Meningococcal disease is a serious bacterial infection caused by the bacterium *Neisseria meningitidis*, which can lead to meningitis (inflammation of the brain and spinal cord membranes) and sepsis (blood infection). To combat this potentially life-threatening illness, meningococcal vaccines have been developed to protect individuals from specific strains of the bacteria. These vaccines work by stimulating the immune system to produce antibodies against the meningococcal bacteria, primarily targeting the polysaccharide capsule that surrounds the bacterium. The vaccine is available in different forms, including conjugate vaccines (which are more effective and provide longer-lasting immunity) and polysaccharide vaccines. Conjugate vaccines, such as MenACWY and MenB, are commonly used and recommended for adolescents, college students, and individuals at higher risk, offering protection against multiple serogroups of the bacteria. Understanding how meningococcal vaccines are formulated and administered is crucial for preventing outbreaks and safeguarding public health.
Explore related products






What You'll Learn
- Vaccine Types: Conjugate, polysaccharide, and protein-based vaccines target different meningococcal strains effectively
- Development Process: Research, clinical trials, and approval ensure vaccine safety and efficacy
- Administration Methods: Injections, doses, and schedules vary by age and risk factors
- Immune Response: Vaccines stimulate antibodies to protect against meningococcal bacteria
- Global Distribution: Accessibility, affordability, and campaigns impact vaccine reach worldwide
![]()
Vaccine Types: Conjugate, polysaccharide, and protein-based vaccines target different meningococcal strains effectively
Meningococcal vaccines are tailored to combat specific strains of *Neisseria meningitidis*, the bacterium responsible for meningococcal disease. Among the most effective vaccine types are conjugate, polysaccharide, and protein-based formulations, each designed to target distinct strains and elicit robust immune responses. Understanding their differences is crucial for informed vaccination decisions, especially for at-risk populations such as infants, adolescents, and travelers to endemic regions.
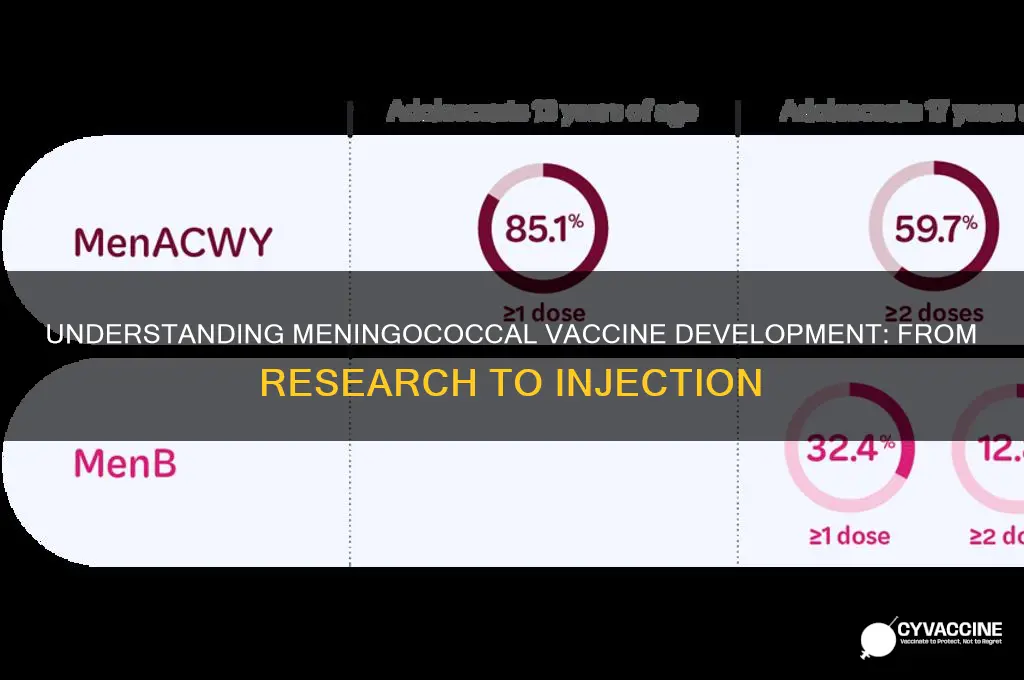
Conjugate vaccines, such as Menactra and Menveo, are the gold standard for long-term protection against meningococcal disease. These vaccines link a sugar molecule (polysaccharide) from the bacterial capsule to a carrier protein, enhancing the immune system’s ability to recognize and remember the pathogen. This process, known as conjugation, significantly improves vaccine efficacy in infants and young children, whose immune systems are less responsive to plain polysaccharide vaccines. For instance, the MenACWY conjugate vaccine is recommended for adolescents at 11–12 years of age, with a booster dose at 16 years, offering protection against serogroups A, C, W, and Y. A single dose provides over 85% efficacy, with immunity lasting up to 5 years or more.
In contrast, polysaccharide vaccines, like MPSV4, are less commonly used today due to their limitations. These vaccines contain purified polysaccharides from the bacterial capsule but lack a carrier protein, making them ineffective in children under 2 years old. Their immune response is also shorter-lived, typically requiring more frequent boosters. However, they remain an option for adults over 55 or those with specific medical conditions who cannot receive conjugate vaccines. A dose of MPSV4 provides immediate but temporary protection, with efficacy waning after 3–5 years.
Protein-based vaccines, such as Bexsero and Trumenba, represent a newer approach targeting serogroup B, which is not covered by conjugate or polysaccharide vaccines. These vaccines contain proteins extracted from the bacterial surface, such as factor H binding protein (fHbp) or Neisserial adhesin A (NadA). Bexsero, for example, is approved for individuals aged 10 weeks to 25 years and requires a 2- or 3-dose series depending on age. While protein-based vaccines offer broader strain coverage, their efficacy varies, and they are often used in outbreak settings or for high-risk groups.
When choosing a meningococcal vaccine, consider age, health status, and regional disease prevalence. Conjugate vaccines are ideal for routine immunization in adolescents and young adults, while protein-based vaccines address the gap in serogroup B protection. Polysaccharide vaccines serve as a fallback option for specific populations. Always follow healthcare provider recommendations, as dosing schedules and booster requirements differ by vaccine type. For travelers to regions like the meningitis belt in Africa, a conjugate vaccine is essential, while college students living in dormitories may benefit from serogroup B coverage. By understanding these vaccine types, individuals can make informed decisions to safeguard against this potentially deadly disease.
Unvaccinated in Portland: Exploring Oregon's Vaccine Hesitancy Trends
You may want to see also
Explore related products






![]()
Development Process: Research, clinical trials, and approval ensure vaccine safety and efficacy
The development of a meningococcal vaccine begins with rigorous research to identify the specific strains of *Neisseria meningitidis* responsible for most cases of meningitis and septicemia. Scientists analyze global epidemiological data to determine which serogroups (A, B, C, W, Y, and X) are prevalent in different regions. For instance, serogroup A is common in the African meningitis belt, while B and C are more prevalent in North America and Europe. This targeted approach ensures the vaccine is effective against the most threatening strains. Once potential antigens are identified, researchers experiment with various formulations, such as conjugate vaccines (e.g., Menactra, Menveo) that link bacterial polysaccharides to carrier proteins, enhancing immune response, especially in infants and young children.
Clinical trials are the backbone of vaccine development, ensuring both safety and efficacy before public use. Phase 1 trials involve small groups of healthy adults to assess dosage, immunogenicity, and side effects. For meningococcal vaccines, common side effects include soreness at the injection site, mild fever, and fatigue. Phase 2 expands to include children and adolescents, as meningococcal disease disproportionately affects these age groups. Dosage adjustments are critical here; for example, the MenB vaccine Bexsero is administered as a two-dose series for infants, with a minimum interval of one month between doses. Phase 3 trials involve thousands of participants to confirm efficacy and monitor rare adverse events. These trials often compare the vaccine to a placebo or an existing vaccine, providing robust data for regulatory review.
Regulatory approval is the final hurdle before a vaccine reaches the market. In the United States, the FDA scrutinizes trial data to ensure the vaccine meets stringent safety and efficacy standards. Similarly, the WHO prequalifies vaccines for global use, particularly in low-income countries. Post-approval, pharmacovigilance programs like the Vaccine Adverse Event Reporting System (VAERS) monitor real-world safety, identifying rare side effects that may not have appeared in trials. For meningococcal vaccines, this includes tracking cases of Guillain-Barré syndrome, though such events are extremely rare. Approval also involves specifying age indications; for instance, Menactra is approved for individuals aged 9 months to 55 years, while Bexsero targets those aged 10 weeks and older.
Practical implementation of meningococcal vaccines requires adherence to recommended schedules and booster guidelines. Adolescents in the U.S. are advised to receive a MenACWY vaccine at age 11–12, with a booster at 16. For those at higher risk, such as college students living in dormitories, a booster dose may be recommended. Travelers to high-risk areas, like the African meningitis belt, should ensure they are vaccinated at least two weeks before departure. Storage and handling are also critical; most meningococcal vaccines require refrigeration at 2–8°C, and healthcare providers must follow strict protocols to maintain vaccine potency. By following these guidelines, individuals and communities can maximize protection against this potentially deadly disease.
Corporate Vaccine Profits: Unveiling Big Pharma's Lucrative Immunization Business
You may want to see also
Explore related products

![]()
Administration Methods: Injections, doses, and schedules vary by age and risk factors
The meningococcal vaccine is administered through intramuscular injection, typically in the upper arm or thigh, depending on the recipient’s age. For infants and young children, the anterolateral thigh is the preferred site, while adolescents and adults receive the vaccine in the deltoid muscle. This method ensures optimal absorption and minimizes discomfort. The number of doses and the schedule, however, are not one-size-fits-all. They are tailored based on age, risk factors, and the specific vaccine type (e.g., MenACWY or MenB). For instance, adolescents aged 11–12 years are recommended to receive a single dose of MenACWY, followed by a booster at age 16. In contrast, high-risk individuals, such as those with complement deficiencies or asplenia, may require additional doses or earlier vaccination.
Consider the MenB vaccine, which is often recommended for younger age groups or those at increased risk. Infants typically receive a series of two or three doses starting at 2 months of age, with intervals of 1–2 months between doses. Adolescents and young adults may receive a two-dose series, with the second dose administered 1–6 months after the first. This variability underscores the importance of consulting healthcare providers to determine the appropriate schedule. For travelers to regions with high meningococcal prevalence, such as the meningitis belt in sub-Saharan Africa, vaccination should be completed at least 1–2 weeks before departure to ensure immunity.
High-risk populations, including college students living in dormitories, military recruits, and individuals with HIV, often face accelerated or modified schedules. For example, college freshmen living in residence halls are strongly encouraged to receive the MenB vaccine, even if they have previously completed the MenACWY series. Similarly, laboratory workers handling *Neisseria meningitidis* require a tailored vaccination plan to mitigate occupational exposure. These adjustments highlight the vaccine’s adaptability to diverse risk profiles, ensuring maximum protection where it’s needed most.
Practical tips can enhance the vaccination experience. For children, distraction techniques like singing or using toys can reduce anxiety during the injection. Adolescents and adults should avoid strenuous activity with the vaccinated arm for 24–48 hours to minimize soreness. It’s also crucial to monitor for rare side effects, such as fever or allergic reactions, and report them promptly to a healthcare provider. By understanding the nuances of administration methods, doses, and schedules, individuals can navigate the vaccination process with confidence, ensuring timely and effective protection against meningococcal disease.
Nevada Vaccine Lottery: Step-by-Step Guide to Register and Win
You may want to see also
![]()
Immune Response: Vaccines stimulate antibodies to protect against meningococcal bacteria
Meningococcal vaccines are designed to trigger a robust immune response, specifically by stimulating the production of antibodies that target the bacteria's outer capsule. This capsule, composed of polysaccharides or proteins depending on the vaccine type, is a key virulence factor that allows *Neisseria meningitidis* to evade the immune system. Conjugate vaccines, such as MenACWY, link these polysaccharides to carrier proteins, enhancing their immunogenicity, especially in infants and young children whose immune systems are less responsive to plain polysaccharide vaccines. This conjugation process is critical for eliciting a T-cell dependent response, leading to immunological memory and long-term protection.
The immune response to meningococcal vaccines begins with antigen presentation. When the vaccine is administered, typically as a 0.5 mL intramuscular injection for adolescents and adults, antigen-presenting cells (APCs) engulf the vaccine components and display them to T cells. In conjugate vaccines, the carrier protein activates T helper cells, which then stimulate B cells to produce high-affinity antibodies. These antibodies circulate in the bloodstream, ready to neutralize the bacteria by preventing their attachment to host cells or by marking them for destruction by phagocytic cells. This process is particularly effective in preventing invasive meningococcal disease, which can progress rapidly to sepsis or meningitis within hours of symptom onset.
A notable advantage of conjugate vaccines is their ability to induce herd immunity. By reducing nasopharyngeal carriage of *N. meningitidis*, vaccinated individuals are less likely to transmit the bacteria to others. For example, the MenACWY vaccine, recommended for adolescents at 11–12 years with a booster at 16, not only protects the recipient but also decreases the prevalence of the bacteria in the community. This dual benefit underscores the importance of adhering to vaccination schedules, which often include a primary dose followed by a booster to maintain protective antibody levels.
Practical considerations for maximizing immune response include proper vaccine storage and administration. Meningococcal vaccines must be refrigerated at 2°C to 8°C to preserve their efficacy, and healthcare providers should avoid freezing or exposing them to direct sunlight. For individuals with compromised immune systems, such as those with complement deficiencies or asplenia, additional doses or alternative vaccine types may be necessary to achieve adequate protection. Parents and caregivers should also be aware of potential side effects, such as mild fever or soreness at the injection site, which are typically transient and outweighed by the vaccine’s benefits.
In summary, meningococcal vaccines harness the immune system’s ability to produce targeted antibodies, offering both individual and community-level protection. Understanding the mechanisms behind this response—from antigen presentation to herd immunity—highlights the importance of vaccination in preventing a potentially devastating disease. By following recommended schedules and ensuring proper vaccine handling, individuals can maximize their defense against *N. meningitidis* and contribute to broader public health goals.
Kim Kardashian's Kids: Vaccinated or Not? The Truth Revealed
You may want to see also
![]()
Global Distribution: Accessibility, affordability, and campaigns impact vaccine reach worldwide
The global distribution of meningococcal vaccines is a complex interplay of accessibility, affordability, and the impact of public health campaigns. While high-income countries often have robust vaccination programs, low- and middle-income countries (LMICs) face significant barriers. For instance, the meningococcal conjugate vaccine (MenAfriVac), developed specifically for Africa’s meningitis belt, costs as little as $0.50 per dose due to partnerships like Gavi, the Vaccine Alliance. This affordability has enabled mass vaccination campaigns, reducing meningitis A cases by 99% in targeted regions. However, such success stories are exceptions, not the rule. Many LMICs still struggle to secure consistent vaccine supplies, highlighting the need for global equity in vaccine distribution.
Accessibility is another critical factor. In remote or conflict-affected areas, logistical challenges such as cold chain requirements and transportation infrastructure limit vaccine reach. For example, the meningococcal serogroup A vaccine requires storage between 2°C and 8°C, a challenge in regions with unreliable electricity. Innovative solutions, like solar-powered refrigerators, have been piloted but remain underutilized. Additionally, vaccine hesitancy and lack of awareness can hinder uptake even when vaccines are available. Public health campaigns, such as those in Brazil and the UK, have successfully increased vaccination rates by targeting specific age groups—adolescents and young adults, who are at higher risk of meningococcal disease.
Affordability remains a persistent barrier, particularly for newer vaccines like MenB (Bexsero and Trumenba). In the U.S., a full MenB series can cost over $300, placing it out of reach for uninsured individuals. Even in countries with universal healthcare, MenB vaccines are often not included in national immunization schedules due to cost-effectiveness debates. This disparity underscores the need for tiered pricing models and international funding mechanisms to ensure LMICs can access these vaccines. For instance, Gavi’s support has enabled over 350 million people in Africa to receive MenAfriVac, demonstrating the power of global collaboration.
Campaigns play a pivotal role in shaping vaccine reach. In Saudi Arabia, annual meningococcal vaccination is mandatory for Hajj pilgrims, preventing outbreaks in crowded settings. Similarly, the UK’s introduction of the MenACWY vaccine for teenagers in 2015, following a rise in MenW cases, led to a 70% decline in infections within two years. These examples illustrate how targeted campaigns, combined with political will and funding, can dramatically improve vaccine coverage. However, sustained efforts are required to maintain high vaccination rates and address emerging serogroups, such as MenX in Africa.
To maximize global vaccine reach, a multi-pronged approach is essential. First, LMICs must be supported through funding, technology transfer, and capacity building to manufacture vaccines locally. Second, innovative delivery systems, such as drone technology for remote areas, should be scaled up. Third, public health campaigns must be culturally tailored and evidence-based, addressing misinformation and building trust. Finally, global health organizations and governments must prioritize meningococcal vaccination as part of broader efforts to achieve health equity. Without these steps, the promise of meningococcal vaccines will remain out of reach for millions worldwide.
The Infamous Doctor Behind the Falsified Autism-Vaccine Study
You may want to see also
Frequently asked questions
The meningococcal vaccine is a preventive measure against meningococcal disease caused by the bacterium *Neisseria meningitidis*. It appears in vaccine form as a sterile liquid, typically in a single-dose vial or pre-filled syringe, ready for injection.
The meningococcal vaccine is formulated to target specific serogroups (e.g., A, B, C, W, Y) of *Neisseria meningitidis*. It contains either polysaccharides, conjugated polysaccharides, or recombinant proteins that stimulate the immune system to produce antibodies against the bacteria.
There are two main types: conjugate vaccines (e.g., MenACWY) and recombinant protein vaccines (e.g., MenB). Conjugate vaccines combine polysaccharides with a protein carrier, while MenB vaccines use recombinant proteins. Both are liquid formulations but differ in their composition and target serogroups.
The meningococcal vaccine is administered via intramuscular injection, typically in the upper arm or thigh. The vaccine appears as a clear or slightly opaque liquid in a syringe, and the injection is quick and straightforward, often causing minimal discomfort.
Depending on the type and age of the recipient, the meningococcal vaccine may require one or more doses. Each dose is presented in the same form—a sterile liquid in a vial or pre-filled syringe—and is administered at specified intervals recommended by healthcare providers.