The polio vaccine, a cornerstone in the global eradication of poliomyelitis, is administered through two primary methods: the inactivated poliovirus vaccine (IPV) and the oral poliovirus vaccine (OPV). IPV, given as an injection, is typically used in countries with low polio risk, offering robust individual protection by preventing paralytic disease. OPV, delivered orally in drops or on a sugar cube, is favored in regions with active polio transmission due to its ease of administration and ability to induce mucosal immunity, which helps interrupt viral transmission in communities. Both vaccines are often included in routine childhood immunization schedules, with multiple doses recommended to ensure long-term immunity. The choice of vaccine and dosing regimen depends on local disease prevalence, public health goals, and global eradication strategies.
Explore related products






What You'll Learn
![]()
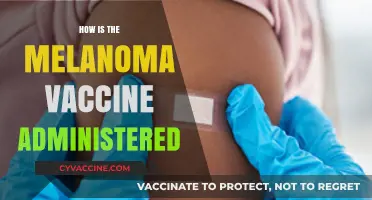
Oral drops administration
The oral polio vaccine (OPV) is a cornerstone of global polio eradication efforts, and its administration via drops is a simple yet powerful method. Typically, the vaccine is given as two drops directly into a child's mouth, a process that takes mere seconds but offers lifelong protection. This method is particularly effective because it stimulates immunity in the gut, where the poliovirus first enters the body, providing robust defense against infection.
Administering OPV drops requires minimal training, making it ideal for mass vaccination campaigns in remote or resource-limited areas. Health workers or volunteers use a dropper to measure the precise dose, ensuring consistency across millions of recipients. The vaccine is stable at room temperature for a limited time, allowing for easier transport and distribution without the need for constant refrigeration. This logistical advantage has been critical in reaching underserved populations and maintaining high vaccination coverage rates.
For parents and caregivers, the process is straightforward but requires attention to detail. Children under five years old are the primary recipients, with the World Health Organization recommending a minimum of three doses to ensure full immunity. In some high-risk areas, additional rounds are conducted to strengthen protection. It’s essential to avoid feeding or giving water to the child immediately before or after administration, as this could dilute the vaccine and reduce its effectiveness.
One of the most compelling aspects of OPV drops is their ability to induce passive immunity in communities. When vaccinated individuals shed the weakened virus, it can immunize others through exposure, creating a ripple effect of protection. This phenomenon has been instrumental in interrupting poliovirus transmission in densely populated regions. However, this same feature necessitates careful monitoring to ensure the vaccine strain doesn’t revert to a harmful form, a rare but documented occurrence.
Despite its success, the oral drops method is gradually being complemented by the inactivated polio vaccine (IPV) in some regions to address specific risks associated with OPV. Yet, in the fight against polio, the simplicity, scalability, and effectiveness of oral drops remain unparalleled. For now, this method continues to play a pivotal role in the global push toward a polio-free world.
Fauci's Wife and the Vaccine Approval: Unraveling the Truth
You may want to see also
Explore related products






![]()
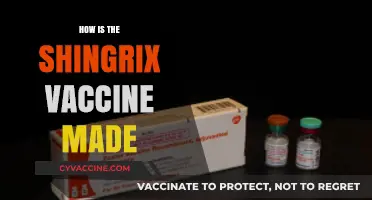
Injectable vaccine methods
Injectable polio vaccines (IPV) are administered via intramuscular or subcutaneous injection, offering a safe and effective method to prevent poliomyelitis. Unlike oral polio vaccines (OPV), which use a live attenuated virus, IPV contains inactivated poliovirus, eliminating the risk of vaccine-derived poliovirus cases. This method is particularly crucial in regions transitioning from OPV to IPV as part of the global polio eradication strategy. The standard dosage for IPV is 0.5 mL, typically injected into the vastus lateralis muscle of the thigh for infants and young children, or the deltoid muscle of the upper arm for older children and adults. Proper needle selection—22–25 gauge for adults and 25–27 gauge for children—ensures minimal discomfort and effective delivery.
The administration process requires precision to maximize efficacy and minimize adverse effects. Healthcare providers must follow aseptic techniques, including cleaning the injection site with an alcohol swab and allowing it to dry before needle insertion. For intramuscular injections, the needle should be inserted at a 90-degree angle to ensure the vaccine reaches the muscle tissue. Subcutaneous administration, less common but occasionally used, involves a 45-degree angle to deposit the vaccine into the fatty tissue just beneath the skin. Post-injection, the site should be monitored for any immediate reactions, though severe side effects are rare with IPV.
One of the key advantages of injectable methods is their suitability for individuals with immunodeficiencies or those living in areas where OPV’s live virus could pose a risk. IPV is often part of combination vaccines, such as DTaP-IPV-Hib, streamlining immunization schedules for children. However, its higher cost and logistical challenges, including the need for trained personnel and sterile equipment, can limit accessibility in low-resource settings. Despite this, IPV remains a cornerstone of polio prevention, particularly in the endgame of eradication efforts.
Comparatively, injectable methods offer a more controlled and standardized approach than oral vaccines, which rely on the recipient’s gastrointestinal tract for absorption. This reliability is critical for achieving herd immunity, especially in populations with varying health statuses. For instance, IPV is recommended for pregnant women and immunocompromised individuals, groups for whom OPV is contraindicated. Its inactivated nature also eliminates the risk of vaccine-associated paralytic polio (VAPP), a rare but serious complication of OPV.
In practice, successful IPV administration hinges on adherence to guidelines and patient education. Parents and caregivers should be informed about potential mild side effects, such as soreness at the injection site or low-grade fever, which typically resolve within 24–48 hours. Ensuring proper storage of the vaccine—between 2°C and 8°C—is equally vital to maintain its potency. As the world edges closer to polio eradication, injectable vaccine methods like IPV play an indispensable role in safeguarding global health, combining safety, efficacy, and strategic utility.
Antibiotics vs. Vaccines: Understanding Their Unique Roles in Medicine
You may want to see also
Explore related products






![]()
Dose scheduling guidelines
The polio vaccine's effectiveness hinges on precise dose scheduling, a critical factor in ensuring robust immunity. For the inactivated poliovirus vaccine (IPV), the Centers for Disease Control and Prevention (CDC) recommends a four-dose series for children: the first dose at 2 months, followed by doses at 4 months, 6-18 months, and a booster at 4-6 years. This staggered approach allows the immune system to build and maintain protective antibodies against all three poliovirus types. Adhering to this schedule is particularly vital in regions with ongoing polio transmission or low vaccination coverage, where the risk of exposure remains significant.
In contrast, the oral poliovirus vaccine (OPV), used primarily in global eradication efforts, typically follows a different regimen. The World Health Organization (WHO) advises a series of multiple doses, often starting at birth in high-risk areas, with subsequent doses administered at 6, 10, and 14 weeks. This frequent dosing is designed to rapidly establish gut immunity, which is crucial for interrupting poliovirus transmission in communities. However, the live attenuated nature of OPV necessitates careful consideration of its use in immunocompromised individuals, where IPV is the safer alternative.
For adults, dose scheduling varies based on vaccination history and risk factors. Those who received the full childhood series generally do not need additional doses unless traveling to polio-endemic areas. In such cases, a single lifetime IPV booster is recommended. Unvaccinated adults require a three-dose series, with the first two doses administered 4-8 weeks apart and the third dose 6-12 months after the second. This accelerated schedule ensures rapid protection, though it may not achieve the same long-term immunity as the pediatric series.
Practical considerations also play a role in dose scheduling. Missed doses should be administered as soon as possible, without restarting the series. However, doses given too close together may reduce efficacy, particularly with IPV. For instance, if the interval between doses is less than 4 weeks, the dose should be repeated. Additionally, co-administration with other vaccines is generally safe and encouraged to improve compliance, though certain combinations (e.g., OPV with antibiotics) may require careful timing to avoid interference.
In summary, dose scheduling guidelines for the polio vaccine are tailored to age, risk, and vaccine type, balancing the need for rapid protection with long-term immunity. Strict adherence to these schedules is essential for individual and community-level protection, particularly in the final push toward global polio eradication. Healthcare providers must remain vigilant in educating caregivers and patients about the importance of completing the full series, as even a single missed dose can leave individuals vulnerable to this debilitating disease.
Is BCG Vaccination Mandatory for Babies? Understanding the Necessity
You may want to see also
Explore related products






![]()
Cold chain storage needs
The polio vaccine's journey from manufacturer to recipient is a delicate dance, heavily reliant on cold chain storage. This intricate system ensures the vaccine remains potent and effective, safeguarding its ability to prevent a debilitating disease. Temperatures must be meticulously maintained between 2°C and 8°C (36°F and 46°F) throughout transportation and storage. Even brief exposure to temperatures outside this range can render the vaccine ineffective, wasting precious doses and potentially leaving individuals vulnerable.
Imagine a fragile, temperature-sensitive elixir – that's essentially what the polio vaccine is.
Maintaining this narrow temperature window presents a logistical challenge, particularly in regions with limited infrastructure or extreme climates. Refrigerated trucks, cold boxes, and vaccine carriers become vital tools in this endeavor. For instance, in remote areas, solar-powered refrigerators can provide a sustainable solution, ensuring the cold chain remains unbroken even without reliable electricity. Diligent monitoring is crucial; data loggers continuously track temperatures, alerting health workers to any deviations that could compromise vaccine integrity.
Every link in the cold chain, from production facilities to local clinics, must be meticulously managed to guarantee the vaccine's efficacy.
The consequences of a broken cold chain are dire. Ineffective vaccines not only fail to protect individuals but can also contribute to the resurgence of polio in communities. This underscores the critical importance of investing in robust cold chain infrastructure, particularly in areas where polio remains a threat. It's not just about storing a vaccine; it's about safeguarding the health of entire populations.
Optimal Arm Vaccination Site: Where to Get Your Shot for Comfort and Effectiveness
You may want to see also
Explore related products



$27.99



![]()
Trained healthcare provider roles
Trained healthcare providers are the linchpin in the effective and safe administration of the polio vaccine. Their roles extend far beyond simply injecting the vaccine; they are responsible for ensuring proper dosage, identifying eligible recipients, and maintaining the cold chain to preserve vaccine efficacy. For instance, the oral polio vaccine (OPV) is typically administered in drops, with a standard dose of 0.05 mL for infants and children under 5 years old. Healthcare providers must carefully measure this dose using a calibrated dropper to avoid under or over-administration, which could compromise immunity or cause adverse effects.
In contrast, the inactivated polio vaccine (IPV), often used in combination vaccines like DTaP-IPV-Hib, requires a 0.5 mL intramuscular injection for children. Here, the provider’s precision in selecting the correct injection site (e.g., the vastus lateralis muscle in infants) and technique (e.g., needle angle and depth) is critical. Providers must also adhere to age-specific schedules, such as administering IPV at 2, 4, and 6 months, followed by a booster between 4–6 years, to ensure optimal immune response. This meticulous attention to detail underscores the provider’s role as both technician and guardian of public health.
Beyond technical skills, healthcare providers serve as educators, addressing parental concerns and dispelling myths about vaccine safety. For example, they explain that OPV’s live attenuated virus is safe for most children but should be avoided in immunocompromised individuals. Providers also monitor for rare adverse reactions, such as allergic responses or, in the case of OPV, vaccine-derived poliovirus (VDPV), which occurs in extremely rare cases. This dual role of clinician and communicator is vital in building trust and ensuring high vaccination rates.
In resource-limited settings, providers often lead community outreach efforts, traveling to remote areas to administer vaccines during campaigns. They must be adept at managing logistics, such as transporting vaccines in portable cold boxes and using temperature monitors to maintain the 2–8°C range required for IPV. Practical tips, like pre-marking injection sites on a child’s thigh to speed up the process during mass campaigns, highlight the provider’s ability to adapt to challenging environments while maintaining precision and safety.
Ultimately, the trained healthcare provider’s role in polio vaccine dispensation is multifaceted, blending technical expertise, educational outreach, and logistical ingenuity. Their work not only ensures individual protection but also contributes to the global goal of polio eradication. By mastering dosage, technique, and communication, these providers bridge the gap between vaccine development and community immunity, making them indispensable in the fight against this debilitating disease.
Understanding Antigens: Key Role in Vaccine Function and Immunity
You may want to see also
Frequently asked questions
The polio vaccine is typically dispensed orally (OPV) as drops or administered via injection (IPV). OPV is given by placing drops in the mouth, while IPV is injected into the muscle or under the skin, depending on the formulation.
The oral polio vaccine (OPV) can often be administered at home or in community settings during vaccination campaigns. However, the inactivated polio vaccine (IPV) is usually given in healthcare facilities by trained professionals due to its injectable nature.
The number of doses varies by country and vaccine type. Typically, OPV requires 3–4 doses, while IPV requires 2–3 doses. Doses are spaced 4–8 weeks apart for OPV and 4–8 weeks or 6–12 months apart for IPV, depending on the schedule. A booster dose may also be recommended.