As of recent data, the number of Americans who have been vaccinated against COVID-19 continues to be a critical indicator of public health progress in the United States. According to the Centers for Disease Control and Prevention (CDC), over 220 million individuals have received at least one dose of a COVID-19 vaccine, with more than 205 million fully vaccinated. Additionally, booster shots have been administered to over 100 million people, reflecting ongoing efforts to enhance immunity and protect against emerging variants. These figures highlight the significant strides made in vaccination campaigns, though disparities in access and hesitancy persist across demographic and geographic lines. Understanding these numbers is essential for assessing the nation’s resilience against the pandemic and guiding future public health strategies.
Explore related products


$2.96 $24.95




What You'll Learn
- Vaccination Rates by State: Compare vaccination percentages across different U.S. states and territories
- Age Group Vaccination Trends: Analyze vaccination rates among various age groups in America
- Vaccine Type Distribution: Breakdown of Americans vaccinated by vaccine brand (Pfizer, Moderna, etc.)
- Urban vs. Rural Vaccination: Compare vaccination rates in urban and rural areas of the U.S
- Vaccination by Demographics: Examine vaccination rates by race, ethnicity, and socioeconomic status in America
![]()
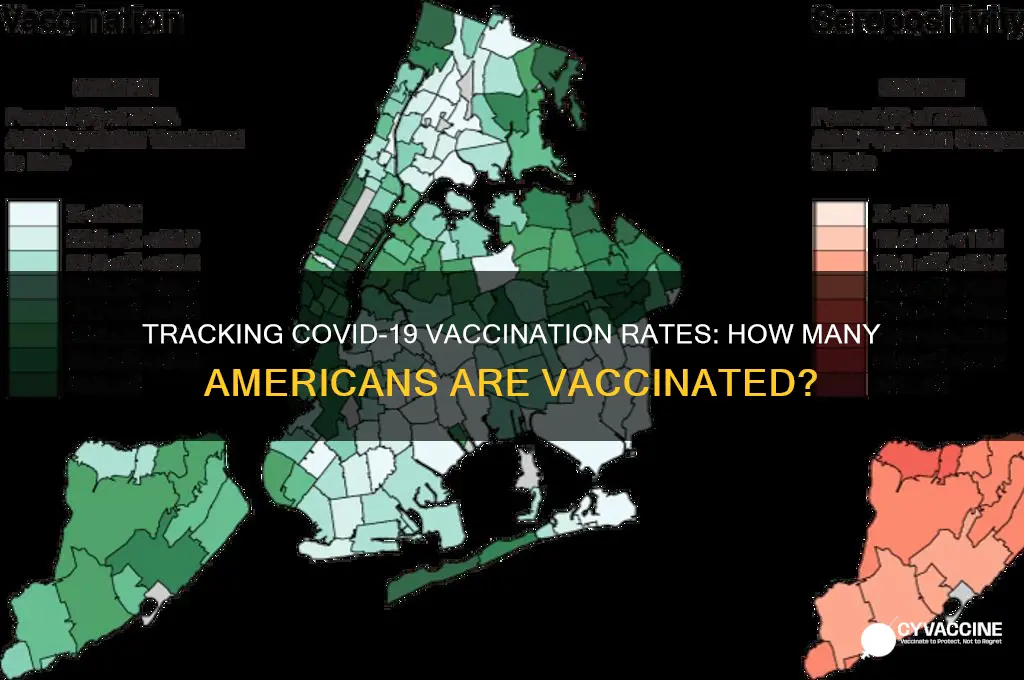
Vaccination Rates by State: Compare vaccination percentages across different U.S. states and territories
As of the latest data, vaccination rates across U.S. states and territories reveal stark disparities, with some regions achieving near-herd immunity levels while others lag significantly behind. For instance, Vermont leads the nation with over 78% of its population fully vaccinated, a testament to robust public health campaigns and high community engagement. In contrast, states like Mississippi and Alabama report rates below 50%, highlighting persistent challenges in access, misinformation, and vaccine hesitancy. These variations underscore the importance of localized strategies to address unique barriers in each state.
Analyzing these differences, several factors emerge as key drivers of vaccination rates. States with higher education levels and urban populations, such as Massachusetts and Connecticut, consistently outperform rural states like Wyoming and Idaho. Additionally, political leanings play a role, as evidenced by lower vaccination rates in predominantly conservative states. Public health experts emphasize the need for tailored messaging and community-based initiatives to bridge these gaps. For example, mobile clinics and partnerships with local leaders have proven effective in increasing uptake in underserved areas.
To compare vaccination percentages effectively, consider the following steps: first, examine CDC data or state health department reports for up-to-date figures. Second, account for demographic differences, such as age distribution, as states with older populations may have higher vaccination rates due to prioritized rollouts. Third, look beyond fully vaccinated numbers to include booster doses, as these provide critical protection against variants. For instance, while California boasts a high initial vaccination rate, its booster uptake lags, leaving millions vulnerable to breakthrough infections.
A persuasive argument for addressing these disparities lies in the economic and social benefits of higher vaccination rates. States with higher vaccination levels, like New Hampshire and Maine, have seen faster economic recoveries and fewer hospitalizations, reducing strain on healthcare systems. Conversely, low-vaccination states face prolonged outbreaks and higher healthcare costs. Policymakers can incentivize vaccination by offering tax breaks or grants to communities that achieve specific milestones, as seen in Ohio’s vaccine lottery program, which temporarily boosted participation.
Finally, a descriptive snapshot of territorial vaccination rates reveals unique challenges. Puerto Rico, with its well-established healthcare infrastructure, has vaccinated over 70% of its population, outpacing many mainland states. In contrast, American Samoa and the U.S. Virgin Islands struggle with limited resources and geographic isolation, resulting in rates below 50%. These territories require targeted federal support, including increased vaccine supply and logistical assistance, to overcome their distinct obstacles. By understanding these variations, stakeholders can craft more effective strategies to ensure equitable protection nationwide.
Pharmacy Vaccination Registration: A Step-by-Step Location Sign-Up Guide
You may want to see also
Explore related products

$18.99 $18.99





![]()
Age Group Vaccination Trends: Analyze vaccination rates among various age groups in America
As of recent data, vaccination rates in the United States vary significantly across age groups, reflecting both demographic priorities and societal behaviors. The Centers for Disease Control and Prevention (CDC) reports that individuals aged 65 and older have achieved the highest vaccination rates, with over 90% receiving at least one dose. This success is attributed to early vaccine rollouts targeting seniors due to their heightened vulnerability to severe illness. Conversely, adolescents aged 12–17 show lower uptake, with approximately 60% fully vaccinated, despite eligibility for Pfizer’s two-dose regimen since May 2021. This disparity highlights the need for targeted outreach in younger populations.
Analyzing these trends reveals a clear correlation between age and vaccine hesitancy. Adults aged 18–29, often perceived as low-risk, exhibit vaccination rates around 70%, influenced by factors like misinformation, logistical barriers, and a sense of invulnerability. In contrast, the 30–49 age group, balancing work and family responsibilities, shows rates closer to 80%, possibly driven by workplace mandates or family health concerns. Public health campaigns must address these age-specific barriers, such as offering evening or weekend vaccination clinics for busy parents or debunking myths targeting younger adults.
A comparative approach underscores the impact of policy and messaging. For instance, school-based vaccination drives have modestly improved adolescent rates, but their effectiveness pales compared to senior outreach programs. Similarly, while booster doses are recommended for all adults, uptake drops sharply below age 50, with only 40% of 18–49-year-olds receiving a booster. This suggests that messaging emphasizing long-term protection and community immunity could resonate more strongly with younger adults than mandates alone.
To bridge these gaps, practical strategies should focus on accessibility and education. For adolescents, integrating vaccine information into school curricula or partnering with social media influencers could normalize vaccination. Employers can incentivize younger workers with paid time off for vaccination appointments. For seniors, maintaining mobile clinics and home visits ensures continued high participation. By tailoring approaches to each age group’s needs and behaviors, public health efforts can achieve more equitable vaccination coverage nationwide.
Should You Vaccinate Your Cat? Essential Health Considerations for Pet Owners
You may want to see also
Explore related products






![]()
Vaccine Type Distribution: Breakdown of Americans vaccinated by vaccine brand (Pfizer, Moderna, etc.)
As of recent data, the distribution of COVID-19 vaccines among Americans reveals a clear dominance by Pfizer-BioNTech, followed by Moderna and Johnson & Johnson (J&J). Pfizer’s vaccine accounts for approximately 60% of all doses administered, with Moderna trailing at around 35%, and J&J making up the remaining 5%. This disparity is partly due to Pfizer’s earlier approval for broader age groups, including children as young as 6 months, while Moderna was initially limited to adults. Additionally, Pfizer’s lower dosage for pediatric populations (10 micrograms for ages 5-11, compared to 30 micrograms for adults) has made it a preferred choice for families. Understanding these brand-specific uptake rates is critical for public health planning, as it influences booster campaigns, vaccine supply chains, and efforts to address hesitancy among specific demographics.
For those navigating vaccine choices, the brand distribution highlights practical considerations. Pfizer’s two-dose primary series (3 weeks apart for adults, 3-8 weeks for children) and Moderna’s similar regimen (4 weeks apart) are both mRNA vaccines, offering high efficacy against severe disease. However, Moderna’s slightly higher dosage (100 micrograms per shot vs. Pfizer’s 30 micrograms) has been associated with marginally higher efficacy in some studies but also slightly more frequent side effects, such as fatigue or fever. Johnson & Johnson’s single-dose adenovirus-based vaccine remains a convenient option for individuals seeking a one-and-done approach, though its use has been limited due to rare blood clot risks and lower overall efficacy compared to mRNA vaccines.
A comparative analysis of vaccine distribution by age group further illuminates brand preferences. Among children aged 5-11, Pfizer holds a near-monopoly, as it was the first and, for a long time, the only vaccine approved for this age group. In contrast, Moderna’s recent approval for ages 6-17 has yet to significantly shift this dynamic. For adults, Pfizer and Moderna are nearly equally preferred, though Moderna’s slightly higher efficacy in younger adults (ages 18-64) has made it a popular choice in this demographic. J&J’s usage is most prominent among older adults who prioritize convenience or have mRNA contraindications, despite its lower efficacy and safety concerns.
From a public health perspective, the uneven distribution of vaccine brands underscores the need for tailored communication strategies. For instance, addressing hesitancy around J&J’s safety profile requires transparent messaging about its rare side effects and the benefits of a single-dose option. Similarly, promoting Moderna’s recent approval for younger age groups could help balance uptake and reduce supply pressures on Pfizer. Clinicians and policymakers should also consider brand-specific dosing intervals and storage requirements—Pfizer’s ultra-cold storage needs initially posed logistical challenges, while Moderna’s slightly less stringent requirements made it more accessible in rural areas.
In conclusion, the breakdown of Americans vaccinated by brand is not just a statistical curiosity but a practical guide for individuals and policymakers alike. Whether you’re a parent deciding between Pfizer and Moderna for your child, an adult weighing the pros and cons of J&J’s single dose, or a health official planning booster campaigns, understanding these distribution patterns is essential. By considering factors like age, dosage, efficacy, and logistical feasibility, stakeholders can make informed decisions that maximize vaccine coverage and protect public health.
Brigham and Women's Hospital: Available Vaccines and Immunization Services
You may want to see also
Explore related products






![]()
Urban vs. Rural Vaccination: Compare vaccination rates in urban and rural areas of the U.S
As of recent data, approximately 67% of the U.S. population has received at least one dose of a COVID-19 vaccine, with urban areas consistently outpacing rural regions. This disparity highlights a critical divide in public health outcomes, influenced by factors such as access to healthcare, socioeconomic status, and community attitudes toward vaccination. Urban centers, with their higher population densities and greater availability of vaccination sites, have achieved vaccination rates often exceeding 75%. In contrast, rural areas, where healthcare infrastructure is limited and skepticism about vaccines can run deeper, lag behind, with rates frequently below 50%.
Analytical Perspective:
The gap in vaccination rates between urban and rural areas is not merely a numbers game but a reflection of systemic inequalities. Urban residents benefit from proximity to hospitals, pharmacies, and mass vaccination sites, often accessible via public transportation. Rural communities, however, face challenges such as long travel distances, fewer healthcare providers, and limited operational hours for vaccination clinics. Additionally, rural populations tend to be older and more reliant on Medicare or Medicaid, which may not cover all vaccine-related services equally. Addressing this disparity requires targeted solutions, such as mobile vaccination units and partnerships with local clinics, to bridge the accessibility gap.
Instructive Approach:
To improve vaccination rates in rural areas, public health officials should focus on three key strategies. First, establish pop-up clinics in underserved communities, leveraging schools, churches, and community centers as vaccination sites. Second, deploy mobile units equipped with vaccines and trained staff to reach remote areas. Third, engage trusted local leaders, such as clergy or farmers, to disseminate accurate information and combat misinformation. For urban areas, the focus should shift to reaching hesitant populations through culturally tailored campaigns and offering incentives like gift cards or free transportation to vaccination sites.
Comparative Insight:
Consider the case of two counties: one urban, with a population of 500,000, and one rural, with 50,000 residents. The urban county has 10 vaccination sites, while the rural county has only one. Despite similar vaccine allocations per capita, the urban county vaccinates 70% of its population within six months, compared to just 40% in the rural county. This disparity underscores the inefficiency of a one-size-fits-all approach. Rural areas require decentralized, community-specific strategies, whereas urban areas benefit from high-volume, centralized efforts.
Persuasive Argument:
Closing the urban-rural vaccination gap is not just a moral imperative but a public health necessity. Unvaccinated rural populations serve as reservoirs for virus transmission, prolonging the pandemic and increasing the risk of new variants. By investing in rural vaccination efforts, we not only protect these communities but also safeguard the entire nation. Policymakers must prioritize funding for rural healthcare infrastructure and incentivize healthcare providers to serve in these areas. Without such action, the divide will persist, leaving millions vulnerable and hindering our collective recovery.
Practical Tips:
For rural residents seeking vaccination, check local health department websites for mobile clinic schedules or call 211 for assistance. Urban dwellers can use apps like VaccineFinder to locate nearby sites and book appointments. Regardless of location, everyone should verify insurance coverage for booster shots, as eligibility and costs may vary. Finally, share reliable vaccine information with friends and family to counter misinformation and encourage uptake across all communities.
Vaccine Mandates: Domestic Air Travel Requirements
You may want to see also
Explore related products


$18.79 $20.99

$61.65 $119.99



![]()
Vaccination by Demographics: Examine vaccination rates by race, ethnicity, and socioeconomic status in America
As of recent data, over 260 million Americans have received at least one dose of a COVID-19 vaccine, yet vaccination rates are not uniform across demographic groups. Disparities in vaccination coverage persist, particularly when examining data by race, ethnicity, and socioeconomic status. For instance, while 72% of Asian Americans and 60% of White Americans are fully vaccinated, only 54% of Hispanic and 50% of Black Americans have reached the same milestone. These gaps highlight systemic inequalities that extend beyond individual choice, underscoring the need for targeted interventions.
Consider the role of socioeconomic status in shaping vaccination access. Individuals in lower-income brackets often face barriers such as limited transportation, inflexible work schedules, and reduced access to healthcare providers. For example, only 45% of Americans earning less than $25,000 annually are fully vaccinated, compared to 78% of those earning over $75,000. Practical solutions include mobile vaccination clinics in underserved neighborhoods, paid time off for vaccine appointments, and multilingual outreach campaigns. Employers and policymakers must collaborate to remove these logistical hurdles, ensuring equitable access regardless of income level.
Race and ethnicity intersect with socioeconomic factors to create complex barriers to vaccination. Black and Hispanic communities, historically marginalized in healthcare, report higher levels of vaccine hesitancy due to mistrust rooted in experiences like the Tuskegee Syphilis Study. However, when culturally sensitive messaging is employed—such as campaigns led by trusted community figures—uptake improves. For instance, a Philadelphia initiative featuring local Black healthcare workers increased vaccination rates by 15% in targeted neighborhoods. This demonstrates the power of tailored approaches in bridging trust gaps and addressing systemic disparities.
Age-specific trends further complicate the demographic landscape. While 85% of seniors (65+) are fully vaccinated, only 60% of adults aged 18-29 have completed their primary series. Young adults, particularly those from minority backgrounds, often underestimate their risk or face misinformation on social media. To counter this, public health efforts should leverage digital platforms with factual, engaging content and partner with influencers who resonate with younger audiences. Additionally, integrating vaccine education into school curricula can foster long-term health literacy and reduce disparities in future generations.
Ultimately, closing the vaccination gap requires a multifaceted strategy that acknowledges the unique challenges faced by different demographic groups. Data-driven policies, community engagement, and structural reforms are essential to ensure that vaccination rates reflect equity, not inequality. By addressing barriers related to race, ethnicity, and socioeconomic status, America can move closer to achieving herd immunity and protecting its most vulnerable populations.
Daycare and Vaccine Exemptions: What's the Deal?
You may want to see also
Frequently asked questions
As of 2023, over 220 million Americans have been fully vaccinated against COVID-19, representing approximately 67% of the total population.
Approximately 92% of the U.S. adult population has received at least one dose of a COVID-19 vaccine as of recent data.
Over 100 million Americans have received at least one COVID-19 booster shot, though uptake varies by age group and region.