As of recent data, a significant portion of the U.S. population remains unvaccinated against COVID-19, despite widespread availability of vaccines. According to the Centers for Disease Control and Prevention (CDC), approximately 20-25% of eligible Americans have not received a single dose, with disparities varying by age, geographic location, and socioeconomic factors. This unvaccinated group includes both those who are hesitant due to concerns about safety or efficacy and those who face barriers to access, such as lack of healthcare or misinformation. The persistence of this unvaccinated population continues to impact public health efforts, contributing to ongoing virus transmission and the emergence of new variants. Understanding the reasons behind vaccine hesitancy and addressing systemic challenges remain critical to increasing vaccination rates and achieving broader immunity nationwide.
Explore related products






What You'll Learn
- Unvaccinated by Age Group: Breakdown of unvaccinated individuals across different age groups in the United States
- Regional Vaccination Rates: Variations in vaccination rates across states and regions in the U.S
- Reasons for Refusal: Common reasons why some Americans choose not to get vaccinated
- Impact on Public Health: How unvaccinated populations affect disease spread and healthcare systems
- Vaccine Hesitancy Trends: Trends in vaccine hesitancy over time and demographic factors influencing it
![]()
Unvaccinated by Age Group: Breakdown of unvaccinated individuals across different age groups in the United States
As of recent data, the distribution of unvaccinated individuals in the United States varies significantly across different age groups. Understanding this breakdown is crucial for public health strategies aimed at increasing vaccination rates and addressing specific demographic challenges. The Centers for Disease Control and Prevention (CDC) and other health organizations provide insights into these disparities, highlighting areas where targeted interventions may be most effective.
Among children and adolescents, vaccination rates have historically been higher due to school immunization requirements. However, there remains a notable percentage of unvaccinated individuals in this age group. For children aged 5 to 11, approximately 20-30% remain unvaccinated against COVID-19, depending on the region. This figure is influenced by factors such as parental hesitancy, access to healthcare, and misinformation. Adolescents aged 12 to 17 show slightly higher vaccination rates, with around 15-25% remaining unvaccinated, though disparities persist based on geographic location and socioeconomic status.
In the young adult population, aged 18 to 29, vaccination rates begin to decline more significantly. Approximately 30-40% of individuals in this age group remain unvaccinated. This demographic often faces barriers such as lack of health insurance, mistrust of medical institutions, and lower perceived risk of severe illness. Additionally, the transient nature of this age group, often moving for education or work, can complicate consistent access to vaccination services.
Middle-aged adults, aged 30 to 49, exhibit a similar trend, with about 25-35% remaining unvaccinated. This group often includes parents and working professionals who may prioritize other responsibilities over vaccination. Economic instability, lack of paid time off for vaccine appointments, and persistent misinformation also contribute to lower vaccination rates in this demographic.
Among older adults, aged 50 and above, vaccination rates are generally higher due to increased awareness of health risks and stronger healthcare engagement. However, there is still a concerning percentage of unvaccinated individuals, particularly in the 50-64 age range, where about 20-25% remain unvaccinated. For those aged 65 and older, the rate drops to approximately 10-15%, as this group is more likely to have chronic conditions and a greater understanding of the risks associated with vaccine-preventable diseases.
Addressing the unvaccinated population across age groups requires tailored approaches. For younger individuals, education campaigns in schools and universities, as well as accessible vaccination clinics, can make a difference. For adults, workplace initiatives and community-based outreach programs are essential. Older adults may benefit from targeted messaging through healthcare providers and senior centers. By understanding the nuances of each age group, public health efforts can be more effective in reducing the number of unvaccinated individuals in the United States.
Childcare Vaccination Requirements: What You Need to Know
You may want to see also
Explore related products






![]()
Regional Vaccination Rates: Variations in vaccination rates across states and regions in the U.S
As of recent data, vaccination rates in the United States exhibit significant regional variations, influenced by factors such as political leanings, socioeconomic status, and access to healthcare. The Centers for Disease Control and Prevention (CDC) and other health organizations have highlighted disparities across states, with some regions achieving high vaccination coverage while others lag behind. For instance, states in the Northeast, such as Vermont and Massachusetts, consistently report some of the highest vaccination rates in the country, often exceeding 80% of eligible populations fully vaccinated. These states benefit from robust public health infrastructure, high healthcare access, and strong community engagement in health initiatives.
In contrast, Southern states like Mississippi, Alabama, and Louisiana often report lower vaccination rates, with some areas hovering below 50% fully vaccinated. These disparities are attributed to a combination of factors, including vaccine hesitancy, limited access to healthcare services, and lower levels of health literacy. Additionally, political and cultural attitudes toward vaccines play a significant role, as some communities in these regions express skepticism or resistance to vaccination campaigns. The rural-urban divide also contributes to these variations, with rural areas generally facing more challenges in vaccine distribution and uptake compared to urban centers.
Western states present a mixed picture, with states like California and Washington achieving relatively high vaccination rates, while others, such as Idaho and Wyoming, lag significantly. In California, targeted outreach programs and diverse vaccine distribution channels have helped boost vaccination numbers, particularly in urban areas. However, in more conservative or rural parts of the West, vaccine hesitancy and logistical barriers remain substantial obstacles. These regional differences underscore the need for tailored public health strategies that address local concerns and improve access to vaccines.
Midwestern states also show variability, with some, like Minnesota and Illinois, performing well in vaccination efforts, while others, such as North Dakota and Missouri, struggle to reach higher coverage levels. Economic factors, including poverty and lack of insurance, contribute to lower vaccination rates in certain areas. Furthermore, the Midwest’s diverse population, including significant rural communities and urban centers, requires multifaceted approaches to ensure equitable vaccine distribution and acceptance. Public health officials in these regions often emphasize community-based initiatives to build trust and combat misinformation.
Understanding these regional variations is crucial for addressing the issue of unvaccinated populations in the U.S. States with lower vaccination rates often correlate with higher numbers of unvaccinated individuals, posing risks not only to those communities but also to the nation’s overall public health. Targeted interventions, such as mobile vaccination clinics, localized public health messaging, and partnerships with community leaders, are essential to closing these gaps. By focusing on the specific needs and challenges of each region, policymakers and health organizations can work toward increasing vaccination rates and reducing disparities across the country.
Unvaccinated Kids in Schools: Policies, Risks, and Community Concerns
You may want to see also
Explore related products






![]()
Reasons for Refusal: Common reasons why some Americans choose not to get vaccinated
As of recent data, a significant portion of the U.S. population remains unvaccinated against COVID-19, with estimates suggesting that around 10-15% of adults have not received a single dose. This reluctance to get vaccinated is influenced by a variety of factors, ranging from personal beliefs to systemic issues. Understanding the reasons behind vaccine refusal is crucial for addressing public health concerns and improving vaccination rates. Below are some of the most common reasons why some Americans choose not to get vaccinated.
One of the primary reasons for vaccine refusal is mistrust in government and healthcare institutions. Historical events, such as the Tuskegee Syphilis Study, have left a lasting legacy of skepticism, particularly among minority communities. Additionally, misinformation and conspiracy theories spread through social media have further eroded trust in public health authorities. Many individuals believe that the government or pharmaceutical companies are withholding information about vaccine safety or using vaccines for ulterior motives, leading them to question the credibility of vaccination campaigns.
Concerns about vaccine safety and side effects also play a significant role in vaccine hesitancy. Despite extensive clinical trials and ongoing monitoring by health agencies, some Americans remain worried about potential long-term effects of the vaccines. High-profile reports of rare side effects, such as blood clots or myocarditis, have amplified these fears, even though the risks are extremely low compared to the dangers of COVID-19. Personal anecdotes shared within communities or online can further reinforce these concerns, making individuals hesitant to get vaccinated.
Another common reason for refusal is the belief in personal immunity or alternative health practices. Some people feel they are healthy enough to fight off COVID-19 without a vaccine, relying on their diet, exercise, or immune system. Others turn to alternative remedies, such as herbal supplements or homeopathic treatments, as substitutes for vaccination. This mindset often stems from a broader skepticism of conventional medicine and a preference for "natural" solutions, which can be deeply ingrained in an individual's lifestyle and beliefs.
Political and ideological factors have also polarized the vaccination debate in the U.S. For some, refusing the vaccine has become a statement of personal freedom or resistance to perceived government overreach. Political leaders and media personalities who question or criticize vaccination mandates have influenced their followers, framing the issue as one of individual rights rather than public health. This politicization has made vaccination a divisive topic, with some Americans viewing it as a symbol of political identity rather than a medical decision.
Finally, barriers to access and systemic issues contribute to lower vaccination rates in certain populations. While not a direct refusal, these obstacles effectively prevent individuals from getting vaccinated. These barriers include lack of transportation, limited access to healthcare facilities, and difficulty taking time off work for vaccination appointments. Additionally, language barriers and cultural differences can hinder outreach efforts, leaving some communities underserved. Addressing these systemic issues is essential for ensuring equitable access to vaccines and reducing the number of unvaccinated individuals.
In conclusion, the reasons for vaccine refusal in the U.S. are multifaceted, encompassing mistrust, safety concerns, personal beliefs, political ideologies, and systemic barriers. Addressing these issues requires a combination of transparent communication, community engagement, and policies that improve access to healthcare. By understanding and tackling these root causes, public health officials can work toward increasing vaccination rates and protecting the broader population.
Air Traffic Controllers: Vaccination Requirements and Protocols
You may want to see also
Explore related products






![]()
Impact on Public Health: How unvaccinated populations affect disease spread and healthcare systems
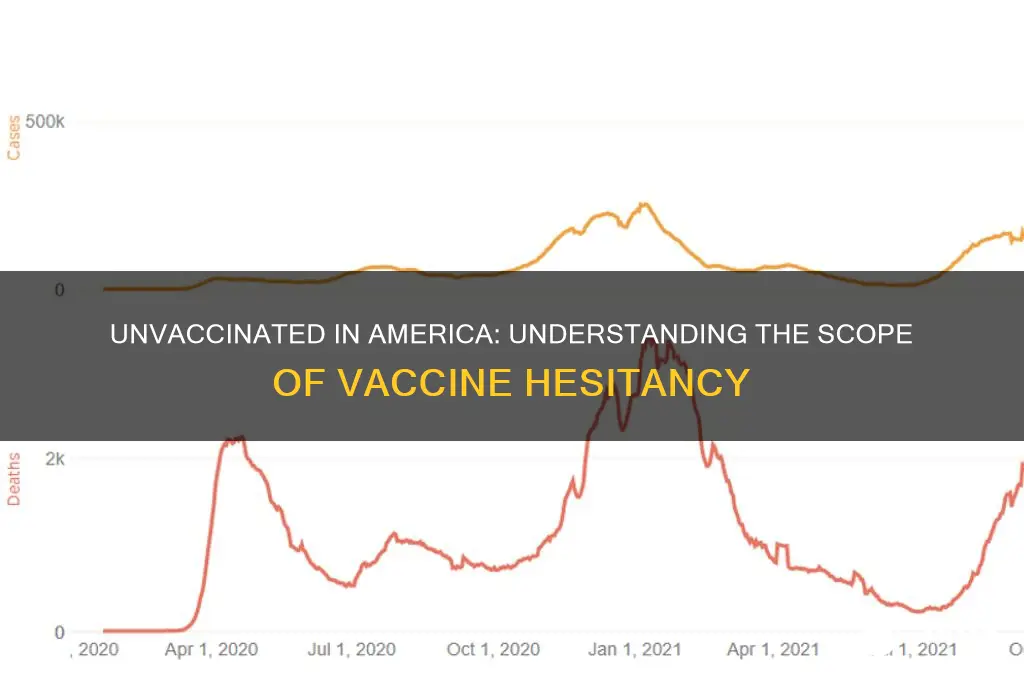
As of recent data, approximately 10-15% of the U.S. population remains unvaccinated against COVID-19, depending on the age group and region. This unvaccinated segment disproportionately contributes to the spread of infectious diseases, as they are more likely to contract and transmit pathogens. Vaccines not only protect individuals but also reduce the viral load and transmission rates within communities. When a significant portion of the population is unvaccinated, herd immunity is compromised, allowing diseases to circulate more freely. This is particularly concerning for highly contagious viruses like measles, influenza, and SARS-CoV-2, where even small unvaccinated clusters can sustain outbreaks.
The presence of unvaccinated populations places a substantial burden on healthcare systems. Unvaccinated individuals are at higher risk of severe illness, hospitalization, and death from vaccine-preventable diseases. During outbreaks, hospitals and clinics often face surges in patient numbers, leading to overcrowded emergency departments, delayed care for other conditions, and increased healthcare costs. For instance, COVID-19 surges driven by unvaccinated individuals have repeatedly strained hospital resources, forcing the cancellation of elective surgeries and overworking healthcare staff. This not only affects the unvaccinated but also jeopardizes care for those with unrelated medical needs.
Unvaccinated populations also contribute to the emergence of new variants, which can undermine vaccine efficacy and prolong pandemics. Viruses mutate more frequently in larger, susceptible populations, increasing the likelihood of variants that evade immunity or cause more severe disease. For example, the Delta and Omicron variants of SARS-CoV-2 emerged in contexts of uneven vaccination coverage, highlighting the global and local consequences of vaccine hesitancy. These variants can then spread to vaccinated individuals, reducing the overall effectiveness of public health measures and necessitating booster shots or new vaccines.
The impact of unvaccinated populations extends beyond immediate disease spread to long-term public health challenges. Vaccine-preventable diseases can lead to complications such as long COVID, heart damage, or neurological disorders, increasing the chronic disease burden on healthcare systems. Additionally, outbreaks in unvaccinated communities can disrupt schools, workplaces, and social services, causing economic and social instability. Public health efforts to control diseases become more resource-intensive, diverting funds from other critical areas like mental health, maternal care, or chronic disease management.
Addressing the impact of unvaccinated populations requires a multifaceted approach, including improving vaccine access, combating misinformation, and implementing targeted public health campaigns. Regions with lower vaccination rates often face barriers such as lack of healthcare infrastructure, distrust in medical institutions, or socioeconomic disparities. By focusing on equitable vaccine distribution and community engagement, public health officials can reduce disease transmission, alleviate strain on healthcare systems, and foster resilience against future pandemics. Ultimately, increasing vaccination rates is not just an individual health decision but a collective responsibility to protect public health and ensure the sustainability of healthcare systems.
Vaccinations: A Requirement for Adoption
You may want to see also
Explore related products






![]()
Vaccine Hesitancy Trends: Trends in vaccine hesitancy over time and demographic factors influencing it
Vaccine hesitancy in the United States has evolved significantly over time, influenced by a complex interplay of historical, social, and demographic factors. According to recent data, approximately 10-15% of the U.S. population remains unvaccinated against COVID-19, though this figure varies by region and demographic group. Historically, vaccine hesitancy has been present in the U.S. for decades, with concerns about vaccines dating back to the 19th century. However, the COVID-19 pandemic amplified these trends, as misinformation, political polarization, and distrust in institutions fueled skepticism. Over time, hesitancy has shifted from general anti-vaccine sentiment to more targeted concerns about specific vaccines, such as those for COVID-19 or childhood diseases like measles. Understanding these trends is crucial for addressing public health challenges and improving vaccination rates.
Demographic factors play a significant role in shaping vaccine hesitancy. Age is a notable influencer, with younger adults (18-29 years) often expressing higher levels of skepticism compared to older populations, who generally trust vaccines more due to their experiences with vaccine-preventable diseases. Education level is another critical factor; individuals with lower educational attainment are more likely to be hesitant, possibly due to limited access to reliable health information. Geographic location also matters, as rural areas tend to report higher rates of vaccine hesitancy compared to urban centers, often linked to differences in healthcare access and community norms. These demographic disparities highlight the need for tailored public health strategies to address specific concerns within different population groups.
Political affiliation has emerged as a powerful determinant of vaccine hesitancy, particularly during the COVID-19 pandemic. Surveys consistently show that individuals identifying as politically conservative are more likely to be unvaccinated compared to their liberal counterparts. This divide is often exacerbated by partisan media narratives and conflicting messages from political leaders. Additionally, racial and ethnic minorities, such as Black and Hispanic communities, initially reported higher hesitancy rates, driven by historical medical mistrust and systemic inequities in healthcare. However, targeted outreach efforts have helped reduce these gaps over time, demonstrating the importance of culturally sensitive communication in building trust.
Over time, vaccine hesitancy has been influenced by the rise of social media and the spread of misinformation. Platforms like Facebook, Twitter, and YouTube have become breeding grounds for false claims about vaccine safety and efficacy, reaching millions of users. This digital landscape has made it challenging for public health officials to combat misinformation effectively. Trends also show that hesitancy can fluctuate in response to specific events, such as the rollout of new vaccines or reports of rare side effects. For instance, the temporary pause of the Johnson & Johnson COVID-19 vaccine in 2021 led to increased skepticism, even though the pause demonstrated regulatory vigilance. Monitoring these shifts is essential for developing responsive public health messaging.
Addressing vaccine hesitancy requires a multifaceted approach that considers both historical trends and current demographic factors. Public health campaigns must focus on building trust through transparent communication, engaging community leaders, and leveraging data to dispel myths. Tailored interventions for specific demographic groups, such as educational workshops in rural areas or culturally relevant materials for minority communities, can be particularly effective. Policymakers and healthcare providers must also work to reduce systemic barriers to vaccination, such as improving access in underserved areas. By understanding the evolving trends and underlying influences of vaccine hesitancy, the U.S. can make strides in increasing vaccination rates and protecting public health.
Protecting Newborns: How Sibling Vaccines Shield Against Hib Infections
You may want to see also
Frequently asked questions
As of recent data, approximately 10-15% of the eligible U.S. population remains unvaccinated against COVID-19, though this percentage varies by age group and region.
Around 10-12% of U.S. adults (aged 18 and older) have not received any COVID-19 vaccine doses, according to the Centers for Disease Control and Prevention (CDC).
Among children aged 5-11 and 12-17, vaccination rates are lower, with approximately 30-40% remaining unvaccinated, depending on the age group and location.
Yes, vaccination rates vary significantly by state. States with lower vaccination rates, such as Mississippi, Alabama, and Wyoming, have higher percentages of unvaccinated individuals, while states like Vermont and Massachusetts have lower unvaccinated populations.