As of the latest data from the Centers for Disease Control and Prevention (CDC), a significant portion of the U.S. population has received COVID-19 vaccinations, marking a critical milestone in the nation’s public health response to the pandemic. The CDC’s vaccination tracker provides real-time updates on the number of Americans who have completed their primary vaccine series, received booster doses, and are fully vaccinated, offering insights into regional disparities and demographic trends. Understanding these figures is essential for assessing the country’s progress in achieving herd immunity, reducing hospitalizations, and mitigating the spread of the virus, while also highlighting areas where vaccination efforts may need to be intensified.
Explore related products






What You'll Learn
![]()
Vaccination Rates by Age Group
As of the latest CDC data, vaccination rates in the U.S. vary significantly by age group, reflecting both generational attitudes and public health priorities. Among adults aged 65 and older, over 90% have received at least one dose of a COVID-19 vaccine, a testament to targeted campaigns emphasizing their vulnerability to severe outcomes. In contrast, adolescents aged 12–17 lag behind, with only about 60% fully vaccinated, despite eligibility since mid-2021. This disparity highlights the challenges of engaging younger populations, who often perceive lower personal risk.
Analyzing these trends reveals a clear correlation between age and vaccination acceptance. For instance, the 18–29 age group hovers around 65% fully vaccinated, a rate influenced by factors like misinformation, lower perceived risk, and logistical barriers. Meanwhile, the 50–64 age group surpasses 80%, benefiting from both heightened awareness of health risks and easier access to vaccination sites. These patterns underscore the need for age-specific strategies, such as school-based clinics for teens or workplace incentives for young adults, to bridge these gaps.
From a practical standpoint, parents and caregivers can play a pivotal role in boosting adolescent vaccination rates. Scheduling vaccine appointments alongside routine check-ups or sports physicals can streamline the process. Additionally, leveraging peer influence—such as hosting vaccination drives at schools or community centers—may encourage participation. For older adults, ensuring access to booster doses remains critical, as immunity wanes over time. The CDC recommends a second booster for those over 50, yet only about 30% have received it, indicating a need for clearer communication and outreach.
Comparatively, the success in vaccinating seniors offers lessons for other age groups. Early prioritization, coupled with messaging tailored to their concerns about comorbidities, proved effective. Applying this model to younger demographics requires addressing their unique barriers. For example, debunking myths through trusted influencers or providing flexible vaccination hours could resonate with busy young adults. Similarly, framing vaccination as a step toward normalcy—like attending mask-free events—might appeal to teens.
In conclusion, understanding vaccination rates by age group is essential for refining public health strategies. While older Americans have largely embraced vaccination, younger groups require targeted, innovative approaches. By combining data-driven insights with practical solutions, we can move closer to equitable protection across all ages. The CDC’s role in monitoring these trends and adapting guidance remains vital, but community-level action is equally indispensable.
Andrew Pollard's Role in Technical Advisory Group on Salmonella Vaccines
You may want to see also
Explore related products

$11.93 $21.99



$9.99 $9.99


![]()
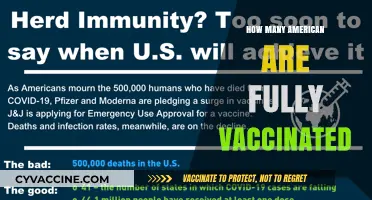
State-by-State Vaccination Coverage
As of the latest CDC data, vaccination coverage varies significantly across the United States, with some states boasting high rates of fully vaccinated individuals while others lag behind. This disparity raises questions about the factors influencing vaccine uptake, from regional demographics to local public health initiatives. For instance, states like Vermont and Massachusetts consistently report vaccination rates above 75% for adults, whereas states like Mississippi and Alabama often fall below 50%. Understanding these variations is crucial for tailoring strategies to improve overall national coverage.
Analyzing the data reveals that urban areas tend to have higher vaccination rates compared to rural regions, likely due to better access to healthcare facilities and higher population density. However, this trend isn’t universal. Some rural states, such as Maine, have achieved impressive vaccination rates by implementing mobile clinics and community outreach programs. Conversely, even in highly urbanized states like New York, certain neighborhoods show lower coverage, highlighting the need for targeted interventions. Age also plays a significant role, with older adults generally more vaccinated than younger populations, though recent campaigns have narrowed this gap in some states.
To improve state-by-state vaccination coverage, public health officials can adopt a multi-pronged approach. First, identify underserved areas using CDC data and allocate resources accordingly. For example, deploying pop-up vaccination sites in rural counties or low-income neighborhoods can increase accessibility. Second, leverage local leaders and trusted community figures to address vaccine hesitancy, as seen in successful campaigns in Colorado and Minnesota. Third, simplify the vaccination process by offering flexible hours, walk-in options, and multilingual services to cater to diverse populations.
A comparative analysis of high-performing states offers valuable lessons. Vermont, for instance, achieved its top vaccination rate by integrating vaccine appointments into existing healthcare visits and partnering with pharmacies. In contrast, California’s success stems from its robust digital registration system and extensive public awareness campaigns. Meanwhile, states struggling with coverage, like Wyoming, could benefit from adopting similar strategies while addressing unique local challenges, such as geographic isolation or cultural barriers.
Practical tips for individuals navigating state-specific vaccination efforts include checking local health department websites for updated clinic locations and eligibility criteria. For parents, ensuring children receive their full vaccine series—typically two doses for COVID-19 and additional boosters as recommended—is essential. Adults should stay informed about booster requirements, as these vary by state and age group. Finally, participating in community health fairs or employer-sponsored vaccination drives can provide convenient opportunities to get vaccinated while supporting broader public health goals.
Why Vaccines Skip Placebo Testing: Ethical and Scientific Insights
You may want to see also
Explore related products






![]()
Booster Shot Uptake Statistics
As of the latest CDC data, booster shot uptake among Americans has plateaued, with only 48% of eligible individuals having received their first booster dose. This statistic is particularly concerning given the evolving nature of COVID-19 variants and the waning immunity from initial vaccine series. The disparity in uptake is even more pronounced when broken down by age groups: while 67% of seniors aged 65 and older have received a booster, only 28% of adults aged 18-49 have done so. This gap highlights the urgent need for targeted public health campaigns to address hesitancy and accessibility issues in younger populations.
Analyzing the data further, geographic trends reveal significant variations in booster uptake. States with higher vaccination rates, such as Vermont and Massachusetts, also lead in booster administration, with rates exceeding 60%. In contrast, states like Mississippi and Alabama lag behind, with booster rates below 30%. These disparities underscore the influence of local policies, healthcare infrastructure, and community attitudes on vaccination behaviors. For instance, states with robust public health systems and proactive outreach programs tend to outperform those with limited resources or political resistance to vaccination efforts.
From a practical standpoint, understanding booster shot uptake requires addressing common barriers to access. Many Americans remain unsure about when or how to get a booster, despite CDC guidelines recommending an additional dose 5 months after the initial series for Pfizer and Moderna, or 2 months after Johnson & Johnson. To improve uptake, healthcare providers should proactively notify eligible patients via text, email, or phone calls, and offer flexible scheduling options, including mobile clinics and workplace vaccination drives. Additionally, debunking misinformation about booster safety and efficacy remains critical, as surveys indicate that 30% of unvaccinated individuals cite concerns about side effects or long-term risks as reasons for avoiding boosters.
Comparatively, booster uptake in the U.S. trails behind countries like Canada and the U.K., where over 60% of eligible populations have received additional doses. This discrepancy can be attributed to differences in messaging, policy enforcement, and public trust in health authorities. For example, Canada’s centralized healthcare system facilitated rapid booster distribution, while the U.K.’s clear, consistent messaging about the benefits of boosters helped maintain public confidence. The U.S. could learn from these examples by streamlining communication strategies and fostering partnerships between federal, state, and local health agencies to ensure a unified approach to booster promotion.
Ultimately, increasing booster shot uptake requires a multifaceted strategy that combines data-driven insights with actionable solutions. Employers can play a pivotal role by offering paid time off for vaccination and hosting on-site clinics. Schools and universities should mandate boosters for students and staff, mirroring successful flu vaccine policies. For individuals, staying informed about evolving CDC recommendations and discussing concerns with trusted healthcare providers can alleviate uncertainty. By addressing access, awareness, and hesitancy, the U.S. can bridge the booster gap and enhance collective immunity against COVID-19.
Maryland Vaccine Scheduling: A Step-by-Step Guide to Book Your Appointment
You may want to see also
Explore related products






![]()
Vaccine Hesitancy Demographics
As of the latest CDC data, approximately 67% of the U.S. population is fully vaccinated against COVID-19, but this figure masks significant disparities across demographic groups. Vaccine hesitancy, defined as delay in acceptance or refusal of vaccines despite availability, varies widely by age, race, education, and geographic location. Understanding these demographics is crucial for tailoring public health strategies to increase vaccination rates.
Age and Vaccine Hesitancy: Younger adults, particularly those aged 18–29, exhibit higher rates of vaccine hesitancy compared to older populations. CDC surveys reveal that only 55% of this age group is fully vaccinated, compared to 85% of adults over 65. This disparity may stem from differing perceptions of COVID-19 risk; younger individuals often feel less vulnerable to severe illness. Public health campaigns targeting this demographic should emphasize long-term health benefits, such as reduced risk of myocarditis from vaccination versus infection, and the role of vaccination in protecting vulnerable community members.
Racial and Ethnic Disparities: Vaccine hesitancy also varies by race and ethnicity. Black and Hispanic communities initially faced lower vaccination rates due to historical medical mistrust and systemic barriers like limited access to healthcare. However, targeted outreach efforts, including community-based vaccination clinics and partnerships with trusted leaders, have narrowed these gaps. For example, Hispanic vaccination rates have risen to 63%, while Black vaccination rates stand at 59%, according to recent CDC data. Sustaining these gains requires continued investment in culturally sensitive messaging and addressing structural inequities in healthcare access.
Education and Geographic Factors: Education level and geographic location are strong predictors of vaccine hesitancy. Individuals with lower educational attainment and those living in rural areas are less likely to be vaccinated. Only 58% of adults without a college degree are fully vaccinated, compared to 82% of college graduates. Rural counties report vaccination rates 10–15 percentage points lower than urban areas, partly due to misinformation spread and fewer healthcare resources. Strategies to address this include leveraging local pharmacies for vaccine distribution, combating misinformation through trusted sources like primary care providers, and offering incentives such as gift cards or paid time off for vaccination.
Practical Steps to Reduce Hesitancy: To effectively address vaccine hesitancy across these demographics, public health initiatives must be data-driven and context-specific. For younger adults, social media campaigns featuring peers discussing vaccine benefits can be impactful. In racially diverse communities, partnering with churches or community centers for vaccination drives builds trust. For rural populations, mobile clinics and partnerships with agricultural employers can improve access. Additionally, addressing misinformation requires clear, consistent messaging from healthcare professionals, emphasizing vaccine safety and efficacy backed by clinical trial data, such as the 95% efficacy rate of the Pfizer-BioNTech vaccine after two doses.
By dissecting vaccine hesitancy demographics, public health officials can design interventions that resonate with specific groups, ultimately moving the needle on national vaccination rates. The goal is not just to inform but to empower individuals to make decisions that protect their health and that of their communities.
Vaccines: How They Curb Disease Spread and Protect Communities
You may want to see also
Explore related products






![]()
CDC Data Collection Methods
The CDC's vaccination data is a critical tool for public health officials, but its accuracy depends on robust data collection methods. One key approach is the Immunization Information System (IIS), a confidential, population-based, computerized database that records all immunization doses administered by participating providers. These systems, operated by state and local health departments, capture data from public and private healthcare providers, pharmacies, and schools. For instance, when a 65-year-old receives their second dose of the Pfizer-BioNTech COVID-19 vaccine, the provider enters this information into the IIS, which then aggregates it for CDC analysis. This method ensures real-time tracking but relies on provider compliance and system interoperability.
Another vital method is the National Immunization Survey (NIS), a household survey that collects vaccination data directly from parents or guardians of children aged 19–35 months. Conducted via telephone interviews, the NIS also verifies vaccination records from healthcare providers. For example, if a parent reports their child received the full series of MMR (measles, mumps, rubella) vaccines, the CDC cross-references this with the child’s medical records. This dual approach minimizes recall bias and provides a more accurate picture of childhood vaccination rates. However, the NIS does not cover adults, leaving a gap in data for older age groups.
The CDC also leverages pharmacy and healthcare provider reporting, particularly for adult vaccinations. Pharmacies, which administer a significant portion of flu and COVID-19 vaccines, submit data through systems like the Vaccine Administration Management System (VAMS). For instance, a pharmacist administering a 30-microgram dose of the Moderna COVID-19 booster logs the recipient’s age, dose date, and vaccine type. While this method is efficient, it can miss doses given by non-reporting providers or those administered outside traditional healthcare settings, such as workplace clinics.
A comparative analysis reveals that each method has strengths and limitations. IIS provides comprehensive, provider-level data but is vulnerable to underreporting. NIS offers verified, population-level insights for young children but excludes adults. Pharmacy reporting captures adult vaccinations but may overlook doses given by non-pharmacy providers. To address these gaps, the CDC employs data triangulation, combining multiple sources to validate findings. For example, COVID-19 vaccination rates are cross-checked using IIS, pharmacy data, and self-reported surveys like the Census Bureau’s Household Pulse Survey. This layered approach enhances accuracy but requires careful harmonization of disparate datasets.
Practical tips for healthcare providers and policymakers include ensuring timely data submission to IIS, participating in NIS verification requests, and promoting standardized reporting across all vaccination sites. For the public, understanding these methods underscores the importance of accurate record-keeping and participation in surveys. By refining these data collection strategies, the CDC can provide more reliable estimates of vaccination coverage, guiding targeted interventions to close immunization gaps.
Vaccination Requirements for Hospital Visits: What You Need to Know
You may want to see also
Frequently asked questions
As of the latest CDC data, over 270 million Americans have received at least one dose of a COVID-19 vaccine.
The CDC reports that approximately 68% of the total U.S. population is fully vaccinated against COVID-19.
The CDC indicates that over 110 million Americans have received a COVID-19 booster dose.
The CDC reports that approximately 30% of children aged 5-11 in the U.S. have completed their primary COVID-19 vaccination series.
The CDC tracks COVID-19 vaccination rates through its Immunization Information Systems (IIS), vaccine provider reports, and other data sources, breaking it down by state, age, race, and ethnicity.