The development of the polio vaccine stands as one of the most remarkable achievements in medical history, marked by unprecedented speed and collaboration. In the mid-20th century, polio was a devastating disease, paralyzing and killing thousands, particularly children, every year. The race to create a vaccine began in earnest in the 1950s, led by pioneering scientists like Jonas Salk and Albert Sabin. Salk’s inactivated polio vaccine (IPV) was developed in just a few years, with large-scale clinical trials involving 1.8 million children in 1954. By April 1955, the vaccine was declared safe and effective, a process that took less than a decade from initial research to widespread distribution. Sabin’s oral polio vaccine (OPV) followed in the early 1960s, further accelerating global eradication efforts. This rapid timeline was made possible by massive public and private investment, international cooperation, and a shared urgency to combat a feared disease, setting a precedent for vaccine development that continues to inspire modern medical breakthroughs.
| Characteristics | Values |
|---|---|
| Development Start | Research on polio vaccines began in the 1930s, but intensified in the 1950s. |
| Key Researcher | Jonas Salk led the development of the first successful polio vaccine. |
| Vaccine Type | Inactivated Polio Vaccine (IPV), introduced in 1955. |
| Clinical Trials | Large-scale field trials involving 1.8 million children in 1954. |
| Approval Date | April 12, 1955, by the U.S. government. |
| Timeframe | Approximately 7 years from focused development to approval (1948–1955). |
| Impact | Polio cases in the U.S. dropped from 28,985 in 1955 to 5,600 in 1957. |
| Global Eradication Efforts | Ongoing since 1988; wild polio cases reduced by over 99% globally. |
| Current Status | Polio remains endemic in only 2 countries (Afghanistan and Pakistan). |
| Vaccine Distribution | Over 2.5 billion children vaccinated worldwide since 1988. |
| Challenges | Initial Cutter Incident (1955) led to temporary vaccine distribution halt. |
| Second Vaccine | Oral Polio Vaccine (OPV) developed by Albert Sabin in 1961. |
| Cost of Development | Funded primarily by the March of Dimes, costing millions of dollars. |
| Public Health Legacy | Served as a model for rapid vaccine development (e.g., COVID-19 vaccines). |
Explore related products


$24.17 $25.99




What You'll Learn
- Pre-Vaccine Polio Outbreaks: Frequency and severity of polio outbreaks before vaccine development
- Research Timeline: Key milestones in the development of the polio vaccine
- Salk vs. Sabin: Differences between Salk’s inactivated and Sabin’s oral polio vaccines
- Clinical Trials: Speed and scale of polio vaccine clinical trials in the 1950s
- Regulatory Approval: Process and timeline for polio vaccine approval by health authorities
![]()
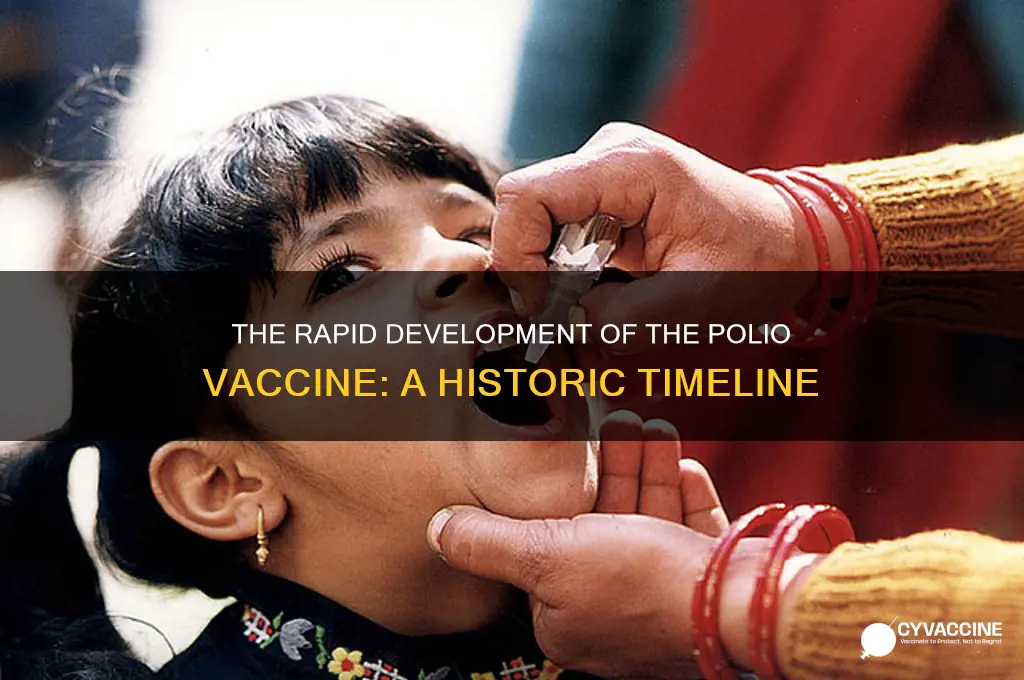
Pre-Vaccine Polio Outbreaks: Frequency and severity of polio outbreaks before vaccine development
Before the development of the polio vaccine, the world experienced frequent and devastating outbreaks of poliomyelitis, a highly contagious viral disease. Polio primarily affected young children, causing muscle weakness, paralysis, and, in severe cases, death. The disease was particularly feared due to its ability to strike suddenly and leave survivors with lifelong disabilities. Outbreaks were seasonal, often peaking during the summer months, and they could spread rapidly through communities, leaving a trail of devastation in their wake.
The frequency of polio outbreaks increased significantly in the early 20th century, coinciding with urbanization and improved sanitation, which paradoxically made the population more susceptible. In the United States, for example, polio cases rose from a few thousand annually in the early 1900s to nearly 60,000 cases in 1952, the worst year on record. Globally, the World Health Organization (WHO) estimates that before the vaccine, polio paralyzed or killed over 500,000 people annually. The severity of these outbreaks was compounded by the lack of effective treatments, leaving isolation, physical therapy, and the infamous iron lung as the primary means of managing the disease.
The impact of pre-vaccine polio outbreaks extended beyond physical health, causing widespread panic and social disruption. Schools and public swimming pools often closed during outbreaks to prevent transmission, and parents lived in constant fear of their children contracting the disease. The economic burden was also substantial, as families faced medical expenses and long-term care costs for paralyzed individuals. These factors fueled an urgent global effort to develop a vaccine, culminating in Jonas Salk's inactivated polio vaccine (IPV) in 1955, which marked the beginning of the end for polio as a major public health threat.
In countries with limited healthcare infrastructure, pre-vaccine polio outbreaks were even more devastating. Poor sanitation and overcrowded living conditions facilitated the virus's spread, and access to medical care was often inadequate. This disparity highlighted the need for a global solution, as localized efforts were insufficient to control the disease. The recurring and severe nature of these outbreaks underscored the critical importance of vaccine development, which ultimately took less than two decades of focused research to achieve, a remarkable feat in medical history.
The historical context of pre-vaccine polio outbreaks is essential for understanding the rapid development of the vaccine. The urgency created by the disease's frequency and severity mobilized governments, scientists, and the public to support research and trials. For instance, the March of Dimes, a U.S. fundraising organization, played a pivotal role in financing Salk's research. This collective effort, driven by the dire need to end the suffering caused by polio, accelerated the timeline for vaccine development, which was completed in an unprecedentedly short period compared to other vaccines. The success of the polio vaccine not only eradicated the disease in most parts of the world but also set a precedent for addressing other global health challenges.
Vaccine Ingredients: Aluminum, Mercury, and More
You may want to see also
Explore related products


$18.99 $18.99




![]()
Research Timeline: Key milestones in the development of the polio vaccine
The development of the polio vaccine was a landmark achievement in medical history, marked by significant milestones that culminated in the eradication of a devastating disease. The journey began in the early 20th century, as polio outbreaks became increasingly frequent and severe, particularly in industrialized countries. The first critical milestone came in 1908 when Karl Landsteiner and Erwin Popper identified the poliovirus as the causative agent of poliomyelitis. This discovery laid the foundation for understanding the disease and paved the way for future research. However, it wasn’t until the 1930s and 1940s that scientists began to make substantial progress in isolating and studying the virus, thanks to the work of researchers like John Enders, Thomas Weller, and Frederick Robbins. In 1949, their team successfully grew the poliovirus in non-nervous tissue cultures, a breakthrough that earned them the Nobel Prize and enabled the development of vaccines.
The 1950s marked a turning point in polio vaccine research, with two distinct approaches emerging. Jonas Salk, a virologist at the University of Pittsburgh, focused on developing an inactivated polio vaccine (IPV). After years of rigorous testing, Salk’s vaccine was declared safe and effective in 1955 following a massive field trial involving 1.8 million children. This milestone marked the first widely available polio vaccine, significantly reducing polio cases in the United States and other countries. Meanwhile, Albert Sabin, a rival researcher, worked on an oral polio vaccine (OPV) using a live but attenuated virus. Sabin’s vaccine, which was easier to administer and provided longer-lasting immunity, was licensed in the United States in 1962 after extensive trials in the Soviet Union and other countries.
The global impact of these vaccines became evident in the decades that followed. By the 1960s, widespread vaccination campaigns had drastically reduced polio cases in many parts of the world. The World Health Organization (WHO) launched the Global Polio Eradication Initiative in 1988, aiming to eliminate polio worldwide through immunization. This initiative built on the success of the vaccines developed by Salk and Sabin, combining both IPV and OPV in strategic vaccination programs. By the early 21st century, polio had been eradicated in most countries, with only a few endemic regions remaining.
From the identification of the poliovirus in 1908 to the global eradication efforts of the late 20th century, the development of the polio vaccine spanned roughly five decades. The rapid progress in the 1950s, particularly the approval of Salk’s vaccine in 1955, demonstrated the power of scientific collaboration and public health initiatives. The polio vaccine’s timeline highlights the importance of persistence, innovation, and global cooperation in tackling infectious diseases. It remains a testament to what can be achieved when research, funding, and public will align toward a common goal.
In summary, the polio vaccine’s development was a multifaceted process that involved key discoveries, technological advancements, and large-scale trials. The timeline from the virus’s identification to the creation of effective vaccines underscores the speed at which scientific breakthroughs can occur when resources and determination are focused. The legacy of the polio vaccine continues to inspire efforts to combat other infectious diseases, proving that with concerted action, even the most formidable health challenges can be overcome.
Vets and Rabies Vaccines: Breed Testing for Paperwork
You may want to see also
Explore related products






![]()
Salk vs. Sabin: Differences between Salk’s inactivated and Sabin’s oral polio vaccines
The development of polio vaccines in the mid-20th century was a landmark achievement in medical history, with Jonas Salk and Albert Sabin playing pivotal roles. Salk’s inactivated polio vaccine (IPV) and Sabin’s oral polio vaccine (OPV) emerged as the two primary tools in the fight against poliomyelitis. The speed at which these vaccines were developed is remarkable: Salk’s vaccine was introduced in 1955, just six years after he began his focused research, while Sabin’s vaccine followed in 1961. This rapid progress was driven by the urgency of the polio epidemic, which paralyzed or killed thousands annually, particularly children. The differences between these vaccines lie in their composition, administration, and immune response, each with distinct advantages and limitations.
Salk’s inactivated polio vaccine (IPV) is made from polioviruses that have been killed or inactivated using formaldehyde. This ensures the vaccine cannot cause polio, making it extremely safe. IPV is administered via injection, typically in the arm or leg, and induces a strong humoral immune response, producing antibodies in the bloodstream to neutralize the virus. However, it does not effectively stimulate mucosal immunity in the gut, where poliovirus replicates, meaning it is less effective at preventing viral shedding and transmission. IPV’s primary advantage is its safety profile, as it cannot revert to a virulent form, making it ideal for individual protection in regions with low polio prevalence.
In contrast, Sabin’s oral polio vaccine (OPV) uses live but attenuated (weakened) polioviruses. Administered orally, often on a sugar cube, OPV mimics natural infection by stimulating both humoral and mucosal immunity. This dual response not only protects against paralysis but also reduces viral shedding, curbing community transmission. However, the use of live virus carries a small risk of vaccine-associated paralytic polio (VAPP), where the attenuated virus regains virulence in rare cases. OPV’s ease of administration and its ability to confer herd immunity made it the vaccine of choice for global eradication campaigns, particularly in resource-limited settings.
The differences in manufacturing and storage further distinguish the two vaccines. IPV requires more complex production processes, including virus inactivation and purification, and must be stored under refrigeration. OPV, while simpler to produce, still requires careful handling to maintain the viability of the live attenuated virus. These logistical considerations influenced their deployment, with OPV being more practical for mass immunization campaigns in developing countries.
In summary, Salk’s IPV and Sabin’s OPV represent complementary approaches to polio prevention. IPV’s safety and injectable form make it suitable for individual protection, while OPV’s ability to induce mucosal immunity and ease of administration have been instrumental in interrupting polio transmission globally. The rapid development of these vaccines, driven by the polio epidemic’s urgency, highlights the power of scientific innovation in addressing public health crises. Together, they have brought the world to the brink of polio eradication, demonstrating the enduring impact of Salk and Sabin’s pioneering work.
Rapid Vaccine Approval: Unraveling the Science Behind the Speed
You may want to see also
Explore related products






![]()
Clinical Trials: Speed and scale of polio vaccine clinical trials in the 1950s
The development and deployment of the polio vaccine in the 1950s were marked by an unprecedented speed and scale in clinical trials, driven by the urgent need to combat a disease that had paralyzed and killed thousands annually. The process began with Jonas Salk's inactivated polio vaccine (IPV), which entered clinical trials in 1954. These trials were massive in scope, involving approximately 1.8 million children across the United States, Canada, and Finland. Known as the Francis Field Trials, named after statistician Thomas Francis Jr., they were the largest medical experiment in history at the time. The trials were designed to test the vaccine's safety and efficacy rigorously, with participants divided into vaccine and control groups. The speed at which these trials were organized and executed was remarkable, reflecting the collective determination of scientists, public health officials, and the public to eradicate polio.
The scale of the trials was not just about numbers but also about logistical complexity. Vaccines and placebos had to be distributed to thousands of locations, and meticulous records were kept to track outcomes. The trials were conducted in two phases: the first phase focused on safety, while the second phase assessed efficacy. Results were analyzed swiftly, and by April 1955, it was announced that the vaccine was safe and effective, reducing polio cases by 80-90%. This rapid timeline was made possible by the collaboration of numerous organizations, including the National Foundation for Infantile Paralysis (now the March of Dimes), which funded the research and mobilized public support. The urgency of the polio epidemic ensured that bureaucratic and administrative hurdles were minimized, allowing the trials to proceed at an accelerated pace.
Despite the speed, the trials maintained high scientific standards. Researchers ensured that the vaccine was thoroughly tested across diverse populations, including different age groups and socioeconomic backgrounds. The success of the trials was also attributed to the public's trust in the medical community and their willingness to participate. This trust was built through transparent communication about the vaccine's development and the potential risks and benefits. The rapid progression from laboratory research to large-scale trials demonstrated the power of focused scientific effort and public-private partnerships in addressing a major health crisis.
The polio vaccine trials also set a precedent for future vaccine development, particularly in terms of trial design and community engagement. The methods used in the 1950s, such as randomized controlled trials and large-scale data collection, became standard practices in clinical research. Additionally, the success of the polio vaccine inspired global efforts to eradicate other infectious diseases, such as smallpox and measles. The speed and scale of the polio vaccine trials were a testament to what could be achieved when scientific innovation, public health infrastructure, and societal commitment aligned toward a common goal.
In conclusion, the clinical trials of the polio vaccine in the 1950s were a landmark achievement in medical history, characterized by their rapid execution and immense scale. The trials not only demonstrated the vaccine's efficacy but also established a model for future vaccine development and public health initiatives. The collaboration between scientists, governments, and the public played a crucial role in overcoming the challenges of such an ambitious endeavor. The polio vaccine's swift development and deployment remain a powerful example of how humanity can unite to combat devastating diseases.
MMR Vaccine: Protection Against Measles, Mumps, and Rubella
You may want to see also
Explore related products






![]()
Regulatory Approval: Process and timeline for polio vaccine approval by health authorities
The development and regulatory approval of the polio vaccine is a landmark achievement in medical history, marked by unprecedented speed and collaboration. The process began in the 1950s, driven by the urgent need to combat a disease that paralyzed or killed thousands annually. Jonas Salk led the effort to create the first inactivated polio vaccine (IPV), which required rigorous testing and regulatory scrutiny to ensure safety and efficacy. The regulatory approval process for the polio vaccine was streamlined but thorough, involving multiple phases of clinical trials and close collaboration with health authorities, particularly the U.S. Food and Drug Administration (FDA).
The timeline for regulatory approval began with preclinical testing and small-scale human trials in the early 1950s. By 1954, the vaccine entered large-scale field trials involving 1.8 million children, known as the Francis Field Trials. These trials were pivotal in demonstrating the vaccine's effectiveness and safety. Following the successful completion of these trials, Salk and his team submitted their findings to the FDA for review. The FDA expedited its evaluation process, recognizing the public health emergency posed by polio. In April 1955, the FDA granted approval for the widespread distribution of the polio vaccine, just a few years after the initial trials began.
The regulatory process for the polio vaccine was characterized by a balance between speed and caution. Health authorities prioritized rapid approval but did not compromise on the need for robust evidence of safety and efficacy. This was achieved through continuous monitoring during the trials and a transparent review process. The collaboration between researchers, pharmaceutical companies, and regulatory bodies was unprecedented, setting a precedent for future vaccine development efforts, such as those seen during the COVID-19 pandemic.
Following FDA approval, the polio vaccine was quickly rolled out across the United States and later globally. However, the process was not without challenges. In 1955, the "Cutter Incident," where a manufacturing defect led to some vaccine batches causing polio cases, highlighted the importance of stringent quality control. This event led to further regulatory measures to ensure vaccine safety, including stricter oversight of manufacturing processes. Despite this setback, the vaccine's overall success in reducing polio cases was undeniable.
Globally, regulatory approval processes varied but followed similar principles of safety and efficacy. The World Health Organization (WHO) played a crucial role in standardizing vaccine requirements and supporting distribution in developing countries. By the late 1950s and early 1960s, the polio vaccine had gained approval in numerous countries, leading to a dramatic decline in polio cases worldwide. The entire process, from initial development to widespread approval, took less than a decade, a remarkable feat that showcased the potential of focused scientific and regulatory collaboration.
In summary, the regulatory approval of the polio vaccine was a testament to the ability of health authorities to act swiftly while maintaining high standards of safety and efficacy. The process involved rigorous clinical trials, expedited FDA review, and global coordination. Lessons from this timeline continue to inform vaccine development and approval processes today, emphasizing the importance of collaboration, transparency, and public health priorities. The polio vaccine's rapid approval not only saved millions of lives but also set a benchmark for addressing future health crises.
Hepatitis B Post-Vaccination: Understanding Risks and Long-Term Protection
You may want to see also
Frequently asked questions
The first polio vaccine, developed by Jonas Salk, took approximately 7 years to go from initial research to widespread distribution, with the vaccine being declared safe and effective in 1955.
The polio vaccine became available to the public in 1955, following successful large-scale trials involving over 1.8 million children.
The rollout of the polio vaccine varied globally, but it began in earnest in the late 1950s and early 1960s, with widespread adoption in developed countries and gradual introduction in developing nations.
The rapid development of the polio vaccine was driven by significant public fear of the disease, substantial funding from organizations like the March of Dimes, and the focused efforts of researchers like Jonas Salk and later Albert Sabin.
The oral polio vaccine (OPV), developed by Albert Sabin, was introduced in 1961, just 6 years after the inactivated polio vaccine (IPV). Its development was faster due to building on Salk's groundwork and advancements in virology.