The vaccination of children aged 5 to 11 has been a critical focus in the global effort to control the COVID-19 pandemic, as it helps reduce transmission, protect vulnerable populations, and maintain in-person learning. Since the approval of vaccines for this age group by health authorities such as the FDA and WHO, many countries have rolled out vaccination campaigns targeting younger children. However, the uptake varies widely due to factors like parental hesitancy, accessibility, and regional health policies. Understanding how many children in this age group have been vaccinated provides valuable insights into the progress of public health initiatives and the challenges that remain in achieving widespread immunity.
Explore related products






What You'll Learn
- Vaccination Rates by Country: Global 5-11 age group COVID-19 vaccination coverage statistics
- Vaccine Types Used: Approved vaccines for children aged 5-11 worldwide
- Side Effects Data: Common side effects reported in vaccinated 5-11-year-olds
- Efficacy Studies: Research on vaccine effectiveness in the 5-11 age group
- Parental Hesitancy: Factors influencing parents' decisions to vaccinate children aged 5-11
![]()
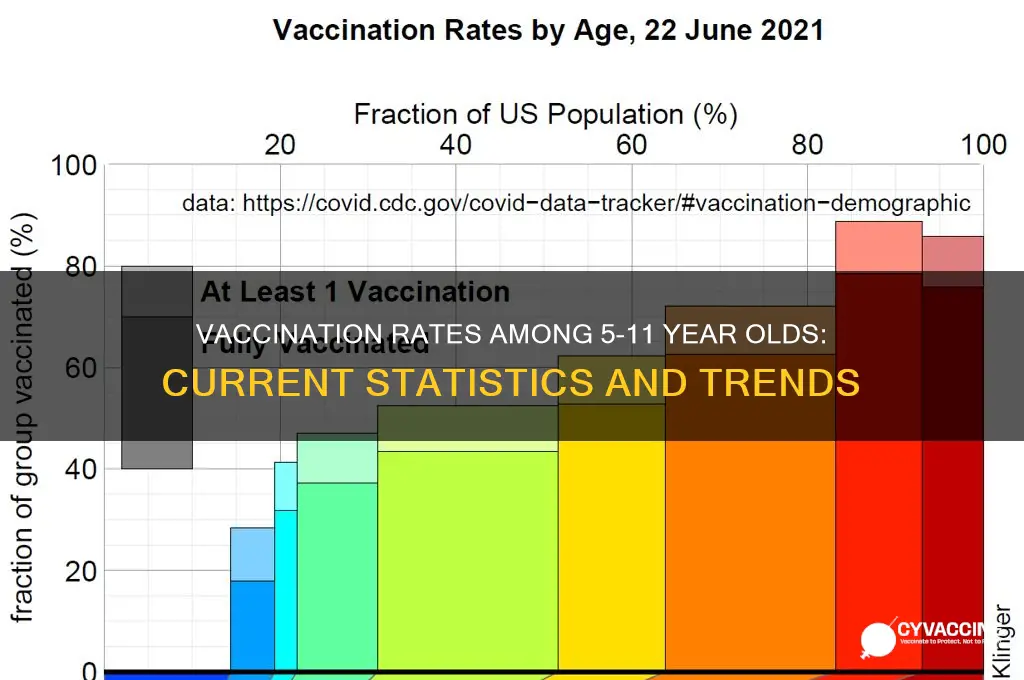
Vaccination Rates by Country: Global 5-11 age group COVID-19 vaccination coverage statistics
As of recent data, the global vaccination rates for children aged 5 to 11 against COVID-19 vary significantly by country, reflecting disparities in healthcare infrastructure, policy decisions, and public trust. For instance, countries like Canada and the United States report vaccination rates around 50-60% for this age group, with many children receiving both doses of the Pfizer-BioNTech vaccine, administered at a lower dosage (10 micrograms per shot) compared to adults. In contrast, many low-income countries in Africa and parts of Asia struggle to reach even 10% coverage due to limited vaccine supply and logistical challenges.
Analyzing these trends reveals a clear correlation between economic status and vaccination accessibility. High-income nations often prioritize pediatric vaccination campaigns, leveraging robust healthcare systems and public awareness initiatives. For example, Singapore and Israel have achieved over 70% vaccination rates in the 5-11 age group by integrating school-based vaccination drives and offering incentives like educational materials or small rewards. Conversely, in countries like Nigeria or Haiti, where vaccine hesitancy and distribution hurdles persist, coverage remains below 5%, highlighting the need for targeted global support.
From a practical standpoint, parents in countries with lower vaccination rates can take proactive steps to protect their children. First, stay informed about local vaccination drives and eligibility criteria, often available through health ministry websites or community health centers. Second, address concerns about vaccine safety by consulting trusted healthcare providers or referring to WHO-approved resources. Finally, advocate for equitable vaccine distribution by supporting global initiatives like COVAX, which aims to provide doses to underserved regions.
Comparatively, the success of pediatric vaccination programs in some countries offers lessons for others. For instance, Spain’s 80% coverage rate among 5-11-year-olds can be attributed to clear communication campaigns, parental consent simplification, and collaboration with schools. In contrast, Japan’s slower rollout, initially hindered by regulatory delays, improved after prioritizing transparency and addressing public concerns. These examples underscore the importance of tailored strategies that consider cultural, logistical, and informational factors.
Ultimately, the global 5-11 vaccination landscape is a mosaic of progress and challenges. While some countries have made strides in protecting their youngest populations, others face systemic barriers that require international cooperation. By learning from successful models, addressing hesitancy, and ensuring equitable access, the world can move closer to safeguarding all children against COVID-19. Practical steps, from local advocacy to global solidarity, are essential to bridge the gap and create a healthier future for this vulnerable age group.
Vaccine Reactions: Understanding Public Responses and Concerns Worldwide
You may want to see also
Explore related products





![]()
Vaccine Types Used: Approved vaccines for children aged 5-11 worldwide
As of late 2023, the Pfizer-BioNTech COVID-19 vaccine remains the most widely approved and administered vaccine for children aged 5-11 globally. This vaccine, known as Comirnaty, is administered in a two-dose regimen, with each dose containing 10 micrograms of mRNA—one-third of the dosage used for individuals aged 12 and older. The doses are typically given 3 to 8 weeks apart, depending on local health guidelines. Its approval in this age group was based on clinical trials demonstrating a robust immune response and a favorable safety profile, with common side effects including mild fatigue, headache, and injection site pain.
In contrast, the Moderna COVID-19 vaccine, though widely used in adults, has seen limited approval for children aged 5-11 in select countries such as Canada and the European Union. Moderna’s Spikevax is administered in a 50-microgram dose for this age group, half the adult dosage. However, its rollout has been slower compared to Pfizer-BioNTech, partly due to later regulatory approvals and concerns about rare side effects like myocarditis, particularly in adolescent males. Parents and caregivers should consult local health authorities for the most up-to-date recommendations on vaccine availability and suitability.
Beyond mRNA vaccines, inactivated virus vaccines like Sinovac’s CoronaVac and Sinopharm’s BBIBP-CorV have been approved for children aged 5-11 in several countries, including China, Brazil, and parts of the Middle East. These vaccines use a traditional technology platform, delivering inactivated SARS-CoV-2 virus particles to stimulate an immune response. Typically administered in two doses, 3 to 4 weeks apart, they offer a familiar alternative for regions with established trust in inactivated vaccines. However, their efficacy data in this age group is less comprehensive compared to mRNA vaccines, and booster recommendations vary widely.
For parents navigating these options, practical considerations include vaccine availability, local health guidelines, and individual child health factors. For instance, children with a history of severe allergic reactions may require additional monitoring post-vaccination. Additionally, combining vaccination appointments with routine check-ups can reduce stress for both children and caregivers. While the choice of vaccine may seem overwhelming, the overarching goal remains consistent: protecting children from severe COVID-19 outcomes while minimizing disruptions to their education and social development.
Human Cells in Vaccines: Fact-Checking a Common Misconception
You may want to see also
Explore related products






![]()
Side Effects Data: Common side effects reported in vaccinated 5-11-year-olds
The COVID-19 vaccination rollout for children aged 5 to 11 has been a significant step in the global effort to control the pandemic. As of recent data, millions of children in this age group have received at least one dose of the vaccine, with the Pfizer-BioNTech vaccine being the primary option authorized for this demographic. This widespread administration has allowed for the collection of valuable data on side effects, providing insights into what parents and caregivers can expect.
Analyzing the side effects reported in vaccinated 5- to 11-year-olds reveals a pattern consistent with those observed in older age groups, though generally milder. The most common side effects include pain at the injection site, fatigue, headache, and fever. These symptoms typically appear within 24 to 48 hours after vaccination and resolve within a few days. For instance, approximately 60-70% of children report mild to moderate arm pain, while fever is less frequent, affecting around 10-15% of recipients. It’s important to note that these reactions are a normal part of the body’s immune response and indicate the vaccine is working as intended.
From a practical standpoint, parents can take proactive steps to manage these side effects. Over-the-counter pain relievers like acetaminophen or ibuprofen can be used to alleviate discomfort, but only if the child is otherwise healthy and there are no contraindications. Encouraging hydration and rest is also beneficial. Applying a cool, damp cloth to the injection site can reduce soreness. However, aspirin should be avoided in children due to the risk of Reye’s syndrome. Monitoring the child for any unusual or severe symptoms, such as persistent high fever or difficulty breathing, is crucial, though such cases are extremely rare.
Comparatively, the side effects in 5- to 11-year-olds are less pronounced than in adolescents and adults, likely due to the lower dosage administered. Children in this age group receive a 10-microgram dose per shot, one-third of the 30-microgram dose given to individuals aged 12 and older. This reduced dosage strikes a balance between efficacy and minimizing adverse reactions, as evidenced by clinical trial data showing robust immune responses with fewer systemic side effects. The tailored approach underscores the importance of age-specific vaccine formulations in pediatric populations.
In conclusion, understanding the side effects data for vaccinated 5- to 11-year-olds empowers parents and caregivers to make informed decisions and prepare for the vaccination process. While the reported side effects are generally mild and short-lived, knowing how to manage them can enhance the overall experience. The data reinforces the safety and tolerability of the vaccine in this age group, contributing to broader public health goals. As vaccination rates continue to rise, ongoing monitoring and transparent communication will remain essential in maintaining trust and ensuring widespread acceptance.
NHS App: Your Digital Proof of COVID-19 Vaccination Explained
You may want to see also
Explore related products






![]()
Efficacy Studies: Research on vaccine effectiveness in the 5-11 age group
Vaccine efficacy in the 5-11 age group has been a critical focus of recent research, particularly as pediatric COVID-19 cases surged during the pandemic. Studies have consistently shown that the Pfizer-BioNTech vaccine, administered as a lower 10-microgram dose compared to the 30-microgram dose for older age groups, elicits a robust immune response in this demographic. Clinical trials involving thousands of children demonstrated that the vaccine was 90.7% effective in preventing symptomatic COVID-19, with no serious safety concerns reported. These findings were pivotal in the FDA’s emergency use authorization for this age group in October 2021, providing parents and healthcare providers with a scientifically validated tool to protect children.
Analyzing the data further, researchers observed that the immune response in 5-11-year-olds was comparable to that seen in 16-25-year-olds, despite the lower dosage. This suggests that the pediatric formulation strikes a balance between efficacy and safety, minimizing potential side effects while ensuring adequate protection. However, real-world studies have highlighted variability in uptake, with vaccination rates among 5-11-year-olds lagging behind other age groups. This gap underscores the need for targeted public health messaging to address parental hesitancy and misinformation, ensuring that evidence-based research translates into actionable protection for children.
Practical considerations for parents include understanding the vaccination schedule: two doses administered three weeks apart, with peak immunity achieved about a week after the second dose. Common side effects, such as fatigue, headache, or soreness at the injection site, are typically mild and short-lived. For children with underlying health conditions, consultation with a pediatrician is advised, as studies have shown the vaccine to be safe and effective even in immunocompromised populations. Parents should also stay informed about booster recommendations, as evolving research may suggest additional doses to maintain protection against new variants.
Comparatively, the 5-11 age group’s vaccine efficacy studies stand out for their emphasis on safety and age-appropriate dosing. Unlike adult trials, pediatric research required meticulous attention to ethical considerations, including parental consent and child-friendly trial designs. This rigor has built trust in the scientific community, but challenges remain in translating research into widespread vaccination. For instance, while the vaccine reduces the risk of severe illness and hospitalization, its impact on asymptomatic transmission in children is still being studied, complicating public health messaging.
In conclusion, efficacy studies on the 5-11 age group have provided a clear scientific foundation for vaccination, but their success hinges on bridging the gap between research and practice. Parents and caregivers play a pivotal role in this process, armed with accurate information and practical guidance. As new data emerges, ongoing dialogue between healthcare providers and families will be essential to ensure that the benefits of vaccination are fully realized for this vulnerable population.
Massachusetts Vaccine Records: Accessing Your State Immunization History
You may want to see also
Explore related products






![]()
Parental Hesitancy: Factors influencing parents' decisions to vaccinate children aged 5-11
As of recent data, vaccination rates for children aged 5 to 11 vary significantly across regions, with some areas reporting rates as low as 20% and others nearing 60%. This disparity highlights a critical issue: parental hesitancy. Understanding the factors driving this reluctance is essential for addressing concerns and improving uptake. One primary factor is the perceived risk versus benefit of the vaccine. Many parents weigh the relatively low severity of COVID-19 in children against potential side effects, even though clinical trials have shown the vaccine to be safe and effective for this age group, with common side effects limited to mild symptoms like soreness at the injection site or fatigue.
Another influential factor is misinformation, which spreads rapidly through social media and other channels. False claims about fertility, long-term effects, or the vaccine’s necessity for children have sown doubt among parents. For instance, a common myth suggests the vaccine contains harmful substances, despite regulatory bodies confirming its safety and transparency in ingredient lists. Combating misinformation requires clear, accessible communication from trusted sources, such as pediatricians or public health campaigns, that directly address parental concerns with evidence-based facts.
Cultural and socioeconomic barriers also play a role in parental hesitancy. In some communities, historical mistrust of medical institutions or limited access to healthcare information creates skepticism. Additionally, logistical challenges, such as transportation to vaccination sites or difficulty taking time off work, can deter parents from pursuing vaccination for their children. Tailored interventions, like mobile clinics or multilingual educational materials, can help bridge these gaps and make vaccination more accessible and culturally relevant.
Finally, the influence of peer networks cannot be overlooked. Parents often look to friends, family, or online communities for guidance, and if these groups express skepticism, it can reinforce hesitancy. Encouraging open dialogue and sharing personal experiences of vaccination can help normalize the decision. For example, testimonials from parents who have vaccinated their children, coupled with data on the vaccine’s impact in reducing school outbreaks, can provide compelling social proof. Addressing parental hesitancy requires a multifaceted approach that respects concerns while providing accurate, actionable information to empower informed decision-making.
Tetanus Vaccination: Weighing Risks Against the Dangers of Non-Vaccination
You may want to see also
Frequently asked questions
As of the latest data, approximately 40% of children aged 5 to 11 in the U.S. have received at least one dose of the COVID-19 vaccine.
Global vaccination rates for 5 to 11-year-olds vary widely, with some countries reporting rates below 10%, while others, like Canada and parts of Europe, have rates closer to 50%.
Clinical trials and real-world data show that COVID-19 vaccines are safe and effective for children aged 5 to 11, with mild side effects like soreness, fatigue, or fever being the most common.
Vaccines for this age group are highly effective at preventing severe illness, hospitalization, and death from COVID-19, with efficacy rates around 90% for preventing symptomatic infection.
Vaccinating children in this age group helps protect them from severe COVID-19, reduces the spread of the virus, and contributes to community immunity, safeguarding vulnerable populations.