A conjugate vaccine is created by chemically linking a weak antigen (such as a polysaccharide from a bacterium) to a strong antigen (typically a protein carrier) to enhance the immune response. This process begins with isolating the polysaccharide from the pathogen's surface and purifying it. The polysaccharide is then chemically modified to introduce reactive functional groups, allowing it to covalently bond with the carrier protein. The carrier protein, often derived from a non-pathogenic source, is chosen for its ability to elicit a robust immune reaction. Once conjugated, the resulting complex is purified and formulated into a vaccine. This method improves the vaccine's efficacy, particularly in young children and the elderly, by enabling the immune system to recognize and respond more effectively to the polysaccharide antigen.
| Characteristics | Values |
|---|---|
| Definition | A conjugate vaccine combines a weak antigen (polysaccharide) with a carrier protein to enhance immune response. |
| Target Antigens | Polysaccharides from bacterial capsules (e.g., Streptococcus pneumoniae, Neisseria meningitidis). |
| Carrier Proteins | Foreign proteins like CRM197 (detoxified diphtheria toxin), tetanus toxoid, or meningococcal proteins. |
| Conjugation Method | Chemical linkage using cross-linking agents (e.g., cyanogen bromide, glutaraldehyde). |
| Immune Response | Induces T-cell-dependent immunity, leading to higher antibody production, immunological memory, and improved efficacy in infants. |
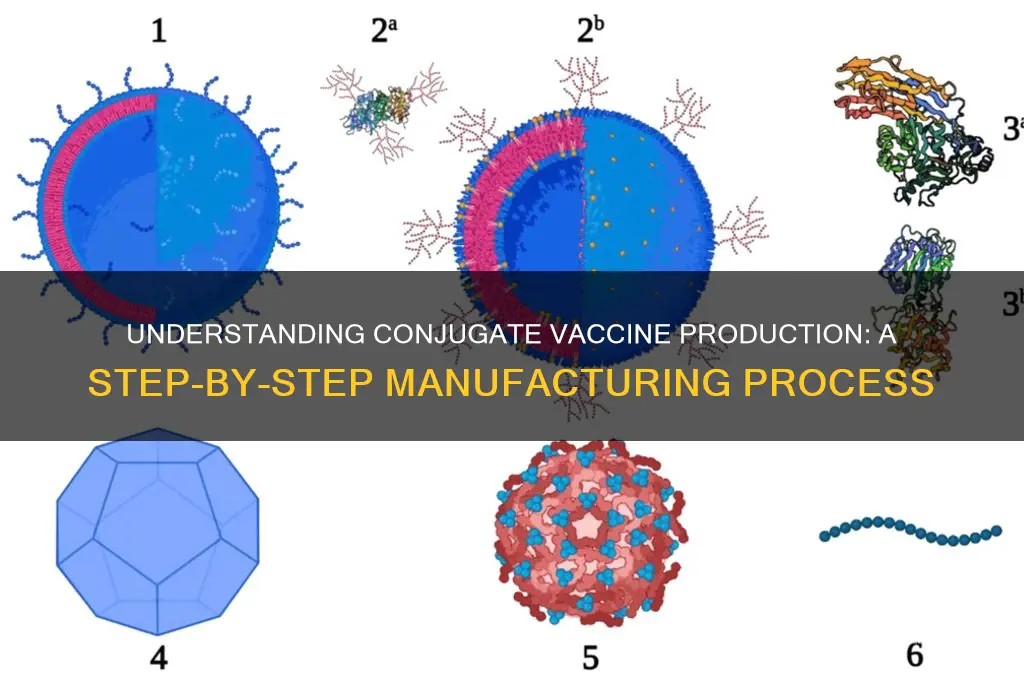
| Manufacturing Steps | 1. Isolation of polysaccharides and carrier proteins. 2. Activation of both components. 3. Conjugation. 4. Purification. 5. Formulation with adjuvants (if needed). |
| Stability | Enhanced stability compared to plain polysaccharide vaccines due to protein conjugation. |
| Efficacy in Infants | Highly effective in infants and young children, unlike plain polysaccharide vaccines. |
| Examples | Prevnar 13 (pneumococcal), Menactra (meningococcal), Hib (Haemophilus influenzae type b). |
| Advantages | Longer-lasting immunity, reduced disease burden, effective in younger populations. |
| Challenges | Complex manufacturing process, higher production costs. |
Explore related products






What You'll Learn
- Antigen Identification: Selecting specific pathogen components (e.g., proteins, polysaccharides) to target for immune response
- Carrier Protein Selection: Choosing a protein (e.g., CRM197) to conjugate with weak antigens for enhanced immunity
- Conjugation Process: Chemically linking the antigen to the carrier protein using stable, immunogenic bonds
- Purification Steps: Removing impurities and unconjugated materials to ensure vaccine safety and efficacy
- Formulation & Testing: Adding adjuvants, stabilizing the vaccine, and conducting trials for safety and immunogenicity
![]()
Antigen Identification: Selecting specific pathogen components (e.g., proteins, polysaccharides) to target for immune response
The first step in crafting a conjugate vaccine is pinpointing the precise molecular targets that will provoke a robust immune response. This process, known as antigen identification, involves a meticulous selection of pathogen components—typically proteins or polysaccharides—that are both immunogenic and essential to the pathogen's survival. For instance, in the case of the *Haemophilus influenzae* type b (Hib) conjugate vaccine, the polysaccharide capsule surrounding the bacterium is the primary target. However, since infants under 2 years old often fail to mount a strong immune response to this polysaccharide alone, it is chemically linked to a carrier protein, such as tetanus toxoid, to enhance immunogenicity.
Consider the analytical approach: not all pathogen components are created equal. Proteins, with their complex structures, often elicit strong T-cell-dependent immune responses, making them ideal candidates for vaccines targeting viruses like influenza or SARS-CoV-2. Polysaccharides, on the other hand, are T-cell-independent antigens, meaning they typically provoke a weaker and less durable response, especially in young children. This distinction underscores the importance of selecting antigens based on both their role in the pathogen's virulence and the immune system's ability to recognize and respond to them. For example, the pneumococcal conjugate vaccine (PCV13) targets 13 serotypes of *Streptococcus pneumoniae* by coupling their polysaccharide capsules to a carrier protein, ensuring a robust immune response even in infants as young as 6 weeks old.
From an instructive perspective, antigen identification requires a multi-step process. First, researchers analyze the pathogen's genome and proteome to identify surface-exposed molecules that are conserved across strains, ensuring broad protection. Next, they assess these candidates for immunogenicity using in vitro and in vivo models. For instance, the meningococcal conjugate vaccine (MenACWY) targets four serogroups of *Neisseria meningitidis* by selecting specific polysaccharides from their capsules. These polysaccharides are then conjugated to a carrier protein like diphtheria toxoid, with each dose containing 4–50 µg of polysaccharide per serogroup, depending on the formulation and age group.
A persuasive argument for careful antigen selection lies in its impact on vaccine efficacy and safety. Poorly chosen antigens can lead to inadequate immune responses or even immune tolerance, as seen in early attempts to vaccinate against *Staphylococcus aureus* using capsular polysaccharides alone. By contrast, the success of the Hib conjugate vaccine, which reduced invasive Hib disease by over 90% in vaccinated populations, highlights the transformative potential of precise antigen identification. Practical tips for researchers include prioritizing antigens that are less prone to mutation and ensuring that the chosen components do not induce adverse reactions, such as antibody-dependent enhancement.
Finally, a comparative analysis reveals that antigen identification is both an art and a science. While proteins are often favored for their ability to elicit long-lasting immunity, polysaccharides remain critical for targeting encapsulated bacteria. The choice between them—or a combination of both—depends on the pathogen's biology, the target population's immune maturity, and the desired duration of protection. For example, the *Streptococcus agalactiae* (Group B Streptococcus) vaccine candidates currently in development focus on protein antigens due to the limitations of its polysaccharide capsule in eliciting a protective response in newborns. This nuanced decision-making process underscores the complexity and importance of antigen identification in the creation of effective conjugate vaccines.
TIG and Tetanus Vaccine: Combined Prevention Against Tetanus Infections?
You may want to see also
Explore related products






![]()
Carrier Protein Selection: Choosing a protein (e.g., CRM197) to conjugate with weak antigens for enhanced immunity
Conjugate vaccines hinge on the strategic pairing of a weak antigen with a robust carrier protein to elicit a potent immune response. Among the array of carrier proteins available, CRM197 stands out as a gold standard due to its non-toxicity, immunogenicity, and well-established safety profile. Derived from *Corynebacterium diphtheriae*, CRM197 lacks enzymatic activity, making it safe for use in vaccines while retaining its ability to stimulate the immune system. Its success in vaccines like Prevnar 13, which targets pneumococcal disease, underscores its reliability in enhancing antibody production against co-administered antigens.
Selecting the right carrier protein involves more than just immunogenicity; it requires careful consideration of factors like allergenicity, stability, and manufacturing scalability. For instance, CRM197’s consistent performance across age groups, from infants to the elderly, makes it a versatile choice. However, alternatives like tetanus toxoid or diphtheria toxoid may be preferred in specific contexts, such as when leveraging pre-existing immunity in certain populations. The choice ultimately depends on the target antigen, the intended demographic, and the desired immune response—humoral, cellular, or both.
A critical step in carrier protein selection is ensuring compatibility with the conjugation process. Chemical methods, such as reductive amination, are commonly used to link the carrier protein to the antigen. CRM197’s lysine residues, for example, provide ample sites for conjugation, allowing for efficient coupling with polysaccharides or other weak antigens. Proper conjugation not only stabilizes the antigen but also promotes its presentation to immune cells, amplifying the response. Manufacturers must optimize conjugation conditions to maintain protein integrity and avoid denaturation, which could compromise vaccine efficacy.
Practical considerations also play a pivotal role in carrier protein selection. For pediatric vaccines, where multiple doses are often required, the carrier protein must be well-tolerated and non-reactogenic. CRM197’s minimal side effect profile makes it ideal for this purpose, as evidenced by its use in infant immunization schedules. Additionally, cost-effectiveness and availability of the carrier protein are crucial for global vaccine distribution. While CRM197 is widely used, emerging carriers like recombinant proteins or synthetic peptides may offer advantages in terms of production efficiency and customization.
In conclusion, carrier protein selection is a nuanced process that balances immunological efficacy, safety, and practicality. CRM197 exemplifies the ideal carrier, combining proven immunogenicity with a strong safety record. However, the choice should always be tailored to the specific vaccine’s goals and target population. By carefully evaluating these factors, vaccine developers can maximize the potential of conjugate vaccines to protect against infectious diseases effectively.
Meningococcal Vaccine: What's in a Name?
You may want to see also
Explore related products






![]()
Conjugation Process: Chemically linking the antigen to the carrier protein using stable, immunogenic bonds
The conjugation process is a delicate dance of chemistry, where the antigen—often a polysaccharide from a bacterium—is tethered to a carrier protein through stable, immunogenic bonds. This linkage transforms the weak immunogenicity of the standalone antigen into a potent stimulus for the immune system. For instance, in the Haemophilus influenzae type b (Hib) vaccine, the polysaccharide antigen is conjugated to the diphtheria toxoid or tetanus toxoid, proteins already known to provoke a robust immune response. The chemical reaction typically involves activation of the antigen with reagents like cyanogen bromide or carbodiimide, followed by coupling to the carrier protein under controlled pH and temperature conditions. Precision is paramount; even slight variations can alter bond stability or immunogenicity, rendering the vaccine ineffective.
Consider the step-by-step approach to conjugation: first, purify both the antigen and carrier protein to remove impurities that could interfere with bonding. Next, activate the antigen using a cross-linking agent, such as 1-ethyl-3-(3-dimethylaminopropyl)carbodiimide (EDC), which facilitates the formation of covalent bonds. The activated antigen is then mixed with the carrier protein in a buffer solution optimized for pH and ionic strength. After conjugation, the product undergoes rigorous purification to remove unreacted components and ensure only stable, immunogenic complexes remain. Quality control is critical; techniques like high-performance liquid chromatography (HPLC) and mass spectrometry verify the integrity of the conjugate. This meticulous process ensures the vaccine not only elicits a strong immune response but also maintains safety for administration, typically in doses of 0.5 mL for infants and children.
A comparative analysis highlights the advantages of conjugation over traditional vaccines. Standalone polysaccharide vaccines, like the early pneumococcal vaccine, were poorly immunogenic in infants under two years old because their immature immune systems could not recognize polysaccharides effectively. Conjugation to a carrier protein bypasses this limitation by engaging T-cell help, amplifying the immune response. For example, the pneumococcal conjugate vaccine (PCV13) links 13 pneumococcal polysaccharides to a non-toxic variant of diphtheria toxin, resulting in a vaccine that is 90% effective in preventing invasive pneumococcal disease in children. This innovation underscores the transformative power of conjugation in modern vaccinology.
Practical tips for optimizing the conjugation process include selecting a carrier protein with a proven safety profile and strong immunogenicity, such as CRM197 (a detoxified form of diphtheria toxin). Ensure the antigen-to-protein ratio is carefully calibrated; an excess of antigen can lead to incomplete conjugation, while too little may reduce immunogenicity. Storage conditions post-conjugation are equally vital—conjugate vaccines are typically stored at 2–8°C to preserve bond stability. For healthcare providers, administering conjugate vaccines within the recommended age-specific schedules (e.g., Hib vaccine at 2, 4, 6, and 12–15 months) maximizes their protective efficacy. By mastering these nuances, scientists and clinicians can harness the full potential of conjugation to combat infectious diseases.
Michigan Vaccine Booking Guide: Easy Steps to Secure Your Appointment
You may want to see also
Explore related products






![]()
Purification Steps: Removing impurities and unconjugated materials to ensure vaccine safety and efficacy
Impurities and unconjugated materials in a vaccine can compromise its safety and efficacy, triggering adverse reactions or reducing immunogenicity. Purification steps are therefore critical in the production of conjugate vaccines, ensuring that only the intended antigen-carrier complex remains in the final product. These steps involve a series of carefully designed processes to separate, isolate, and remove unwanted components, such as unreacted antigens, carriers, or by-products of the conjugation reaction.
One common purification technique is size-exclusion chromatography, which separates molecules based on their size and shape. In this process, the conjugate vaccine mixture is passed through a porous resin, where smaller impurities and unconjugated materials are retained, while the larger, properly conjugated complexes elute through the column. This method is particularly effective in removing low-molecular-weight contaminants, ensuring a more homogeneous vaccine product. For instance, in the production of the pneumococcal conjugate vaccine (PCV), size-exclusion chromatography is used to isolate the polysaccharide-protein conjugate from unreacted components, resulting in a final product with a well-defined size distribution.
Another crucial purification step is dialysis, which removes small molecules and salts by diffusing them through a semi-permeable membrane. This process is often used to eliminate excess reagents, such as activating agents or buffers, that may remain after the conjugation reaction. Dialysis is especially important in vaccines intended for pediatric populations, where even trace amounts of impurities could pose a risk. For example, the Haemophilus influenzae type b (Hib) conjugate vaccine undergoes dialysis to remove residual cyanoborohydride, a reducing agent used in the conjugation process, ensuring the vaccine is safe for administration to infants as young as 2 months old.
Tangential flow filtration (TFF) is a more advanced purification method that combines filtration and recirculation to separate particles based on size. This technique is highly efficient in concentrating the conjugate vaccine while removing impurities and unconjugated materials. TFF is particularly useful in large-scale vaccine production, where consistency and scalability are essential. For the meningococcal conjugate vaccine, TFF is employed to achieve a precise antigen concentration, typically ranging from 10 to 20 µg per dose, ensuring optimal immunogenicity while minimizing adverse effects.
Despite the effectiveness of these purification steps, they must be meticulously validated to ensure their reliability. Quality control assays, such as high-performance liquid chromatography (HPLC) and enzyme-linked immunosorbent assay (ELISA), are used to confirm the removal of impurities and the integrity of the conjugate. These assays provide quantitative data on the purity and potency of the vaccine, ensuring it meets regulatory standards. For instance, the diphtheria toxoid-based conjugate vaccines require HPLC analysis to verify that the ratio of polysaccharide to protein falls within the specified range, typically 1:1 to 2:1, to guarantee both safety and efficacy.
In conclusion, purification steps are a cornerstone of conjugate vaccine manufacturing, safeguarding against impurities and unconjugated materials that could undermine vaccine performance. By employing techniques like size-exclusion chromatography, dialysis, and tangential flow filtration, manufacturers can produce vaccines that are both safe and effective, even for vulnerable populations such as infants. Rigorous quality control further ensures that these vaccines meet the highest standards, reinforcing public trust in immunization programs.
Vaccines: A Powerful Weapon Against Diseases
You may want to see also
Explore related products


![]()
Formulation & Testing: Adding adjuvants, stabilizing the vaccine, and conducting trials for safety and immunogenicity
Adjuvants are the unsung heroes of conjugate vaccines, amplifying the immune response to ensure robust protection. These substances, often aluminum salts like aluminum hydroxide or aluminum phosphate, are added in precise quantities—typically 0.1 to 1.0 mg per dose—to enhance the vaccine’s effectiveness. For instance, the Haemophilus influenzae type b (Hib) conjugate vaccine relies on aluminum hydroxide to stimulate a stronger immune reaction in infants as young as 2 months old. Adjuvants work by creating a depot effect, slowly releasing the antigen to immune cells, and triggering inflammation that mimics a natural infection. Without them, many conjugate vaccines would require higher antigen doses or additional boosters, making adjuvants a critical component of formulation.
Stabilizing a conjugate vaccine is a delicate balance of science and practicality, ensuring it remains potent from manufacturing to administration. Lyophilization, or freeze-drying, is a common method, transforming the vaccine into a dry powder that can be reconstituted with sterile water before use. This technique is particularly useful for vaccines distributed in regions with limited refrigeration, such as the meningococcal conjugate vaccine used in sub-Saharan Africa. Excipients like sucrose or lactose are added as stabilizers to protect the vaccine’s structure during drying. For liquid formulations, cold chain storage at 2–8°C is mandatory, with some vaccines requiring ultra-cold temperatures. Stability testing, conducted over months or years, verifies that the vaccine retains its efficacy under various conditions, ensuring it performs as intended in real-world scenarios.
Clinical trials are the cornerstone of proving a conjugate vaccine’s safety and immunogenicity, typically progressing through three phases. Phase I trials involve small groups of healthy adults (20–100 participants) to assess safety, dosage, and initial immune response. Phase II expands to several hundred volunteers, including target populations like children or the elderly, to evaluate immunogenicity and refine dosing. For example, the pneumococcal conjugate vaccine (PCV13) demonstrated seroconversion rates exceeding 90% in infants during Phase II. Phase III trials involve thousands of participants, comparing the vaccine to a placebo or existing vaccine to confirm efficacy and monitor rare side effects. Throughout these trials, serological assays measure antibody titers, while adverse events are meticulously documented to ensure the vaccine’s benefit outweighs any risks.
Post-licensure surveillance completes the testing cycle, monitoring the vaccine’s performance in the general population. Programs like the Vaccine Adverse Event Reporting System (VAERS) in the U.S. allow healthcare providers and patients to report side effects, enabling rapid detection of rare or long-term issues. For instance, the introduction of the rotavirus conjugate vaccine led to ongoing surveillance for intussusception, a rare bowel complication. Immunogenicity studies continue post-approval, tracking antibody persistence and the need for boosters. This comprehensive approach ensures that conjugate vaccines not only meet regulatory standards but also deliver sustained protection across diverse populations, from newborns to the immunocompromised.
Costa Rica's Vaccination Rate: Current Status and Public Health Insights
You may want to see also
Frequently asked questions
A conjugate vaccine is a type of vaccine that combines a weak antigen (such as a polysaccharide from a bacterium) with a strong antigen (a carrier protein) to enhance the immune response. Unlike traditional vaccines, conjugate vaccines improve immunity in populations like infants and the elderly, who often respond poorly to polysaccharide-only vaccines.
A conjugate vaccine is made by chemically linking a weak antigen (e.g., bacterial polysaccharide) to a carrier protein (e.g., tetanus toxoid or diphtheria toxoid). This process involves isolating and purifying both components, activating them with reagents, and then conjugating them together. The resulting conjugate is purified and formulated into a vaccine.
The key steps include: 1) isolating and purifying the polysaccharide antigen and carrier protein, 2) activating both components using chemical reagents, 3) conjugating the polysaccharide to the carrier protein, 4) purifying the conjugate to remove unreacted materials, and 5) formulating the conjugate into a stable vaccine product.
A carrier protein is necessary because it helps the immune system recognize and respond more effectively to the weak antigen (polysaccharide). The carrier protein stimulates T-cell help, leading to a stronger, longer-lasting immune response, including the production of memory cells and high-affinity antibodies.