Monoclonal antibodies and vaccines are both powerful tools in the fight against infectious diseases, but they function in distinct ways. Vaccines work by stimulating the body’s immune system to produce its own antibodies and memory cells, providing long-term protection against a specific pathogen. In contrast, monoclonal antibodies are lab-created proteins designed to mimic the immune system’s ability to fight off harmful pathogens. They are administered directly into the body and offer immediate, short-term protection or treatment by targeting specific antigens on the pathogen. While vaccines are preventive measures that require time to build immunity, monoclonal antibodies are therapeutic agents used to treat active infections or provide temporary immunity in high-risk individuals. This fundamental difference in mechanism and application highlights their complementary roles in disease management.
| Characteristics | Values |
|---|---|
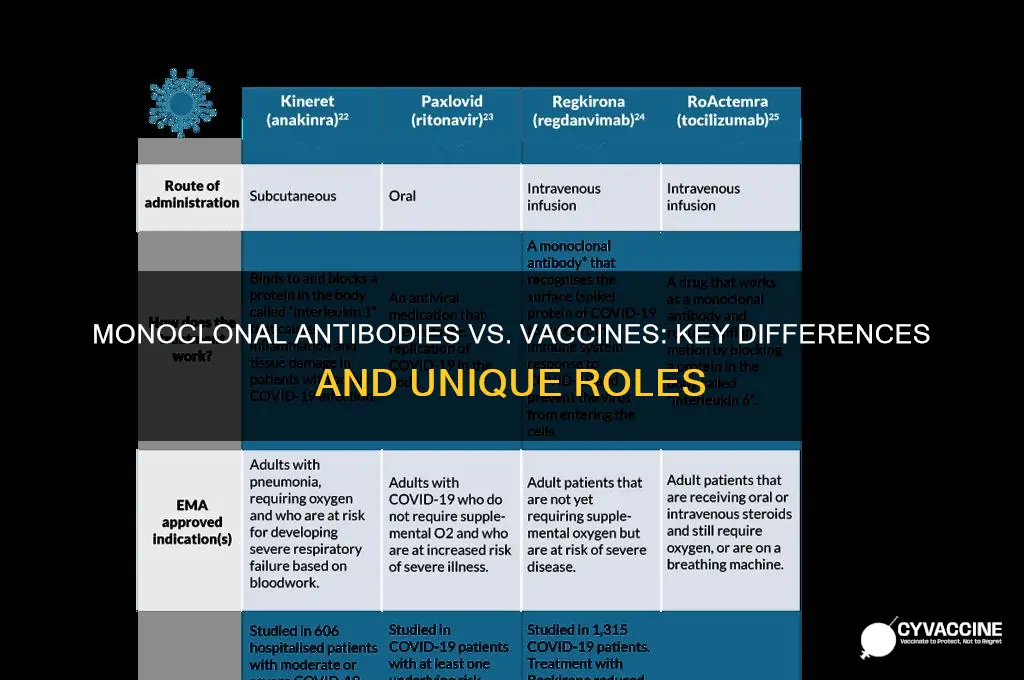
| Mechanism of Action | Monoclonal antibodies (mAbs) are lab-made proteins that mimic the immune system’s ability to fight off harmful pathogens by directly targeting and neutralizing the virus or toxin. Vaccines stimulate the immune system to produce its own antibodies and memory cells to prevent future infections. |
| Purpose | mAbs are primarily used for treatment or prevention in high-risk individuals (e.g., immunocompromised patients) after exposure or infection. Vaccines are used for prevention by building immunity before exposure. |
| Administration | mAbs are typically administered via intravenous infusion or injection and provide immediate but temporary protection. Vaccines are usually given intramuscularly and require time (days to weeks) to build immunity. |
| Duration of Protection | mAbs offer short-term protection, lasting weeks to months. Vaccines provide longer-term immunity, often lasting months to years, and can be boosted with additional doses. |
| Immune Response | mAbs bypass the immune system and directly provide antibodies. Vaccines train the immune system to recognize and respond to the pathogen, creating a memory response for future protection. |
| Target Population | mAbs are often reserved for specific high-risk groups or those with severe disease. Vaccines are recommended for the general population to achieve herd immunity. |
| Development Time | mAbs can be developed and deployed relatively quickly in response to emerging pathogens. Vaccines typically require longer development and testing periods to ensure safety and efficacy. |
| Cost | mAbs are generally more expensive to produce and administer compared to vaccines. Vaccines are more cost-effective for widespread use. |
| Storage and Distribution | mAbs often require cold chain storage and specialized administration facilities. Vaccines vary in storage requirements, with some needing refrigeration and others stable at room temperature. |
| Side Effects | mAbs may cause infusion-related reactions or allergic responses. Vaccines can cause mild side effects like soreness, fever, or fatigue, but severe reactions are rare. |
| Approval and Availability | mAbs are often authorized under emergency use during outbreaks. Vaccines undergo rigorous clinical trials and are fully approved for widespread use. |
| Examples | mAbs: Casirivimab/Imdevimab (REGEN-COV), Sotrovimab. Vaccines: Pfizer-BioNTech, Moderna, AstraZeneca, Johnson & Johnson. |
Explore related products


$22.99 $22.99




What You'll Learn
- Mechanism of Action: Vaccines trigger immune response; monoclonal antibodies provide direct, immediate immune system boost
- Duration of Protection: Vaccines offer long-term immunity; monoclonal antibodies provide short-term protection, weeks to months
- Administration Method: Vaccines are preventive, injected; monoclonal antibodies are therapeutic, often intravenous
- Target Population: Vaccines for healthy individuals; monoclonal antibodies for high-risk or infected patients
- Immune Response: Vaccines rely on body’s response; monoclonal antibodies are lab-made, ready-to-use proteins
![]()
Mechanism of Action: Vaccines trigger immune response; monoclonal antibodies provide direct, immediate immune system boost
Vaccines and monoclonal antibodies (mAbs) are both powerful tools in the fight against infectious diseases, but they operate through distinct mechanisms of action. Vaccines function by triggering an active immune response in the body. When a vaccine is administered, it introduces a harmless form of a pathogen (such as a weakened virus, a fragment of the virus, or its genetic material) to the immune system. This prompts the body to recognize the pathogen as a threat and mount a defense by producing antibodies and activating immune cells like T cells. The immune system also creates memory cells, which "remember" the pathogen and enable a faster, more robust response if the individual is exposed to the real pathogen in the future. This process takes time—typically days to weeks—as the body builds its own immune defenses.
In contrast, monoclonal antibodies provide a direct and immediate immune system boost. Instead of relying on the body to produce its own antibodies, mAbs are lab-created proteins designed to mimic the body’s natural antibodies. These antibodies are specifically engineered to target a particular antigen (e.g., the spike protein of a virus). When administered, mAbs immediately bind to the pathogen, neutralizing it or marking it for destruction by other immune cells. This mechanism bypasses the need for the immune system to generate its own response, offering rapid protection. However, this protection is temporary, as mAbs do not confer long-term immunity or create immune memory.
The key difference in their mechanisms lies in proactivity versus reactivity. Vaccines are proactive, training the immune system to recognize and combat a pathogen before exposure, thereby providing long-lasting immunity. Monoclonal antibodies, on the other hand, are reactive, offering immediate but short-term protection by directly neutralizing the pathogen. Vaccines stimulate the body’s own immune machinery, while mAbs act as external agents that supplement or replace the immune response.
Another critical distinction is their application and timing. Vaccines are typically used as a preventive measure, administered before infection to prepare the body for future encounters with the pathogen. Monoclonal antibodies are often used as a treatment or post-exposure prophylaxis, providing rapid protection to individuals who are already infected or at high risk of infection. For example, COVID-19 vaccines prevent infection by building immunity, whereas COVID-19 monoclonal antibodies are used to treat severe cases or prevent progression in vulnerable individuals.
In summary, vaccines and monoclonal antibodies differ fundamentally in their mechanism of action. Vaccines trigger an active, long-lasting immune response by training the body to recognize and combat pathogens, while monoclonal antibodies provide a direct, immediate immune boost by neutralizing the pathogen themselves. Both approaches are valuable in different contexts, with vaccines serving as a preventive tool and mAbs offering rapid therapeutic intervention. Understanding these mechanisms highlights the complementary roles of vaccines and monoclonal antibodies in modern medicine.
Vaccine Passports: US Plans and Privacy Concerns
You may want to see also
Explore related products






![]()
Duration of Protection: Vaccines offer long-term immunity; monoclonal antibodies provide short-term protection, weeks to months
The duration of protection is a critical distinction between vaccines and monoclonal antibody treatments. Vaccines are designed to stimulate the body's immune system to produce its own antibodies and immune memory cells, which can provide long-term immunity against a specific pathogen. This process, known as active immunization, typically takes a few weeks to develop after vaccination but can offer protection lasting years or even a lifetime, depending on the vaccine. For example, vaccines like those for measles, mumps, and rubella (MMR) often confer lifelong immunity after a complete series of doses. Booster shots may be required for some vaccines to maintain high levels of protection, but the foundational immunity remains robust.
In contrast, monoclonal antibodies provide passive immunity, meaning they directly deliver lab-made antibodies to the body to neutralize the pathogen. This approach offers immediate protection but is short-lived, typically lasting from several weeks to a few months. Monoclonal antibodies do not induce immune memory, so once they are metabolized by the body, their protective effects diminish. For instance, monoclonal antibody treatments for COVID-19, such as those developed by Regeneron or Eli Lilly, have been shown to reduce the risk of severe disease in high-risk individuals, but their protection wanes after a few months. This short-term nature makes them more suitable for prophylaxis or early treatment rather than long-term prevention.
The difference in duration of protection is rooted in how these interventions interact with the immune system. Vaccines train the immune system to recognize and combat the pathogen independently, creating a lasting defense mechanism. Monoclonal antibodies, however, act as a temporary shield, providing immediate but transient protection without engaging the body’s own immune response in a way that builds long-term immunity. This makes vaccines the preferred choice for widespread, durable prevention of infectious diseases, while monoclonal antibodies are often reserved for specific scenarios, such as treating vulnerable populations or preventing severe illness in those already exposed to the pathogen.
Another factor to consider is the logistical and practical implications of these differences. Vaccines, with their long-term protection, are administered in campaigns aimed at achieving herd immunity and reducing the overall spread of a disease. Monoclonal antibodies, due to their short-term efficacy, are typically used in targeted interventions, such as for individuals who cannot mount an adequate immune response to vaccines or those at high risk of severe disease. The recurring need for monoclonal antibody treatments also poses challenges in terms of cost, accessibility, and healthcare resource allocation, further highlighting the advantages of vaccines for broad, sustained public health benefits.
In summary, the duration of protection is a fundamental difference between vaccines and monoclonal antibodies. Vaccines offer long-term immunity by training the immune system to respond effectively to future threats, while monoclonal antibodies provide immediate but short-term protection by directly supplying antibodies. This distinction influences their use in clinical and public health settings, with vaccines being the cornerstone of disease prevention and monoclonal antibodies serving as a valuable but temporary tool for specific populations or situations. Understanding these differences is essential for making informed decisions about their application in combating infectious diseases.
Understanding Vaccine Efficacy: Calculation Methods and Real-World Implications
You may want to see also
Explore related products






![]()
Administration Method: Vaccines are preventive, injected; monoclonal antibodies are therapeutic, often intravenous
The administration method is a key differentiator between vaccines and monoclonal antibodies, highlighting their distinct roles in disease management. Vaccines are primarily preventive tools designed to prepare the immune system for future encounters with pathogens. They are typically administered via injection, most commonly intramuscularly or subcutaneously. This delivery method allows the vaccine to introduce a harmless piece of the pathogen, such as a protein or a weakened virus, to the immune system. The immune system then recognizes this foreign entity, produces antibodies, and creates memory cells. This process ensures that if the actual pathogen invades the body in the future, the immune system can respond swiftly and effectively, preventing or reducing the severity of the disease. Vaccination campaigns have been instrumental in eradicating or controlling numerous infectious diseases, such as smallpox and polio, by providing long-term immunity to populations.
In contrast, monoclonal antibodies serve a therapeutic purpose, meaning they are used to treat active infections or diseases rather than prevent them. These antibodies are laboratory-produced molecules engineered to serve as substitute antibodies that can restore, enhance, or mimic the immune system's attack on harmful pathogens. Unlike vaccines, monoclonal antibodies are often administered intravenously, allowing them to enter the bloodstream directly and start working immediately. This method of delivery is crucial for patients who are already infected and need rapid relief from symptoms or reduction in disease severity. For example, monoclonal antibodies have been used to treat conditions like COVID-19, where they can neutralize the virus and prevent it from causing severe illness, especially in high-risk individuals.
The intravenous administration of monoclonal antibodies ensures a high concentration of the therapeutic agent reaches the target sites quickly, which is essential for their effectiveness. This is particularly important in cases where the immune system is compromised or the disease progresses rapidly. However, this approach also means that the protection offered by monoclonal antibodies is immediate but temporary, lasting only as long as the antibodies remain in the system, typically a few weeks to a few months. This is in stark contrast to vaccines, which aim to provide long-lasting immunity through the development of memory cells.
Another aspect of administration is the frequency and setting. Vaccines are usually given in a series of doses over a period, often in outpatient settings like clinics or pharmacies. This allows for the gradual build-up of immunity and the establishment of long-term protection. Monoclonal antibodies, on the other hand, are typically administered in a single dose or a short course, often in a clinical setting where patients can be monitored for any immediate reactions. This is because their use is targeted at individuals who are already ill and require immediate intervention.
The differences in administration methods also reflect the distinct goals of vaccines and monoclonal antibodies. Vaccines aim to educate the immune system to recognize and combat future threats, a process that requires time and the body's active participation. Monoclonal antibodies, however, provide a direct and immediate solution by supplying ready-made antibodies to fight off an existing infection. This therapeutic approach is particularly valuable for vulnerable populations, such as the elderly or immunocompromised individuals, who may not mount an adequate response to a vaccine or are at high risk of severe disease.
In summary, the administration methods of vaccines and monoclonal antibodies are tailored to their respective purposes. Vaccines, being preventive, are injected to stimulate a long-term immune response, while monoclonal antibodies, being therapeutic, are often administered intravenously to provide immediate and targeted treatment. Understanding these differences is crucial for healthcare providers and patients alike, as it informs the appropriate use of these tools in disease prevention and management.
Vaccine Side Effects: Muscle Spasms Explained
You may want to see also
Explore related products


$92.93 $98.95



![]()
Target Population: Vaccines for healthy individuals; monoclonal antibodies for high-risk or infected patients
Monoclonal antibodies and vaccines serve distinct purposes and are targeted at different populations based on their mechanisms of action and intended outcomes. Vaccines are primarily designed for healthy individuals as a preventive measure, aiming to stimulate the immune system to recognize and combat pathogens before exposure. They work by introducing a harmless component of the virus or a weakened/inactivated form of it, prompting the body to produce antibodies and memory cells. This proactive approach ensures that if the individual encounters the actual pathogen, their immune system is prepared to respond swiftly, preventing or reducing the severity of the disease. Vaccines are a cornerstone of public health, offering long-term protection and contributing to herd immunity, which benefits the entire community.
In contrast, monoclonal antibodies are therapeutic agents targeted at high-risk or infected individuals, providing immediate but temporary protection or treatment. Unlike vaccines, which train the immune system, monoclonal antibodies are lab-created proteins that directly neutralize the pathogen, typically a virus, by binding to its spike proteins and preventing it from entering cells. This intervention is particularly crucial for individuals with compromised immune systems, such as the elderly, those with chronic illnesses, or immunocompromised patients, who may not mount an adequate response to a vaccine. Monoclonal antibodies are also used as a treatment for those already infected, helping to reduce the viral load and prevent severe disease progression.
The target population for vaccines is broad and includes healthy individuals of all ages, with specific formulations tailored to different demographics, such as children, adults, and the elderly. Vaccination campaigns focus on widespread distribution to achieve high immunization rates, which are essential for controlling the spread of infectious diseases. On the other hand, monoclonal antibodies are reserved for a narrower, more specific population: those at high risk of severe illness or complications, such as hospitalized COVID-19 patients or individuals with conditions that make vaccination less effective. This targeted approach ensures that resources are allocated efficiently to those who need them most.
Another key difference lies in the timing and duration of protection. Vaccines provide long-term immunity, often requiring multiple doses to build and maintain robust protection. Booster shots may be necessary to address waning immunity or new variants. Monoclonal antibodies, however, offer immediate but short-lived protection, typically lasting only a few weeks to months. They are not a substitute for vaccination but rather a complementary tool in the fight against infectious diseases, particularly for vulnerable populations.
In summary, vaccines are preventive tools for healthy individuals, fostering long-term immunity and community-wide protection, while monoclonal antibodies are therapeutic interventions for high-risk or infected patients, providing immediate but temporary relief. Understanding these differences is crucial for healthcare providers and policymakers to deploy these resources effectively, ensuring that both preventive and therapeutic measures are tailored to the needs of specific populations.
White House Employees: Vaccination Requirements and Protocols
You may want to see also
Explore related products






![]()
Immune Response: Vaccines rely on body’s response; monoclonal antibodies are lab-made, ready-to-use proteins
The immune response triggered by vaccines and monoclonal antibodies (mAbs) differs fundamentally in origin and mechanism. Vaccines are designed to stimulate the body’s own immune system to produce antibodies and memory cells. When a vaccine is administered, it introduces a harmless form of a pathogen (such as a weakened virus, protein subunit, or mRNA) to the immune system. This triggers an immune response where B cells are activated to produce antibodies specific to the pathogen. Over time, the immune system also develops memory cells, ensuring a faster and more effective response if the actual pathogen is encountered in the future. This process relies entirely on the body’s ability to mount an immune response, making vaccines a proactive and preventive measure.
In contrast, monoclonal antibodies are lab-made proteins engineered to serve as a direct and immediate defense against a specific pathogen. Unlike vaccines, mAbs do not require the body to produce its own antibodies. Instead, these ready-to-use proteins are administered directly into the bloodstream, where they bind to specific targets (such as viral proteins) to neutralize the pathogen or mark it for destruction by the immune system. This approach bypasses the need for the body to generate an immune response, providing instant protection. Monoclonal antibodies are particularly useful in treating active infections or in individuals with compromised immune systems who may not respond effectively to vaccines.
The key distinction lies in the timing and nature of the immune response. Vaccines are preventive and work by training the immune system over time, typically requiring weeks to build full immunity. They rely on the body’s natural ability to recognize and combat pathogens, fostering long-term immunity. Monoclonal antibodies, however, are therapeutic and provide immediate protection by delivering pre-made antibodies. Their effect is short-lived, as they do not confer lasting immunity or stimulate the production of memory cells. This makes mAbs a reactive tool rather than a preventive one.
Another critical difference is the specificity and versatility of these approaches. Vaccines often target multiple components of a pathogen, inducing a broad immune response that can adapt to variants. Monoclonal antibodies, on the other hand, are highly specific, targeting a single epitope on the pathogen. While this precision can be advantageous in treating specific infections, it also limits their effectiveness against mutations or variants that alter the target epitope. Additionally, vaccines are generally more cost-effective and scalable for population-wide use, whereas mAbs are resource-intensive to produce and administer, making them more suitable for targeted treatments.
In summary, vaccines and monoclonal antibodies represent distinct strategies for combating pathogens, each with unique strengths and limitations. Vaccines harness the body’s immune system to provide long-term, adaptive protection, while monoclonal antibodies offer immediate, lab-made solutions for direct intervention. Understanding these differences is crucial for determining the appropriate use of each in preventive and therapeutic contexts.
TDAP Vaccine Safety: Has It Been Tested on Pregnant Women?
You may want to see also
Frequently asked questions
Monoclonal antibodies are laboratory-made proteins designed to directly target and neutralize a specific pathogen, such as a virus, by binding to it. They provide immediate, passive immunity but are temporary, lasting only a few weeks to months. Vaccines, on the other hand, stimulate the body’s immune system to produce its own antibodies and memory cells, offering long-term active immunity against the pathogen.
No, monoclonal antibodies are primarily used as a treatment for individuals who are already infected or at high risk of severe disease. They are not a preventive measure like vaccines, which are administered to healthy individuals to prevent infection or reduce its severity before exposure.
Monoclonal antibodies provide immediate protection but their effects typically last only a few weeks to months, as they are gradually cleared from the body. Vaccines, however, offer longer-lasting protection, often for years, by training the immune system to recognize and fight the pathogen in the future. Booster doses may be needed to maintain immunity.