against preventable diseases throughout childhood.
Metals in Vaccines: Unraveling Their Role and Safety Concerns
You may want to see also
Explore related products






![]()
Global Variations: Differences in vaccine administration across countries and regions
The number of childhood vaccines administered varies dramatically across the globe, influenced by factors like healthcare infrastructure, economic resources, and cultural attitudes. In high-income countries like the United States, children typically receive around 14 vaccinations by age six, protecting against diseases such as measles, mumps, rubella, polio, and hepatitis B. These vaccines are often administered in multiple doses, starting as early as two months of age, following a standardized schedule designed to maximize immunity during critical developmental stages.
Contrast this with low-income regions in sub-Saharan Africa or Southeast Asia, where vaccine coverage can be as low as 50% for basic immunizations. Here, children may receive only essential vaccines like BCG (tuberculosis), oral polio vaccine, and measles, often delayed due to supply chain challenges or limited access to healthcare facilities. In some cases, vaccines are administered during mass immunization campaigns rather than routine clinic visits, leading to gaps in coverage and missed doses. This disparity highlights the critical role of global health initiatives like Gavi, the Vaccine Alliance, in bridging the immunization gap.
Cultural and religious beliefs also shape vaccine administration practices. For instance, in parts of India, Pakistan, and Afghanistan, skepticism about vaccines—fueled by misinformation or historical mistrust—has led to lower uptake, particularly for polio vaccination. Conversely, countries like Japan have historically limited certain vaccines, such as the HPV vaccine, due to public concerns over side effects, despite strong scientific evidence of safety and efficacy. These variations underscore the need for tailored communication strategies to address local hesitancy and build trust.
A comparative analysis reveals that middle-income countries often occupy a middle ground. Brazil, for example, has a robust national immunization program that includes 12 childhood vaccines, administered free of charge through public health clinics. Similarly, China has expanded its vaccine schedule to include newer vaccines like pneumococcal conjugate vaccine (PCV), reflecting its growing economic capacity and commitment to public health. However, even in these countries, urban-rural disparities persist, with rural children often receiving fewer doses due to logistical barriers.
To address these global variations, policymakers and health organizations must adopt context-specific strategies. In resource-limited settings, this might involve strengthening cold chain systems to preserve vaccine efficacy, training community health workers to deliver vaccines, or leveraging digital tools for tracking immunization records. In regions with high hesitancy, engaging local leaders and utilizing culturally sensitive messaging can improve acceptance. Ultimately, understanding these differences is not just about counting vaccines—it’s about ensuring equitable protection for every child, regardless of where they are born.
Identifying Smallpox Vaccine Scars: A Guide to Recognizing Past Immunization
You may want to see also
Explore related products






![]()
Combination Vaccines: How multiple vaccines are often combined to reduce administration frequency
Childhood immunization schedules can seem daunting, with the CDC recommending up to 14 separate vaccine doses by age two. However, combination vaccines streamline this process by bundling multiple antigens into a single injection. For instance, the DTaP vaccine protects against diphtheria, tetanus, and pertussis in one shot, reducing clinic visits and minimizing discomfort for the child. This approach not only simplifies scheduling but also improves adherence to vaccination timelines, a critical factor in achieving herd immunity.
Consider the MMR vaccine, a classic example of combination efficacy. Administered typically at 12–15 months and again at 4–6 years, it safeguards against measles, mumps, and rubella with a single dose. This consolidation eliminates the need for three separate injections, reducing stress for both children and caregivers. Similarly, the Pentacel vaccine combines DTaP, IPV (polio), and Hib (Haemophilus influenzae type b) into one shot, further exemplifying how combinations optimize the immunization process.
From a logistical standpoint, combination vaccines are a game-changer for healthcare providers. They reduce storage requirements, minimize preparation time, and lower the risk of administration errors. For parents, fewer appointments mean less time off work and reduced exposure to healthcare settings, where other illnesses could be contracted. However, it’s essential to note that not all vaccines can be combined due to compatibility issues or differing dosing schedules, such as the separate administration of the varicella (chickenpox) vaccine.
Despite their advantages, combination vaccines require careful consideration of potential side effects. While generally safe, they may cause localized reactions like redness or swelling at the injection site. Rarely, systemic symptoms such as fever can occur. Parents should monitor their child post-vaccination and consult a healthcare provider if concerns arise. Adhering to the recommended schedule, which often includes combination vaccines, ensures comprehensive protection without overwhelming the immune system.
In practice, combination vaccines are a cornerstone of modern pediatric care, balancing efficiency with efficacy. For example, the Kinrix vaccine offers a booster dose of DTaP and IPV for children aged 4–6, ensuring continued immunity with minimal disruption. By embracing these innovations, healthcare systems can deliver timely immunizations while respecting the practical constraints of families. Ultimately, combination vaccines represent a strategic approach to safeguarding children’s health, one streamlined dose at a time.
US Vaccination Rates: Tracking the Number of Vaccinated Americans
You may want to see also
Frequently asked questions
In the first year, infants typically receive around 10-12 vaccine doses, protecting against diseases like hepatitis B, rotavirus, diphtheria, tetanus, pertussis, Haemophilus influenzae type b (Hib), pneumococcal disease, polio, and influenza.
By age 6, children are recommended to receive approximately 25-30 vaccine doses, covering diseases such as measles, mumps, rubella, varicella (chickenpox), and others, depending on the specific schedule and vaccine combinations.
Many childhood vaccines are combined into a single shot to reduce the number of injections. For example, the DTaP vaccine protects against diphtheria, tetanus, and pertussis, and the MMR vaccine covers measles, mumps, and rubella.
By the time a child starts school (around age 5-6), they typically receive about 15-18 vaccine doses, ensuring protection against the most common and serious childhood diseases.
Yes, the number of childhood vaccines can vary by country based on local disease prevalence, public health priorities, and healthcare infrastructure. Some countries may include additional vaccines, such as BCG for tuberculosis or Japanese encephalitis, depending on regional needs.