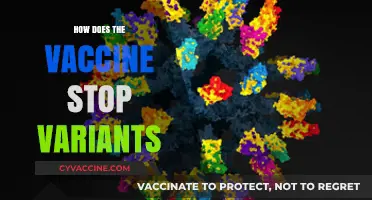
Vaccine-derived poliovirus (VDPV) is a rare but significant phenomenon that occurs when the weakened poliovirus contained in the oral polio vaccine (OPV) mutates and regains its ability to cause paralysis after circulating in underimmunized populations. Unlike wild poliovirus, which is naturally occurring, VDPVs emerge from the live, attenuated virus in OPV, particularly in areas with low vaccination coverage where the virus can spread and evolve over time. This can lead to outbreaks of polio, posing a challenge to global eradication efforts. Understanding how VDPVs spread is crucial, as it highlights the importance of maintaining high vaccination rates and transitioning to inactivated polio vaccine (IPV) in regions where OPV use is phased out.
| Characteristics | Values |
|---|---|
| Mode of Spread | Fecal-oral transmission |
| Source of Virus | Shedding of attenuated vaccine virus (Sabin strains) from vaccinated individuals |
| Vaccine Type Involved | Oral Polio Vaccine (OPV), specifically types 1, 2, or 3 Sabin strains |
| Circulation Risk | Occurs in under-immunized populations with low vaccination coverage |
| Mutation Potential | Vaccine virus can revert to a neurovirulent form after prolonged circulation |
| Duration of Shedding | Vaccinated individuals can shed the virus for 6–8 weeks post-vaccination |
| Environmental Factors | Poor sanitation and hygiene facilitate spread |
| Geographic Prevalence | Common in regions with low OPV coverage or weak immunization programs |
| Clinical Presentation | Can cause paralysis in rare cases, similar to wild poliovirus infection |
| Prevention Measures | Switching to Inactivated Polio Vaccine (IPV) and strengthening OPV campaigns |
| Global Cases (Latest Data) | As of 2023, over 500 cases reported in 20+ countries (WHO data) |
| Genetic Changes | Accumulation of 10–20 nucleotide reversions leads to virulence |
| Public Health Impact | Threatens polio eradication efforts due to vaccine-derived outbreaks |
| Surveillance Methods | Environmental and acute flaccid paralysis (AFP) surveillance |
| Eradication Strategy | Global OPV cessation and IPV integration in routine immunization |
Explore related products






What You'll Learn
- Vaccine Strain Mutation: How oral polio vaccine (OPV) strains can mutate into circulating vaccine-derived polioviruses (cVDPV)
- Immune Deficiency Role: Spread in individuals with weakened immune systems shedding vaccine-derived virus for years
- Underimmunized Populations: How low vaccination rates allow vaccine-derived strains to circulate and cause outbreaks
- Sanitation and Transmission: Poor sanitation facilitates the spread of vaccine-derived polioviruses in communities
- Global Surveillance Efforts: Monitoring and containment strategies to detect and stop cVDPV transmission
![]()
Vaccine Strain Mutation: How oral polio vaccine (OPV) strains can mutate into circulating vaccine-derived polioviruses (cVDPV)
Oral polio vaccine (OPV) contains live, attenuated (weakened) polioviruses designed to trigger immunity without causing disease. However, in rare cases, these vaccine strains can revert to a more virulent form through genetic mutation, particularly in underimmunized populations. This process, known as vaccine-derived poliovirus (VDPV) emergence, occurs when the vaccine virus circulates long enough in a community with low vaccination coverage, accumulating mutations that restore its neurovirulence. Circulating vaccine-derived polioviruses (cVDPVs) are the most concerning type of VDPV, as they can spread from person to person, causing paralysis in susceptible individuals.
The risk of cVDPV emergence is directly tied to the duration and extent of vaccine virus circulation. In areas with inadequate sanitation and low OPV coverage, the vaccine virus can be shed in stool and transmitted through fecal-oral routes, persisting in the environment for weeks. Each time the virus replicates, it has a chance to mutate. Key mutations often occur in the viral capsid proteins, particularly the VP1 region, which can restore the virus’s ability to evade the immune system and cause disease. For instance, a single nucleotide change can alter the virus’s antigenic properties, making it indistinguishable from wild poliovirus in terms of pathogenicity.
Preventing cVDPV emergence requires a two-pronged strategy: maintaining high OPV coverage to limit virus circulation and transitioning to inactivated polio vaccine (IPV) in regions where wild poliovirus has been eradicated. The Global Polio Eradication Initiative recommends administering at least 3 doses of OPV to children under 5 years old, with supplementary immunization campaigns in high-risk areas. However, as wild poliovirus nears eradication, the risk-benefit balance of OPV shifts, prompting the phased removal of type 2 OPV (which accounts for 90% of cVDPV cases) in 2016. This strategy, known as the "polio endgame," aims to eliminate both wild and vaccine-derived polioviruses.
Despite these efforts, cVDPV outbreaks continue to occur, particularly in regions with conflict, poor healthcare infrastructure, or vaccine hesitancy. For example, in 2020, cVDPV2 outbreaks were reported in 20 countries across Africa, Asia, and Europe, highlighting the challenges of achieving uniform vaccination coverage. Surveillance is critical to detect and respond to cVDPVs early. Stool samples from acute flaccid paralysis (AFP) cases are tested for poliovirus, and genetic sequencing is used to distinguish between wild, vaccine, and vaccine-derived strains. Rapid outbreak response, including targeted vaccination campaigns, can halt transmission and prevent further spread.
In conclusion, while OPV has been instrumental in reducing polio cases by 99% since 1988, its use carries a small but significant risk of cVDPV emergence. Understanding the mechanisms of vaccine strain mutation underscores the importance of sustained vaccination efforts, robust surveillance, and strategic vaccine transitions. As the world edges closer to polio eradication, addressing cVDPVs remains a critical priority to ensure a polio-free future.
Rabies Vaccine for Cattle: Availability, Benefits, and Importance Explained
You may want to see also
Explore related products






![]()
Immune Deficiency Role: Spread in individuals with weakened immune systems shedding vaccine-derived virus for years
Vaccine-derived polioviruses (VDPVs) emerge when the attenuated (weakened) virus in the oral polio vaccine (OPV) mutates in environments with low vaccination coverage. While rare, a critical yet under-discussed pathway for their spread involves individuals with weakened immune systems. These immunocompromised individuals, such as those with primary immunodeficiencies, HIV/AIDS, or undergoing immunosuppressive therapies, can shed the vaccine-derived virus for extended periods—sometimes years—posing a risk to unvaccinated populations. This phenomenon highlights a paradox: the very tool designed to eradicate polio can, in specific cases, contribute to its persistence.
Consider the case of a 28-year-old patient with agammaglobulinemia, a primary immunodeficiency disorder, who received OPV as a child. Despite the vaccine’s attenuated nature, their compromised immune system failed to clear the virus. Over seven years, they intermittently shed the mutated virus in their stool, unknowingly becoming a source of transmission in their community. This scenario underscores the importance of identifying and managing immunocompromised individuals in polio eradication efforts. For instance, the World Health Organization (WHO) recommends that such individuals avoid OPV and instead receive the inactivated polio vaccine (IPV), which contains no live virus and cannot revert to a virulent form.
The risk of prolonged shedding is not uniform across all immunocompromised groups. Children under five with severe combined immunodeficiency (SCID) are particularly vulnerable, as their immune systems are incapable of mounting an effective response to the vaccine virus. Studies show that these individuals can shed VDPVs for up to 10 years, with viral loads comparable to those of wild poliovirus infections. To mitigate this, healthcare providers should screen for immunodeficiencies before administering OPV, especially in regions transitioning from OPV to IPV. For those already exposed, antiviral therapies and close monitoring of stool samples can help limit viral spread.
Persuasively, the argument for transitioning entirely to IPV gains strength when considering the immunocompromised population. While OPV’s ease of administration and gut immunity benefits have made it a cornerstone of polio eradication, its risks in vulnerable individuals cannot be ignored. Countries like the United States and the United Kingdom have long relied on IPV, eliminating the risk of VDPVs altogether. For low-income regions, where OPV remains prevalent, targeted IPV campaigns for immunocompromised individuals could serve as a practical interim solution. This dual approach balances the need for herd immunity with the protection of those most at risk.
In conclusion, the role of immunocompromised individuals in the spread of vaccine-derived polio is a critical yet often overlooked aspect of eradication efforts. By understanding the mechanisms of prolonged shedding, implementing targeted vaccination strategies, and prioritizing IPV for vulnerable populations, public health systems can address this hidden pathway of transmission. The goal remains clear: to eliminate polio without inadvertently enabling its persistence in those least equipped to fight it.
Understanding the Coronavirus Vaccine: Types, Technology, and Effectiveness Explained
You may want to see also
Explore related products




![]()
Underimmunized Populations: How low vaccination rates allow vaccine-derived strains to circulate and cause outbreaks
In regions with underimmunized populations, the oral polio vaccine (OPV) can paradoxically become a source of outbreaks. OPV contains weakened live viruses that, in rare cases, can mutate and regain virulence as they circulate in communities with low vaccination coverage. This phenomenon, known as vaccine-derived poliovirus (VDPV), highlights the delicate balance between immunization and vulnerability. When a critical mass of individuals remains unvaccinated, the mutated virus finds fertile ground to spread, causing paralysis in the same manner as wild poliovirus. This underscores the importance of achieving and maintaining high vaccination rates to prevent such reversals in polio eradication efforts.
Consider the mechanics of VDPV transmission: in fully vaccinated populations, the mutated virus is quickly contained, as the majority have immunity. However, in areas where vaccination rates dip below 80%, the virus can silently circulate, evolving over months or years. Children under 5 are particularly at risk, as they require multiple OPV doses (typically 3–4) to build robust immunity. In underimmunized communities, even a single missed dose can leave gaps in protection, allowing the virus to persist and mutate. This is why outbreaks often emerge in hard-to-reach or conflict-affected areas, where healthcare access is limited and vaccination campaigns face logistical challenges.
A comparative analysis of recent outbreaks reveals a clear pattern. In 2020, vaccine-derived polio cases were reported in 22 countries, primarily in Africa and Asia, where vaccination rates had stagnated or declined. For instance, in northern Nigeria, a region with historically low OPV coverage due to vaccine hesitancy and insecurity, VDPV caused over 100 cases of paralysis. In contrast, countries like India, which achieved near-universal vaccination coverage, have successfully prevented such outbreaks. This disparity illustrates how underimmunization not only leaves individuals unprotected but also creates reservoirs for VDPV to emerge and spread.
To mitigate this risk, public health strategies must focus on closing immunity gaps. This includes targeted vaccination drives in underserved areas, addressing misinformation through community engagement, and strengthening surveillance systems to detect VDPV early. For parents in at-risk regions, ensuring children receive all recommended OPV doses is critical. Additionally, transitioning from OPV to the inactivated polio vaccine (IPV) in routine immunization programs can reduce the risk of VDPV, though this requires robust cold chain infrastructure and higher costs. Ultimately, the lesson is clear: underimmunization is not just a local problem—it threatens global polio eradication efforts by allowing vaccine-derived strains to circulate and cause harm.
Are Inactivated Vaccines Recombinant? Understanding Vaccine Types and Differences
You may want to see also
Explore related products






![]()
Sanitation and Transmission: Poor sanitation facilitates the spread of vaccine-derived polioviruses in communities
Poor sanitation serves as a critical conduit for the spread of vaccine-derived polioviruses (VDPVs), particularly in communities where access to clean water and proper waste management is limited. When oral polio vaccine (OPV) is administered, it contains weakened strains of the virus that replicate in the intestinal tract. These attenuated viruses are excreted in feces for several weeks after vaccination. In areas with inadequate sanitation, contaminated fecal matter can easily enter the water supply or environment, exposing unvaccinated or immunocompromised individuals to the vaccine-derived virus. Over time, as the virus circulates in underimmunized populations, it can mutate and regain neurovirulence, transforming into VDPVs capable of causing paralysis.
Consider the mechanics of transmission: a single dose of OPV sheds enough virus to contaminate water sources if sanitation systems fail. In communities where open defecation is common or sewage treatment is nonexistent, the risk escalates dramatically. For instance, studies in regions like northern Nigeria and the Democratic Republic of Congo have shown that VDPV outbreaks often correlate with areas where less than 50% of households have access to improved sanitation facilities. Children under five, who are both primary recipients of OPV and highly susceptible to environmental contamination, become unwitting vectors, perpetuating the cycle of transmission.
To mitigate this risk, targeted interventions must address sanitation gaps in high-risk areas. Practical steps include constructing latrines, implementing wastewater treatment systems, and promoting handwashing with soap after contact with fecal material. For example, in India’s polio eradication campaign, the integration of sanitation improvements alongside vaccination drives reduced environmental poliovirus detection by 70% within two years. Similarly, in conflict-affected regions where sanitation infrastructure is often destroyed, distributing portable water filters and chlorine tablets can serve as temporary but effective stopgaps.
However, improving sanitation alone is insufficient without concurrent efforts to boost vaccination coverage. The World Health Organization recommends maintaining OPV coverage above 90% in at-risk populations to minimize the likelihood of VDPV emergence. Yet, in areas where vaccine hesitancy or logistical challenges persist, even minor sanitation lapses can undermine progress. A comparative analysis of VDPV outbreaks in Syria and Somalia revealed that communities with vaccination rates below 80% and poor sanitation experienced outbreak durations twice as long as those with better hygiene practices.
Ultimately, breaking the link between poor sanitation and VDPV transmission requires a dual strategy: strengthening immunization programs while systematically upgrading sanitation infrastructure. This approach not only curtails the spread of vaccine-derived polioviruses but also addresses broader public health threats associated with contaminated environments. By treating sanitation as a cornerstone of disease prevention, communities can move closer to the global goal of polio eradication, ensuring that the very tools designed to protect us do not inadvertently become sources of harm.
Pneumonia Vaccine Frequency: Essential Timing for Optimal Protection
You may want to see also
Explore related products






![]()
Global Surveillance Efforts: Monitoring and containment strategies to detect and stop cVDPV transmission
Vaccine-derived polioviruses (cVDPVs) emerge when the attenuated virus in the oral polio vaccine (OPV) mutates and regains neurovirulence, posing a risk to under-immunized populations. Detecting and containing these outbreaks requires a robust global surveillance system, which operates through a multi-pronged approach. Environmental surveillance, for instance, involves collecting sewage samples from high-risk areas to detect the presence of polioviruses before clinical cases appear. This early warning system is critical in regions with low vaccination coverage, where cVDPVs can silently circulate. By analyzing these samples, public health officials can pinpoint transmission hotspots and deploy targeted interventions.
Once a cVDPV is detected, rapid response teams are mobilized to conduct outbreak investigations. These teams assess vaccination coverage, identify gaps in immunity, and implement containment strategies. One key tactic is conducting reactive vaccination campaigns using OPV or inactivated polio vaccine (IPV), depending on the local context. For example, in areas with low IPV coverage, a rapid round of OPV may be administered to children under 5 years old, ensuring at least 95% coverage to interrupt transmission. However, the use of OPV must be carefully managed, as it can itself seed new cVDPVs if not phased out appropriately.
Containment strategies extend beyond vaccination to include improving routine immunization services and strengthening health systems. This involves training healthcare workers to administer vaccines correctly, ensuring cold chain integrity, and educating communities about the importance of completing the full vaccine series. In settings where vaccine hesitancy is a barrier, tailored communication strategies are employed to address misconceptions and build trust. For instance, in some regions, local leaders and religious figures are engaged to endorse vaccination campaigns, increasing acceptance rates.
Global coordination is another cornerstone of surveillance efforts. The Global Polio Eradication Initiative (GPEI) facilitates information sharing, resource allocation, and technical support across countries. Through its Environmental Surveillance (ES) network, over 40 countries regularly test sewage samples, contributing to a global database that tracks poliovirus circulation. This data-driven approach allows for real-time monitoring and rapid response, minimizing the risk of cVDPV spread across borders. For example, when a cVDPV strain was detected in Malawi in 2021, GPEI’s rapid response mechanisms helped contain the outbreak before it could spread regionally.
Despite these efforts, challenges remain. Limited funding, political instability, and logistical hurdles in remote areas can hinder surveillance and response activities. To address these gaps, innovative tools like digital surveillance platforms and geospatial mapping are being integrated into monitoring systems. These technologies enable more precise tracking of vaccination campaigns and outbreak responses, ensuring resources are allocated efficiently. Ultimately, the success of global surveillance efforts hinges on sustained commitment, collaboration, and adaptability to emerging threats. By combining scientific rigor with community engagement, the world can move closer to eradicating all forms of polio, including cVDPVs.
Nevada Vaccine Lottery: Step-by-Step Guide to Register and Win
You may want to see also
Frequently asked questions
Vaccine-derived polio spreads when the weakened virus in the oral polio vaccine (OPV) mutates and circulates in underimmunized populations, causing rare cases of paralysis similar to wild poliovirus.
Yes, vaccine-derived polio can spread from person to person, especially in areas with low vaccination coverage, as the mutated virus is shed in stool and can infect others.
Individuals living in areas with poor sanitation, inadequate vaccination coverage, and limited access to healthcare are at higher risk of contracting vaccine-derived polio.
Vaccine-derived polio can be prevented by maintaining high vaccination coverage with OPV or transitioning to the inactivated polio vaccine (IPV), improving sanitation, and strengthening surveillance systems.