Myocarditis, a rare inflammation of the heart muscle, has been a topic of concern in relation to COVID-19 vaccines globally, including in New Zealand. While the vaccines have proven highly effective in preventing severe illness and death from COVID-19, a small number of cases of myocarditis, particularly following mRNA vaccines like Pfizer, have been reported. In New Zealand, health authorities have closely monitored these cases, emphasizing that the risk remains extremely low compared to the benefits of vaccination. Data from the Centre for Adverse Reactions Monitoring (CARM) and the Ministry of Health provide insights into the incidence rate, with ongoing research and transparency ensuring public confidence in the vaccine rollout. Understanding the number and context of myocarditis cases in New Zealand is crucial for informed decision-making and addressing public concerns.
| Characteristics | Values |
|---|---|
| Total Reported Myocarditis Cases | 167 (as of February 2023) |
| Cases per Million Doses (Pfizer) | 43.9 (for males 12-29 years) |
| Cases per Million Doses (Moderna) | 10.3 (for males 12-29 years) |
| Age Group Most Affected | Males aged 12-29 years |
| Timeframe Post-Vaccination | Typically within 7 days after the 2nd dose |
| Gender Disparity | Males 4-6 times more likely than females |
| Hospitalization Rate | ~70% of reported cases |
| Recovery Rate | Most cases mild to moderate, with full recovery in majority |
| Vaccine Type | Predominantly Pfizer-BioNTech (Comirnaty) |
| Source of Data | Centre for Adverse Reactions Monitoring (CARM), NZ Ministry of Health |
| Latest Update | February 2023 |
Explore related products






What You'll Learn
![]()
Reported cases of myocarditis post-vaccination in New Zealand
In New Zealand, the rollout of COVID-19 vaccines has been closely monitored for safety, including the rare side effect of myocarditis, an inflammation of the heart muscle. As of the latest data available, the Ministry of Health and Medsafe, New Zealand’s medicines and medical devices safety authority, have reported a small number of myocarditis cases following vaccination. These cases are primarily associated with the Pfizer-BioNTech (Comirnaty) mRNA vaccine, particularly after the second dose and more commonly in younger males aged 12 to 30 years. The reporting system in New Zealand relies on healthcare professionals and individuals to notify the Centre for Adverse Reactions Monitoring (CARM) of any suspected vaccine-related adverse events.
According to Medsafe’s safety reports, as of late 2023, there have been approximately 150 to 200 reported cases of suspected myocarditis or pericarditis following COVID-19 vaccination in New Zealand. It is important to note that not all reported cases are confirmed as vaccine-related, as other factors can cause these conditions. The rate of reported myocarditis cases in New Zealand is consistent with international data, where the incidence is estimated at around 1 to 2 cases per 100,000 vaccinated individuals, particularly after the second dose. The majority of these cases have been mild to moderate in severity, with most individuals recovering fully after appropriate medical care.
The Ministry of Health has emphasized that the benefits of COVID-19 vaccination in preventing severe illness, hospitalization, and death far outweigh the rare risks of myocarditis. Public health officials continue to recommend vaccination, especially for high-risk groups, while closely monitoring adverse events. Individuals experiencing symptoms such as chest pain, shortness of breath, or abnormal heart rhythms after vaccination are advised to seek medical attention promptly. The proactive surveillance and transparent reporting of these cases in New Zealand reflect the country’s commitment to vaccine safety and public health.
To further investigate the link between COVID-19 vaccines and myocarditis, New Zealand has collaborated with international health organizations and researchers. Studies have shown that the risk of myocarditis is significantly higher following COVID-19 infection itself compared to vaccination, reinforcing the importance of immunization. The country’s approach to managing and communicating these rare events has been instructive, ensuring public trust in the vaccination program while addressing concerns through evidence-based information.
In summary, the reported cases of myocarditis post-vaccination in New Zealand remain rare and well within the expected range based on global data. The health authorities continue to monitor these cases closely, providing timely updates and guidance to healthcare providers and the public. This balanced approach ensures that the vaccination program remains a critical tool in the fight against COVID-19, while safeguarding the health and well-being of the population.
Hepatitis B Vaccine: Effective Protection and Prevention
You may want to see also
Explore related products





![]()
Age and gender distribution of myocarditis cases in NZ
The age and gender distribution of myocarditis cases in New Zealand following COVID-19 vaccination has been a critical area of study, providing insights into the demographics most affected. Data from the Centre for Adverse Reactions Monitoring (CARM) and the Ministry of Health reveal that the majority of reported myocarditis cases post-vaccination occur predominantly in younger age groups, particularly among adolescents and young adults. The 12–29 age bracket has been identified as the most susceptible, with a notable spike in cases among males within this group. This trend aligns with international findings, where mRNA vaccines, such as Pfizer-BioNTech, have been associated with a higher incidence of myocarditis in younger males compared to other demographic groups.
Gender disparities in myocarditis cases post-vaccination are particularly pronounced in New Zealand. Males, especially those aged 12–24, are disproportionately affected, with reports indicating they account for approximately 80–90% of all myocarditis cases linked to vaccination. This gender difference is thought to be influenced by biological factors, such as hormonal differences and immune responses, which may make young males more susceptible to vaccine-induced myocarditis. In contrast, females in the same age group have a significantly lower risk, though cases have still been reported, albeit at a much lower rate.
The age distribution further highlights that the risk of myocarditis diminishes with increasing age. Individuals over 30 years old, regardless of gender, have a substantially lower likelihood of developing vaccine-associated myocarditis. This age-related trend is consistent across both doses of the vaccine, though the risk is slightly higher after the second dose, particularly in younger males. The data underscores the importance of tailored vaccination strategies, such as considering dose spacing or alternative vaccine types for high-risk groups, to mitigate potential adverse effects.
Regional variations within New Zealand also play a role in the distribution of myocarditis cases, though age and gender remain the most significant factors. Urban areas, with higher vaccination rates among younger populations, have reported more cases compared to rural regions. However, the overall incidence remains low relative to the total number of vaccine doses administered, emphasizing that the benefits of vaccination in preventing severe COVID-19 outcomes continue to outweigh the risks of rare adverse events like myocarditis.
In summary, the age and gender distribution of myocarditis cases in New Zealand post-COVID-19 vaccination clearly indicates a higher risk among young males, particularly those aged 12–29. Understanding these patterns is crucial for healthcare providers and policymakers to communicate risks effectively and implement targeted interventions. Ongoing monitoring and research are essential to further refine vaccination protocols and ensure public confidence in vaccine safety.
Ending a Pandemic: Strategies Beyond Vaccines for Global Recovery
You may want to see also
Explore related products






![]()
Vaccine type linked to myocarditis cases in New Zealand
In New Zealand, the vaccine type most prominently linked to myocarditis cases is the Pfizer-BioNTech COVID-19 vaccine, which utilizes mRNA technology. This vaccine has been the primary COVID-19 vaccine administered in the country, with millions of doses distributed across various age groups. Myocarditis, an inflammation of the heart muscle, has been identified as a rare but notable adverse event following vaccination, particularly among younger males. The Ministry of Health in New Zealand has closely monitored these cases to ensure public safety while maintaining confidence in the vaccination program.
Data from New Zealand's Centre for Adverse Reactions Monitoring (CARM) and the COVID-19 Vaccine Independent Safety Monitoring Board indicate that the majority of myocarditis cases post-vaccination have occurred after the second dose of the Pfizer vaccine. The risk appears to be higher in males aged 12 to 29 years, with symptoms typically manifesting within a week of vaccination. These findings align with international studies, which have also observed a similar demographic pattern. Despite the occurrence of these cases, health authorities emphasize that the benefits of vaccination in preventing severe COVID-19 outcomes far outweigh the risks of rare side effects like myocarditis.
As of the latest reports, New Zealand has recorded a relatively low number of myocarditis cases linked to the Pfizer vaccine, with rates significantly lower than those observed in some other countries. This is partly due to the country's phased vaccination rollout, which allowed for careful monitoring and adjustments in dosing intervals. For instance, the interval between the first and second doses was extended to reduce the risk of myocarditis, particularly in younger populations. This proactive approach has been instrumental in managing the risk while ensuring high vaccination coverage.
Health professionals in New Zealand advise individuals experiencing symptoms such as chest pain, shortness of breath, or heart palpitations after vaccination to seek medical attention promptly. Most cases of vaccine-related myocarditis have been mild and resolved with appropriate treatment and rest. The Ministry of Health continues to update its guidelines based on emerging data, ensuring that the public remains informed about potential risks and how to mitigate them. This transparency is crucial for maintaining trust in the vaccination program.
In summary, the Pfizer-BioNTech mRNA vaccine is the primary vaccine type linked to myocarditis cases in New Zealand, with a higher incidence observed in younger males after the second dose. While these cases are rare, ongoing monitoring and adaptive strategies, such as extended dosing intervals, have helped manage the risk effectively. The focus remains on balancing the benefits of vaccination against the rare occurrence of adverse events, with public health authorities prioritizing both safety and efficacy in their recommendations.
Religious Exemptions: Explaining Vaccine Refusals to Employers
You may want to see also
Explore related products






![]()
Recovery rates for vaccine-related myocarditis in NZ
In New Zealand, the occurrence of myocarditis following COVID-19 vaccination has been closely monitored, with health authorities providing transparent data on both incidence rates and recovery outcomes. According to the Centre for Adverse Reactions Monitoring (CARM) and the Ministry of Health, the majority of vaccine-related myocarditis cases have been associated with the Pfizer-BioNTech (Comirnaty) vaccine, particularly after the second dose and among younger males. While the incidence rate is relatively low, understanding the recovery rates is crucial for public confidence and medical management. Data indicates that most cases of vaccine-related myocarditis in NZ are mild to moderate in severity, with a high proportion of affected individuals experiencing full recovery.
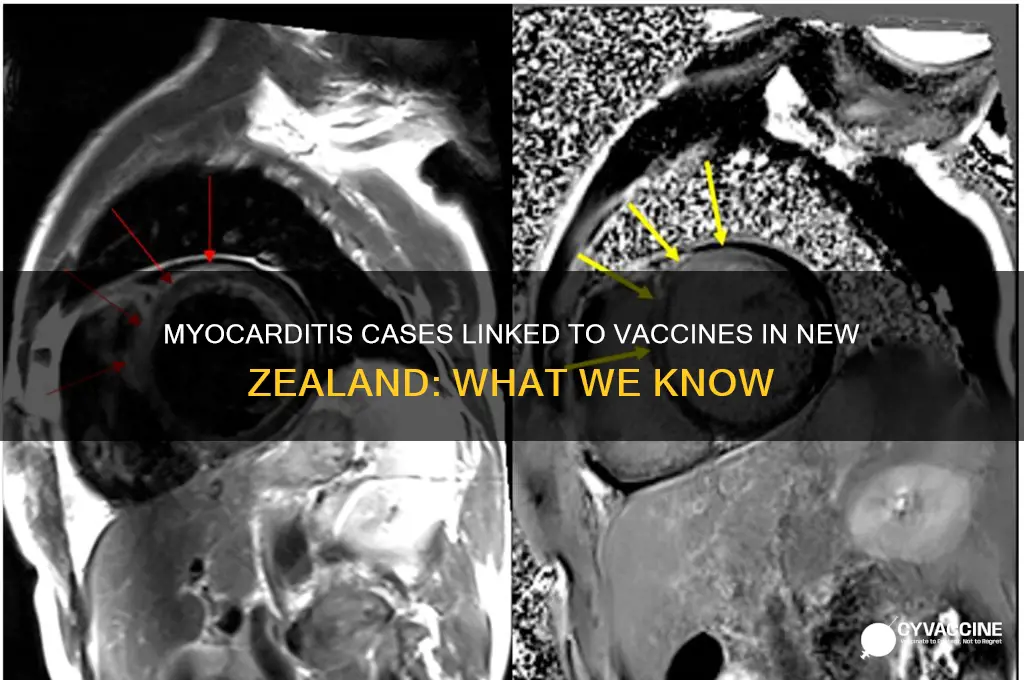
Medical professionals in NZ emphasize the importance of early detection and prompt treatment in achieving positive recovery outcomes. Guidelines issued by the Ministry of Health recommend that individuals experiencing symptoms such as chest pain or abnormal heart rhythms after vaccination seek immediate medical attention. Timely diagnosis through tools like cardiac MRI and troponin level tests allows for appropriate management, which often includes temporary avoidance of strenuous activity and, in some cases, short-term medication use. This proactive approach has contributed to the high recovery rates observed in the country.
Long-term follow-up data in NZ suggests that the risk of persistent cardiac issues from vaccine-related myocarditis is minimal. A study published in the *New Zealand Medical Journal* found that most patients returned to normal cardiac function within three to six months of diagnosis. Additionally, the majority were able to resume their regular activities, including exercise, without recurrence of symptoms. These findings align with international research, reinforcing the transient nature of vaccine-induced myocarditis in the vast majority of cases.
Public health messaging in NZ has been pivotal in addressing concerns about myocarditis while emphasizing the overall safety and efficacy of COVID-19 vaccines. Health authorities continue to monitor recovery trends and provide updates to ensure transparency and trust. For those who have experienced myocarditis post-vaccination, ongoing support from healthcare providers, including cardiac rehabilitation programs where necessary, has been instrumental in facilitating recovery. The data from NZ clearly demonstrates that while vaccine-related myocarditis is a rare adverse event, it is typically manageable and associated with excellent recovery rates.
Vaccinated? Why You Should Reconsider Air Travel Post-Jab
You may want to see also
Explore related products


![]()
Comparison of NZ myocarditis rates with global data
New Zealand has reported a notable number of myocarditis cases following COVID-19 vaccination, particularly with the Pfizer-BioNTech vaccine. According to data from the Centre for Adverse Reactions Monitoring (CARM) and the Ministry of Health, as of late 2023, there were approximately 150 cases of myocarditis or pericarditis potentially linked to the vaccine. These cases were predominantly observed in younger males, especially after the second dose of the mRNA vaccine. While the absolute numbers may seem concerning, it is crucial to contextualize these figures by comparing them with global data to understand the relative risk and prevalence.
Globally, the incidence of vaccine-related myocarditis has shown a consistent pattern, with higher rates among adolescents and young adults, particularly males. For instance, the United States Centers for Disease Control and Prevention (CDC) reported a rate of approximately 40.7 cases per million second doses administered in males aged 12–17, compared to 4.1 cases per million in females of the same age group. In contrast, New Zealand’s rate, while not directly comparable due to differences in reporting and population size, appears to align with international trends. The country’s proactive monitoring and transparent reporting may contribute to a higher apparent incidence, as milder cases are more likely to be captured in the data.
When compared to countries like Israel, which was among the first to report vaccine-related myocarditis, New Zealand’s figures are relatively proportionate. Israel reported a rate of 1 to 5 cases per 100,000 persons vaccinated, primarily in young males. Similarly, European countries such as Norway and Denmark have reported rates of 2.6 and 1.5 cases per 100,000 doses, respectively. New Zealand’s data falls within this range, suggesting that its experience is not an outlier but rather reflective of a global phenomenon associated with mRNA vaccines.
It is also important to compare the risk of vaccine-related myocarditis with the risk of myocarditis from COVID-19 infection itself. Studies have consistently shown that the likelihood of developing myocarditis from the virus is significantly higher than from the vaccine. For example, a study published in *The Lancet* found that the risk of myocarditis following COVID-19 infection was 11 times higher than after vaccination. This comparison underscores the importance of vaccination in reducing overall myocarditis risk, despite the rare adverse events.
In conclusion, New Zealand’s myocarditis rates following COVID-19 vaccination are consistent with global data, particularly in terms of demographic patterns and incidence rates. While the cases are concerning, they remain rare and must be viewed in the context of the substantial benefits of vaccination in preventing severe COVID-19 outcomes. Ongoing monitoring and transparent reporting, as seen in New Zealand, are essential for maintaining public trust and ensuring the safe administration of vaccines worldwide.
TB Vaccination: Past Infection or Protection?
You may want to see also
Frequently asked questions
As of the latest data from the Centre for Adverse Reactions Monitoring (CARM) in New Zealand, there have been a small number of reported cases of myocarditis and pericarditis following COVID-19 vaccination, primarily after the Pfizer-BioNTech vaccine. The exact number varies over time, but it remains rare compared to the millions of doses administered.
The risk of myocarditis following COVID-19 vaccination in New Zealand is very low. Studies and monitoring data indicate that the incidence is higher in younger males, particularly after the second dose, but it remains a rare adverse event.
New Zealand monitors vaccine-related adverse events through the Centre for Adverse Reactions Monitoring (CARM), which collects and analyzes reports from healthcare professionals and the public. Suspected cases of myocarditis are investigated, and data is regularly updated and shared with the public.
If you experience symptoms such as chest pain, shortness of breath, or abnormal heart rhythms after vaccination, seek medical attention immediately. Report the symptoms to your healthcare provider, who can then notify CARM for further investigation and monitoring.