As the global effort to combat the COVID-19 pandemic continues, the rollout of vaccines has become a critical measure of each state's ability to protect its population and return to normalcy. Across the United States, states have adopted varying strategies for distributing vaccines, influenced by factors such as supply chain logistics, population density, and local healthcare infrastructure. While some states have achieved high vaccination rates, efficiently administering doses to a significant portion of their residents, others face challenges such as vaccine hesitancy, inequitable access, or logistical hurdles. Analyzing how each state is performing in its vaccine rollout provides valuable insights into the successes, disparities, and areas needing improvement in this unprecedented public health campaign.
Explore related products



$20.41 $21.95



What You'll Learn
- State-by-State Vaccination Rates: Compare doses administered per capita across all 50 states
- Equity in Distribution: Analyze access disparities based on race, income, and rural/urban areas
- Supply Chain Challenges: Examine delays, storage issues, and distribution bottlenecks in each state
- Hesitancy and Uptake: Assess vaccine acceptance rates and public health campaigns’ effectiveness
- Priority Group Progress: Track vaccination completion for seniors, healthcare workers, and essential workers
![]()
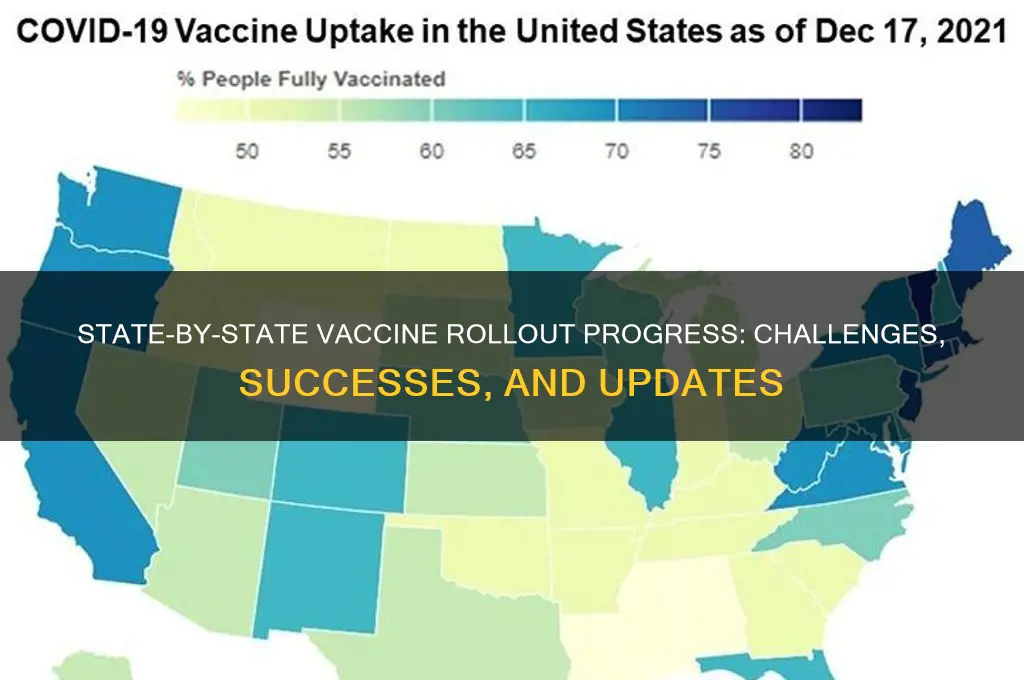
State-by-State Vaccination Rates: Compare doses administered per capita across all 50 states
As of the latest data, the United States has made significant progress in its COVID-19 vaccination efforts, but the rollout varies widely across the 50 states. When comparing doses administered per capita, it becomes clear that some states have outpaced others in vaccinating their populations. States like Vermont and Connecticut have consistently led the nation, with over 70% of their populations fully vaccinated. These states have implemented efficient distribution systems, leveraged strong public health infrastructure, and benefited from high public trust in vaccines. Vermont, in particular, has been praised for its targeted outreach to rural communities, ensuring equitable access to vaccines.
In contrast, states such as Mississippi and Alabama have lagged behind, with fully vaccinated rates below 50%. Factors contributing to slower rollouts in these states include vaccine hesitancy, limited healthcare access in rural areas, and lower investment in public health campaigns. Additionally, socioeconomic disparities and political attitudes toward vaccines have played a role in these states' slower uptake. Efforts to improve vaccination rates in these areas include mobile clinics, partnerships with community organizations, and incentives like lotteries or gift cards.
Midwestern states like Minnesota and Wisconsin have shown moderate success, with vaccination rates around 60-65%. These states have balanced urban and rural challenges, with denser populations in cities like Minneapolis and Milwaukee driving higher vaccination rates. However, rural areas in these states have faced logistical hurdles, such as transportation and storage of vaccines. Public-private partnerships and local health department initiatives have been key to bridging these gaps.
On the West Coast, California and Washington have demonstrated robust vaccination campaigns, with rates exceeding 70% in many counties. California’s large population and diverse demographics presented unique challenges, but the state’s early adoption of mass vaccination sites and digital appointment systems helped streamline the process. Washington State has also excelled, thanks to its strong public health network and proactive communication strategies. However, both states continue to address disparities in underserved communities.
Southern states like Florida and Texas have seen mixed results, with vaccination rates hovering around 55-60%. Florida’s rollout was initially criticized for its lack of organization, but the state has since improved access through walk-in clinics and partnerships with retail pharmacies. Texas faced early challenges with vaccine distribution during severe winter storms but has made strides by focusing on high-risk populations and expanding mobile vaccination units. Despite progress, both states grapple with significant pockets of vaccine hesitancy.
Overall, the state-by-state comparison of doses administered per capita highlights the impact of local leadership, public health infrastructure, and community engagement on vaccination success. While some states have achieved high coverage, others continue to face barriers that require tailored solutions. Understanding these disparities is crucial for policymakers and health officials working to close the vaccination gap nationwide.
Relieving Post-Vaccine Arm Soreness
You may want to see also
Explore related products






![]()
Equity in Distribution: Analyze access disparities based on race, income, and rural/urban areas
The rollout of COVID-19 vaccines in the United States has highlighted significant disparities in access, particularly along racial, economic, and geographic lines. Data from various states reveal that communities of color, low-income populations, and rural areas often face greater challenges in obtaining vaccines compared to their urban, wealthier, and white counterparts. For instance, in states like Mississippi and Alabama, where Black populations are substantial, early vaccination rates among Black residents lagged behind those of white residents, despite higher COVID-19 mortality rates in these communities. This disparity underscores systemic barriers, including limited access to healthcare facilities, transportation challenges, and vaccine hesitancy fueled by historical mistrust of medical institutions.
Income inequality further exacerbates these disparities. Wealthier neighborhoods, which often have better access to technology and healthcare infrastructure, have seen higher vaccination rates. In contrast, low-income areas, where residents may lack internet access or flexible work schedules, have struggled to secure appointments. States like California and New York have attempted to address this by prioritizing zip codes with lower socioeconomic status, but implementation has been inconsistent. Additionally, language barriers and lack of outreach in non-English speaking communities have left many immigrant populations, often low-income, underserved in the vaccine rollout.
Rural areas face unique challenges that urban centers do not. Limited healthcare infrastructure, longer travel distances to vaccination sites, and lower population density make distribution logistically difficult. States like Wyoming and Montana have reported slower vaccination rates in rural counties compared to urban ones. While mobile clinics and partnerships with local pharmacies have helped, these efforts are often underfunded and insufficient to meet demand. Furthermore, rural populations tend to be older and more susceptible to severe COVID-19 outcomes, making equitable distribution in these areas particularly critical.
Racial disparities persist even within urban areas. In cities like Chicago and Houston, vaccination rates in predominantly Black and Hispanic neighborhoods have trailed those in white neighborhoods. This gap is partly due to the concentration of vaccination sites in wealthier, whiter areas, leaving underserved communities with fewer options. Targeted outreach efforts, such as community-based vaccination events and partnerships with local leaders, have shown promise in bridging this divide, but such initiatives require sustained funding and political will.
To achieve equity in vaccine distribution, states must adopt data-driven, targeted strategies. This includes allocating resources based on need, ensuring culturally competent outreach, and addressing logistical barriers like transportation and scheduling. Transparency in reporting vaccination rates by race, income, and geographic area is essential to identify and rectify disparities. Ultimately, equitable distribution is not just a matter of fairness but a public health imperative to control the pandemic and prevent further loss of life.
When Do I Achieve Full Vaccination Status?
You may want to see also
Explore related products






![]()
Supply Chain Challenges: Examine delays, storage issues, and distribution bottlenecks in each state
The rollout of COVID-19 vaccines across the United States has been a monumental task, but it has not been without significant supply chain challenges. Each state has faced unique obstacles in ensuring timely delivery, proper storage, and efficient distribution of vaccines. One of the most common issues has been delays in vaccine supply, often stemming from manufacturing constraints and unpredictable allocation from the federal government. States like California and Texas, with large populations, have reported receiving fewer doses than needed, leading to appointment cancellations and public frustration. These delays have forced states to prioritize certain groups, such as healthcare workers and the elderly, while leaving others waiting longer than anticipated.
Storage issues have further complicated the vaccine rollout, particularly for mRNA vaccines like Pfizer-BioNTech, which require ultra-cold storage temperatures. States like Alaska and Montana, with vast rural areas, have struggled to transport and store vaccines effectively due to limited infrastructure and extreme weather conditions. In contrast, urban centers like New York and Illinois have faced challenges in maintaining the cold chain during the "last mile" of distribution, especially in densely populated areas where logistics are more complex. These storage requirements have led to wastage in some cases, as vaccines spoiled before they could be administered.
Distribution bottlenecks have also been a major hurdle, with many states grappling with how to equitably and efficiently get vaccines to their populations. In states like Florida and Georgia, centralized distribution models have led to long lines and confusion at mass vaccination sites. Meanwhile, decentralized approaches in states like Colorado and Washington have sometimes resulted in uneven distribution, with rural areas receiving fewer doses compared to urban centers. Additionally, the lack of a unified digital system for scheduling appointments has caused inefficiencies, leaving many residents unsure of when or where they can get vaccinated.
Another critical issue has been the workforce shortage in managing the supply chain. States like Michigan and Ohio have reported difficulties in hiring and training enough staff to handle vaccine administration, data entry, and logistics. This has slowed down the pace of vaccinations and exacerbated existing delays. Furthermore, the need for second doses has added another layer of complexity, requiring precise tracking and scheduling to ensure recipients return for their follow-up shots. Without adequate personnel, states have struggled to meet their vaccination targets.
Finally, equity in distribution has emerged as a significant supply chain challenge. States like Mississippi and Alabama, with higher proportions of underserved and minority populations, have faced barriers in reaching these communities due to limited access to transportation, technology, and healthcare facilities. Language and cultural barriers have also hindered outreach efforts, leading to lower vaccination rates in these groups. Addressing these disparities requires targeted strategies, such as mobile clinics and community partnerships, which many states are still working to implement effectively.
In summary, the supply chain challenges in the vaccine rollout vary widely across states but share common themes of delays, storage issues, distribution bottlenecks, workforce shortages, and equity concerns. Overcoming these obstacles will require continued collaboration between federal, state, and local authorities, as well as innovative solutions to ensure that vaccines reach all Americans efficiently and equitably.
Delay Puppy Vaccinations: Why Wait Until 10 Weeks is Crucial
You may want to see also
Explore related products






![]()
Hesitancy and Uptake: Assess vaccine acceptance rates and public health campaigns’ effectiveness
Vaccine hesitancy remains a significant challenge in the rollout of COVID-19 vaccines across the United States, with acceptance rates varying widely by state. States like Vermont and Massachusetts have reported high vaccination rates, with over 70% of their populations fully vaccinated, partly due to strong public trust in health authorities and effective communication strategies. In contrast, states such as Mississippi and Alabama have struggled, with vaccination rates below 50%, often linked to higher levels of skepticism, misinformation, and historical distrust of medical institutions, particularly in underserved communities. Understanding these disparities is crucial for tailoring public health campaigns to address specific concerns and improve uptake.
Public health campaigns have played a pivotal role in combating hesitancy, but their effectiveness varies by state. Successful campaigns, such as California’s "California for All" initiative, have utilized multilingual messaging, community partnerships, and local influencers to build trust and dispel myths. Similarly, New York’s "Vax for Facts" campaign leveraged data transparency and expert testimonials to reassure the public. However, in states like Wyoming and Idaho, where hesitancy is deeply rooted in political and cultural beliefs, traditional campaigns have had limited impact. This highlights the need for hyper-localized strategies that resonate with specific communities and address their unique concerns.
The role of local leaders and healthcare providers cannot be overstated in influencing vaccine uptake. In states like West Virginia, early success in vaccination rates was attributed to the proactive involvement of local pharmacists and community leaders who personally advocated for the vaccine. Conversely, in states where political leaders have expressed ambivalence or skepticism, vaccination rates have lagged. Public health officials must collaborate with trusted figures, including religious leaders, educators, and local celebrities, to amplify positive messaging and counteract misinformation.
Data-driven approaches are essential for assessing the effectiveness of public health campaigns. States like Colorado have employed real-time surveys and social media analytics to monitor public sentiment and adjust their strategies accordingly. For instance, identifying pockets of hesitancy through ZIP code-level data has allowed targeted interventions in underserved areas. However, many states lack the resources for such granular analysis, leading to one-size-fits-all approaches that fall short. Investing in robust data collection and analysis tools is critical for refining campaigns and maximizing their impact.
Finally, addressing vaccine hesitancy requires a long-term commitment to health literacy and community engagement. States like Minnesota have launched educational programs in schools and workplaces to foster a broader understanding of vaccine science and public health. By integrating these efforts into ongoing health initiatives, states can build resilience against future health crises. Ultimately, the effectiveness of public health campaigns hinges on their ability to adapt to local contexts, engage with communities authentically, and provide clear, consistent information that empowers individuals to make informed decisions.
Global Vaccine Progress: How Other Countries Are Faring in 2023
You may want to see also
Explore related products






![]()
Priority Group Progress: Track vaccination completion for seniors, healthcare workers, and essential workers
As of the latest data, the progress of vaccine rollout across U.S. states varies significantly, particularly in terms of Priority Group Progress—specifically, the vaccination completion rates for seniors, healthcare workers, and essential workers. These groups were identified early on as critical to protecting public health and maintaining essential services. States like Connecticut and New Hampshire have reported high completion rates for seniors (aged 65+), with over 90% fully vaccinated, thanks to targeted outreach programs and accessible vaccination sites. In contrast, states such as Mississippi and Alabama lag behind, with senior vaccination rates hovering around 75%, highlighting disparities in healthcare access and vaccine hesitancy.
Healthcare workers, the first priority group in most states, have seen relatively high vaccination completion rates nationwide, with states like Rhode Island and Vermont reporting over 95% fully vaccinated among this group. However, pockets of resistance remain, particularly in states with lower overall vaccination rates. For instance, in Wyoming and Idaho, healthcare worker vaccination rates are closer to 80%, raising concerns about workforce protection and patient safety. Efforts to address this gap include workplace mandates and educational campaigns emphasizing the safety and efficacy of vaccines.
Essential workers, a broader and more diverse group, have experienced more uneven progress. States like California and New York have made strides, with over 80% of essential workers fully vaccinated, driven by large-scale vaccination sites and employer partnerships. Conversely, in Georgia and South Carolina, essential worker vaccination rates are below 70%, reflecting challenges such as scheduling flexibility, language barriers, and mistrust. Mobile clinics and community-based initiatives are being deployed to improve access and build trust in these areas.
Tracking Priority Group Progress requires robust data collection and transparency, which some states have excelled at while others struggle. For example, Minnesota and Washington provide detailed dashboards breaking down vaccination rates by occupation and age group, enabling targeted interventions. In contrast, states like Texas and Florida have faced criticism for less transparent reporting, making it harder to assess progress and address gaps. Standardizing data reporting across states could improve accountability and ensure equitable vaccine distribution.
Finally, disparities in Priority Group Progress often correlate with broader socioeconomic and geographic factors. Rural states like Montana and West Virginia face unique challenges, including limited healthcare infrastructure and higher rates of vaccine hesitancy, which slow progress for all priority groups. Urban states, while generally ahead, still grapple with inequities among marginalized communities. Addressing these disparities requires tailored strategies, such as culturally sensitive outreach and incentives for underserved populations. Monitoring and addressing these gaps will be crucial as states transition to broader population vaccination efforts.
Vaccination Injuries and Illnesses: Real Risks or Rare Occurrences?
You may want to see also
Frequently asked questions
Most states provide regular updates on their official health department websites, including dashboards with vaccination data. You can also check the CDC's (Centers for Disease Control and Prevention) COVID Data Tracker for state-by-state vaccination rates and trends.
While the CDC provides guidelines, each state has the autonomy to develop its own distribution plan. This means that eligibility criteria, priority groups, and rollout strategies may vary. Some states have chosen to follow a phased approach, while others have opened up vaccinations to all adults earlier.
Several factors contribute to the variation in vaccine rollout across states. These include population density, healthcare infrastructure, supply chain logistics, and local policies. States with larger populations and more rural areas might face challenges in distributing vaccines evenly, while others with well-established healthcare systems may have an advantage in administering doses quickly. Additionally, each state's approach to prioritizing different age groups or at-risk populations can impact the overall pace of vaccination.