The polio vaccine, a cornerstone in the global eradication of poliomyelitis, is administered through two primary methods: the inactivated poliovirus vaccine (IPV) and the oral poliovirus vaccine (OPV). IPV, given as an injection, typically in the leg or arm, contains inactivated (killed) poliovirus and is commonly used in countries with a low risk of polio. OPV, on the other hand, is delivered orally in the form of drops and uses a weakened form of the virus, offering both individual protection and the ability to interrupt person-to-person transmission in communities. The choice of vaccine and administration method depends on factors such as regional polio prevalence, healthcare infrastructure, and public health strategies aimed at achieving and maintaining polio-free status worldwide.
| Characteristics | Values |
|---|---|
| Route of Administration | Oral (OPV - Oral Polio Vaccine) or Injectable (IPV - Inactivated Polio Vaccine) |
| Oral Polio Vaccine (OPV) | Administered as drops in the mouth, typically 2 drops per dose. |
| Injectable Polio Vaccine (IPV) | Administered via intramuscular or subcutaneous injection, usually in the thigh or upper arm. |
| Dosage for OPV | Varies by age: infants (2 drops), children (2 drops), adults (rarely used). |
| Dosage for IPV | 0.5 mL for children and adults, given as a single dose or part of a combination vaccine. |
| Primary Series (OPV) | 3–4 doses starting at 6 weeks of age, with intervals of 4–8 weeks. |
| Primary Series (IPV) | 3–4 doses starting at 2 months of age, with intervals of 4–8 weeks. |
| Booster Doses | 1–2 booster doses recommended during childhood (varies by country). |
| Age Groups | Infants, children, and adults (IPV primarily for children, OPV for outbreaks). |
| Storage Requirements | OPV: 2–8°C (refrigerated); IPV: 2–8°C (refrigerated). |
| Shelf Life | OPV: 12–24 months; IPV: 24–36 months (varies by manufacturer). |
| Common Side Effects (OPV) | Mild fever, sore throat, or temporary vaccine-derived poliovirus (rare). |
| Common Side Effects (IPV) | Pain, redness, or swelling at the injection site, mild fever. |
| Global Usage | OPV: Primarily in endemic regions; IPV: Widely used in polio-free countries. |
| WHO Recommendation | Both OPV and IPV are endorsed, with a shift toward IPV in polio-free areas. |
Explore related products






What You'll Learn
![]()
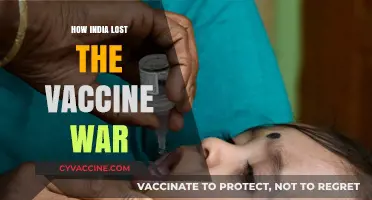
Oral drops for children
Oral polio vaccine (OPV) drops are a cornerstone of global polio eradication efforts, particularly for children under five. Administered as two drops per dose, OPV is designed to be simple, cost-effective, and easily scalable for mass immunization campaigns. The vaccine contains live, attenuated (weakened) polioviruses that stimulate immunity in the gut, preventing the virus from replicating and shedding, thus halting its spread. This method is ideal for young children because it requires no needles, making it less intimidating and more accessible in resource-limited settings.
The dosage for OPV is consistent across age groups: two drops per dose, typically given multiple times to ensure robust immunity. For infants, the World Health Organization (WHO) recommends the first dose at 6 weeks of age, followed by additional doses at 10 weeks, 14 weeks, and a booster at 15–18 months. In polio-endemic or high-risk areas, supplementary immunization activities (SIAs) may provide additional doses to children up to 5 years old. The drops are administered directly into the mouth, often using a dropper or a marked vaccine vial monitor to ensure accuracy. Parents and caregivers are advised to avoid feeding or giving water to the child immediately before or after administration to maximize absorption.
One of the key advantages of OPV drops is their ability to induce both humoral (blood-based) and mucosal immunity, which is critical for blocking viral transmission in communities. However, this live vaccine carries a rare risk of vaccine-associated paralytic polio (VAPP), occurring in approximately 1 in 2.7 million doses. Despite this, the benefits of OPV in preventing wild poliovirus outbreaks far outweigh the risks, particularly in regions with low vaccination coverage. In recent years, the global shift toward inactivated polio vaccine (IPV) in routine immunization schedules has aimed to mitigate VAPP while maintaining herd immunity.
Practical tips for administering OPV drops include ensuring the vaccine is stored at the correct temperature (2°C–8°C) to maintain potency and using a clean, dry dropper to avoid contamination. Health workers should demonstrate the correct technique to caregivers, emphasizing the importance of delivering the full dose directly into the child’s mouth. In mass campaigns, marking the child’s finger or toenail with ink after vaccination helps track coverage and prevent missed doses. For parents, understanding the vaccine’s role in protecting not just their child but the entire community can foster trust and compliance.
While OPV drops have been instrumental in reducing polio cases by 99% since 1988, their success relies on high vaccination coverage and sustained efforts. The transition to IPV in some regions highlights the evolving strategies in polio eradication, but OPV remains indispensable in areas where the virus persists. By combining oral drops with robust surveillance and community engagement, the goal of a polio-free world remains within reach. For children, these drops represent more than a vaccine—they are a lifeline to a healthier, polio-free future.
Lying on Child Vaccination Records: Consequences, Risks, and Legal Implications
You may want to see also
Explore related products






![]()
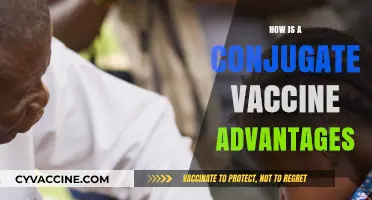
Injected dose for adults
The injected polio vaccine, known as the inactivated poliovirus vaccine (IPV), is a critical tool for adults in regions where polio remains a threat or for travelers to such areas. Unlike the oral vaccine, which uses a weakened live virus, IPV contains no live virus, making it safer for individuals with weakened immune systems. For adults, the typical dose is 0.5 milliliters, administered intramuscularly, usually in the deltoid muscle of the upper arm or the vastus lateralis muscle of the thigh. This method ensures the vaccine is absorbed efficiently, triggering a robust immune response without the risk of vaccine-derived poliovirus.
Administering IPV to adults follows a specific protocol to maximize efficacy. The vaccine is often given as part of a combination vaccine, such as DTaP-IPV, which protects against diphtheria, tetanus, pertussis, and polio simultaneously. For adults who have not completed their polio vaccination series, a three-dose schedule is recommended: the first dose at any time, the second dose 1–2 months later, and the third dose 6–12 months after the second. This spacing allows the immune system to build and retain immunity effectively. Healthcare providers must ensure the vaccine is stored at 2°C to 8°C and shaken well before administration to maintain its potency.
One key consideration for adults receiving IPV is their vaccination history. Those who received the oral polio vaccine (OPV) in childhood may still need IPV, as OPV provides intestinal immunity but not systemic protection. Adults traveling to polio-endemic countries should receive a single booster dose of IPV, even if they were vaccinated as children. This precaution is particularly important due to the risk of exposure to wild poliovirus or vaccine-derived strains in such regions. Pregnant women, immunocompromised individuals, and those with allergies to vaccine components should consult a healthcare provider before receiving IPV.
Practical tips for adults receiving IPV include wearing loose clothing to allow easy access to the injection site and planning the vaccination well in advance of travel, as immunity takes several weeks to develop fully. Mild side effects, such as soreness at the injection site, fatigue, or a low-grade fever, are common and typically resolve within a few days. While rare, severe allergic reactions require immediate medical attention. By adhering to the recommended dosage and schedule, adults can ensure they are adequately protected against polio, contributing to global eradication efforts.
Vaccination Testing: How Doctors Verify Immunity and Vaccine Effectiveness
You may want to see also
Explore related products






![]()
Multiple doses required
The polio vaccine's effectiveness hinges on a critical factor: multiple doses. This isn't a one-and-done scenario. Unlike some vaccines that offer protection after a single shot, polio requires a series of doses to build robust immunity. This multi-dose approach is a cornerstone of polio eradication efforts, ensuring individuals develop the antibodies needed to fight off the poliovirus effectively.
Understanding the dosing schedule is crucial for both healthcare providers and individuals seeking protection.
The specific number of doses and the timing between them vary depending on the type of polio vaccine used. The inactivated poliovirus vaccine (IPV), administered through injection, typically requires a series of three or four doses. In many countries, infants receive their first dose at two months of age, followed by subsequent doses at four months and six to 18 months. A booster dose is often recommended between the ages of four and six years. Oral poliovirus vaccine (OPV), delivered as drops, usually involves a series of four doses, starting at six weeks of age with a one-month interval between doses.
This multi-dose regimen is designed to prime the immune system gradually. The initial dose introduces the weakened or inactivated virus, prompting the body to produce antibodies. Subsequent doses reinforce this immune response, significantly increasing the level of protective antibodies. This cumulative effect is vital because polio is a highly contagious disease, and even a small number of unprotected individuals can pose a risk to the wider community.
The need for multiple doses underscores the importance of adherence to the vaccination schedule. Missing doses can leave individuals vulnerable to infection. Public health initiatives often focus on ensuring access to all required doses, particularly in regions where polio remains endemic.
While the multi-dose approach may seem inconvenient, it's a proven strategy for achieving long-lasting immunity against polio. The success of global polio eradication efforts is a testament to the power of this approach. By understanding the rationale behind multiple doses and adhering to the recommended schedule, individuals can play a vital role in protecting themselves and contributing to the global fight against this debilitating disease.
Tetanus Vaccination Frequency: How Often Should You Get the Shot?
You may want to see also
Explore related products






![]()
Trained healthcare worker administration
The administration of the polio vaccine by trained healthcare workers is a critical component in ensuring its effectiveness and safety. These professionals are equipped with the knowledge and skills to handle the vaccine properly, from storage to injection, minimizing the risk of contamination or error. For instance, the inactivated polio vaccine (IPV) requires storage at 2°C to 8°C, and healthcare workers are trained to maintain this temperature range to preserve the vaccine’s potency. This attention to detail is essential, as even minor deviations can compromise the vaccine’s efficacy.
In practice, trained healthcare workers follow a strict protocol when administering the polio vaccine. For children under 5 years old, the most common recipients, the vaccine is typically given as an intramuscular injection in the vastus lateralis muscle of the thigh or the deltoid muscle of the upper arm. The dosage varies by age: infants receive 0.1 mL of IPV, while older children and adults receive 0.5 mL. Healthcare workers are trained to select the appropriate needle length—5/8 inch for infants and 1 inch for older children—to ensure the vaccine reaches the correct muscle tissue. This precision is vital to maximize immune response and minimize discomfort.
One of the key advantages of having trained healthcare workers administer the polio vaccine is their ability to address patient concerns and provide education. For example, they can explain the difference between IPV and the oral polio vaccine (OPV), clarifying that IPV is the standard in many countries due to its safety profile and inability to cause vaccine-derived poliovirus. This transparency builds trust and encourages vaccination uptake, particularly in communities where vaccine hesitancy may be a barrier. Healthcare workers also monitor for immediate adverse reactions, such as allergic responses, ensuring prompt intervention if needed.
Comparatively, while community health workers or volunteers can play a role in vaccine distribution, especially in mass campaigns, their involvement is often limited to oral vaccines like OPV. Trained healthcare workers, however, are indispensable for injectable vaccines like IPV. Their expertise ensures adherence to global health standards, such as those set by the World Health Organization (WHO), which recommends IPV as part of routine immunization schedules. This distinction highlights the irreplaceable role of trained professionals in maintaining the integrity of polio vaccination programs.
In conclusion, the administration of the polio vaccine by trained healthcare workers is a cornerstone of successful immunization efforts. Their technical proficiency, from proper storage to precise injection techniques, ensures the vaccine’s effectiveness. Equally important is their ability to educate and reassure patients, fostering confidence in the vaccination process. As the world nears polio eradication, the role of these professionals remains pivotal in delivering the final blows to this debilitating disease.
Is the CDC Altering 'Fully Vaccinated' Definition? What You Need to Know
You may want to see also
Explore related products






![]()
Cold chain storage essential
The polio vaccine's potency hinges on maintaining a precise temperature range from production to administration. This is where cold chain storage becomes indispensable. The oral polio vaccine (OPV), the most commonly used form, must be kept between 2°C and 8°C (36°F and 46°F) at all times. Even brief exposure to higher temperatures can render the vaccine ineffective, compromising its ability to confer immunity. For the inactivated polio vaccine (IPV), which is administered via injection, the temperature requirements are equally stringent, though it is generally more stable than OPV. Ensuring this continuous refrigeration is a logistical challenge, especially in remote or resource-limited areas, but it is non-negotiable for the vaccine’s efficacy.
Consider the journey of a polio vaccine vial: from the manufacturer, it travels through a network of storage facilities, transport vehicles, and health clinics before reaching the recipient. Each step requires meticulous temperature monitoring and control. For instance, vaccine carriers equipped with ice packs or cold boxes are essential for transporting doses to immunization sites, particularly in regions without reliable electricity. Health workers must also adhere to strict protocols, such as minimizing the time vaccine vials spend outside the cold chain during administration. A single lapse can jeopardize an entire batch, potentially leaving individuals unprotected against this highly contagious disease.
The importance of cold chain storage is underscored by the vaccine’s dosage requirements. OPV is typically administered in multiple doses, starting as early as 6 weeks of age, with subsequent doses given at 4-month intervals. IPV, often used in combination with other vaccines, follows a similar schedule. If any dose is compromised due to improper storage, the entire immunization series may be ineffective, leaving gaps in immunity. This is particularly critical in polio eradication efforts, where herd immunity depends on high vaccination coverage and individual protection.
Practical tips for maintaining the cold chain include regular calibration of refrigerators and temperature loggers, using vaccine carriers with sufficient cold life, and training health workers to handle vaccines properly. In areas with frequent power outages, backup power sources or solar-powered refrigerators can be lifesavers. Additionally, digital monitoring systems that track temperature in real-time can alert health officials to potential breaches, allowing for swift corrective action. These measures, while resource-intensive, are essential for ensuring that every dose of the polio vaccine delivers its intended protection.
Ultimately, cold chain storage is not just a logistical requirement but a cornerstone of polio vaccination programs. Without it, the vaccine’s ability to prevent this debilitating disease is severely compromised. As global health efforts continue to push toward polio eradication, maintaining the integrity of the cold chain remains a critical priority, ensuring that every child, regardless of location, receives a potent and effective vaccine.
Pneumonia Vaccine: Why Some Serotypes Remain Unchanged Post-Vaccination
You may want to see also
Frequently asked questions
The polio vaccine can be administered either orally (OPV - Oral Polio Vaccine) as drops or by injection (IPV - Inactivated Polio Vaccine). The method depends on the vaccine type and the country's immunization program.
No, the polio vaccine requires multiple doses for full protection. The number and schedule of doses vary depending on the vaccine type (OPV or IPV) and the age of the recipient, as recommended by local health authorities.
Yes, the polio vaccine is typically given to infants starting at 6 weeks of age. The oral vaccine (OPV) is administered as drops in the mouth, while the injectable vaccine (IPV) is given as a shot in the leg or arm, depending on the child's age.