Conjugated vaccines for pneumonia represent a groundbreaking advancement in the prevention of pneumococcal diseases, which are caused by the bacterium *Streptococcus pneumoniae*. These vaccines work by linking a weak antigen (a polysaccharide from the bacterial capsule) to a strong carrier protein, enhancing the immune system's ability to recognize and respond to the pathogen. This conjugation process not only improves the vaccine's efficacy in young children and the elderly, who are most vulnerable to pneumonia, but also stimulates long-term immunity and immunological memory. By targeting multiple serotypes of *S. pneumoniae*, conjugated vaccines significantly reduce the incidence of invasive pneumococcal infections, including pneumonia, meningitis, and sepsis, thereby saving lives and reducing the burden on healthcare systems globally. Their introduction has marked a pivotal shift in public health strategies, offering robust protection against a leading cause of morbidity and mortality worldwide.
| Characteristics | Values |
|---|---|
| Mechanism of Action | Conjugated vaccines link a weak antigen (polysaccharide) from the pneumococcal bacteria to a strong carrier protein, enhancing immune response and immunological memory. |
| Target Population | Infants, young children, older adults, and immunocompromised individuals. |
| Vaccine Types | PCV7 (7-valent), PCV10 (10-valent), PCV13 (13-valent), PCV15 (15-valent), PCV20 (20-valent). |
| Serotypes Covered | Varies by vaccine (e.g., PCV13 covers 13 serotypes, PCV20 covers 20 serotypes). |
| Efficacy | High efficacy (70-90%) in preventing invasive pneumococcal disease (IPD) and pneumonia caused by covered serotypes. |
| Administration Route | Intramuscular injection. |
| Dosing Schedule | Varies by age group (e.g., infants: 3-dose series at 2, 4, and 6 months with a booster at 12-15 months). |
| Side Effects | Mild: pain at injection site, fever, irritability. Rare: severe allergic reactions. |
| Duration of Protection | Long-lasting immunity, with potential need for boosters in high-risk groups. |
| Herd Immunity | Reduces disease transmission by decreasing carriage of vaccine-type pneumococcal strains. |
| Serotype Replacement | Risk of non-vaccine serotypes causing disease, but overall disease burden remains reduced. |
| Global Impact | Significant reduction in pneumococcal disease incidence since introduction. |
| Storage Requirements | Refrigerated at 2-8°C (36-46°F) to maintain potency. |
| Cost-Effectiveness | Highly cost-effective in preventing hospitalizations and deaths from pneumococcal disease. |
| Latest Development | PCV15 and PCV20 approved in recent years to broaden serotype coverage. |
Explore related products






What You'll Learn
- Vaccine Composition: Contains purified polysaccharides linked to carrier proteins for enhanced immune response
- Mechanism of Action: Stimulates T-cell-dependent immunity, improving antibody production and memory response
- Targeted Pathogens: Protects against Streptococcus pneumoniae serotypes causing invasive pneumococcal disease
- Efficacy and Duration: Provides long-term protection, reducing pneumonia incidence and disease severity
- Population Benefits: Recommended for infants, elderly, and immunocompromised individuals to prevent complications
![]()
Vaccine Composition: Contains purified polysaccharides linked to carrier proteins for enhanced immune response
Conjugated vaccines for pneumonia are engineered to overcome the limitations of traditional polysaccharide vaccines, which often fail to elicit a robust immune response in young children and the elderly. The core innovation lies in their composition: purified polysaccharides from the bacterial capsule are chemically linked to carrier proteins. This strategic coupling transforms the immune response by engaging both T-cell and B-cell pathways, ensuring a more durable and effective defense against pneumococcal infection.
Consider the process as a molecular upgrade. Polysaccharides alone are poor immunogens, particularly in infants under two years old, whose immune systems are still maturing. By attaching them to carrier proteins like diphtheria toxoid or CRM197 (a non-toxic mutant of diphtheria toxin), the vaccine harnesses the protein’s ability to activate T-cells. This activation amplifies the immune response, leading to the production of high-affinity antibodies and immunological memory. For instance, the Prevnar 13® vaccine, recommended for children under five and adults over 65, uses CRM197 as the carrier protein, linking it to 13 distinct pneumococcal polysaccharides to provide broad serotype coverage.
The practical implications of this design are significant. Pediatric dosing typically involves a series of injections starting at two months of age, with boosters at four months, six months, and 12–15 months. Adults over 65 receive a single dose, often in conjunction with the pneumococcal polysaccharide vaccine (PPSV23) for comprehensive protection. The conjugation process ensures that even immunocompromised individuals, such as those with HIV or asplenia, can mount a protective response, though their dosing schedules may differ.
A critical takeaway is the balance between efficacy and safety. While conjugated vaccines are highly effective, their production is complex and costly due to the precise chemical linkage required. This complexity is reflected in their price, which can be a barrier in low-resource settings. However, initiatives like Gavi, the Vaccine Alliance, have expanded access to these vaccines globally, saving millions of lives annually. For parents and caregivers, ensuring timely vaccination according to regional health guidelines remains the most practical step to protect against pneumococcal disease.
In summary, the conjugated vaccine’s composition—purified polysaccharides linked to carrier proteins—represents a breakthrough in immunology. It addresses the innate weaknesses of polysaccharide antigens, particularly in vulnerable populations, by leveraging the immune system’s protein-recognition machinery. This design not only enhances antibody production but also fosters long-term immunity, making it a cornerstone of pneumonia prevention strategies worldwide.
Child Vaccinations: Ontario Parents' Rights and Responsibilities
You may want to see also
Explore related products






![]()
Mechanism of Action: Stimulates T-cell-dependent immunity, improving antibody production and memory response
Conjugate vaccines for pneumonia, such as the pneumococcal conjugate vaccine (PCV), harness the power of T-cell-dependent immunity to provide robust protection against Streptococcus pneumoniae, a leading cause of bacterial pneumonia. Unlike plain polysaccharide vaccines, which primarily elicit B-cell responses, conjugate vaccines link a weak antigen (polysaccharide) to a strong carrier protein (e.g., diphtheria toxoid). This linkage transforms the polysaccharide into a T-cell-dependent antigen, triggering a more vigorous and sustained immune response.
The mechanism unfolds in stages. Upon vaccination, antigen-presenting cells (APCs) engulf the conjugate vaccine and process it into smaller fragments. These fragments are then presented to T-helper cells via MHC class II molecules. Activated T-helper cells release cytokines, such as IL-4 and IL-5, which stimulate B-cells to proliferate and differentiate into plasma cells. Plasma cells secrete high-affinity antibodies specific to the polysaccharide antigen, effectively neutralizing encapsulated bacteria and preventing colonization in the lungs.
Memory response is a cornerstone of conjugate vaccine efficacy. Unlike plain polysaccharide vaccines, which induce short-lived immunity, conjugate vaccines generate long-lived memory B-cells and T-cells. Upon re-exposure to S. pneumoniae, memory cells rapidly activate, producing antibodies and coordinating an accelerated immune response. This memory response is particularly critical for vulnerable populations, such as infants and the elderly, who are at higher risk of pneumonia complications. For example, PCV13 (Prevnar 13) is administered in a 4-dose series to infants (2, 4, 6, and 12–15 months), ensuring robust immunity during early childhood when the risk of pneumococcal disease is highest.
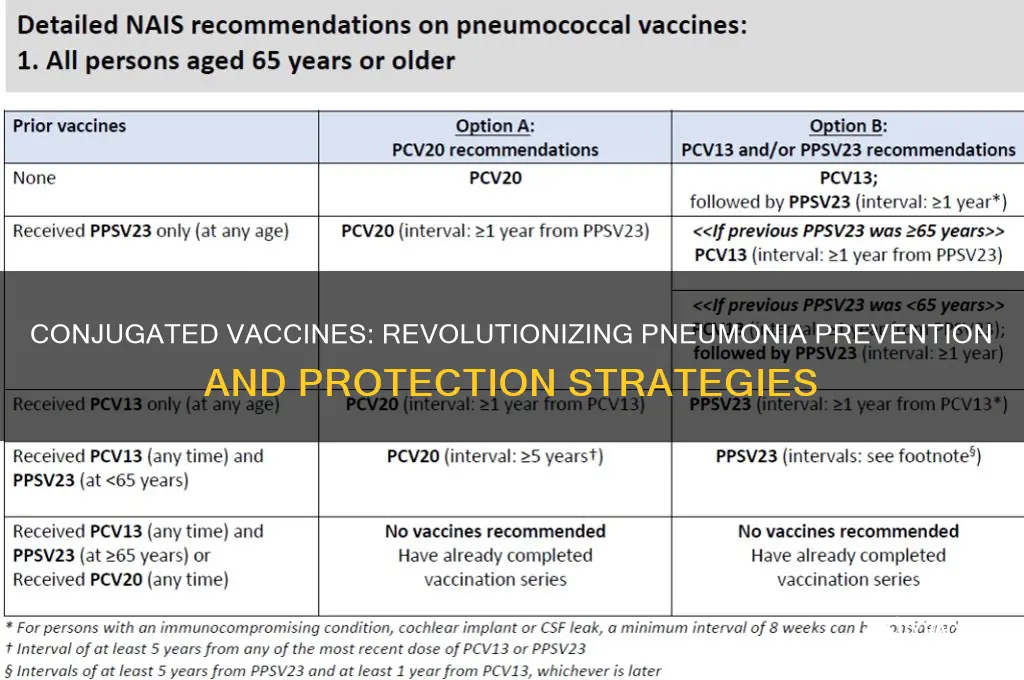
Practical considerations underscore the importance of this mechanism. Conjugate vaccines are highly effective in preventing invasive pneumococcal disease, including pneumonia, meningitis, and bacteremia. For adults aged 65 and older, a single dose of PCV20 (Prevnar 20) or PCV15 (Vaxneuvance) followed by a dose of PPSV23 (Pneumovax 23) at least one year later is recommended to maximize protection. This sequential approach leverages both T-cell-dependent and -independent pathways, ensuring broad coverage against pneumococcal serotypes. Adhering to age-specific dosing schedules and staying updated with evolving vaccine recommendations are essential for optimal protection.
In summary, conjugate vaccines for pneumonia stimulate T-cell-dependent immunity by coupling polysaccharide antigens to carrier proteins, enhancing antibody production and memory responses. This mechanism not only provides immediate protection but also ensures long-term immunity, making these vaccines indispensable tools in the fight against pneumococcal disease. By understanding this process, healthcare providers and individuals can make informed decisions to safeguard against pneumonia and its complications.
Polio Decline Mystery: Factors Reducing Cases Before Vaccine Arrival
You may want to see also
Explore related products






![]()
Targeted Pathogens: Protects against Streptococcus pneumoniae serotypes causing invasive pneumococcal disease
Conjugated pneumococcal vaccines are precision tools designed to target specific serotypes of *Streptococcus pneumoniae*, the bacterium responsible for invasive pneumococcal disease (IPD). Unlike traditional polysaccharide vaccines, which elicit a weaker immune response, conjugated vaccines chemically link pneumococcal polysaccharides to a carrier protein. This innovation enhances the immune system's ability to recognize and remember these serotypes, providing robust protection across diverse populations. The vaccines currently available, such as PCV13 (Prevnar 13) and PCV15, are formulated to cover the most prevalent and virulent serotypes associated with IPD, including pneumonia, meningitis, and sepsis.
The selection of serotypes in conjugated vaccines is no accident. Epidemiological data guide the inclusion of serotypes responsible for the majority of IPD cases globally. For instance, PCV13 targets 13 serotypes (1, 3, 4, 5, 6A, 6B, 7F, 9V, 14, 18C, 19A, 19F, and 23F), which historically accounted for up to 70% of IPD cases in children. PCV15 expands this coverage by adding serotypes 22F and 33F, addressing emerging strains not covered by earlier formulations. This targeted approach ensures that the vaccine maximizes protection against the most dangerous pathogens while minimizing the risk of serotype replacement, where non-vaccine serotypes fill the ecological niche left by vaccinated strains.
Administering conjugated pneumococcal vaccines follows a strict schedule tailored to age and risk factors. For infants, PCV13 is typically given in a series of four doses at 2, 4, 6, and 12–15 months of age. Adults aged 65 and older may receive a single dose of PCV15 or PCV20, followed by a dose of the polysaccharide vaccine PPSV23 at least one year later. Immunocompromised individuals or those with chronic conditions may require additional doses or earlier vaccination. Adhering to these schedules is critical, as incomplete vaccination can leave gaps in immunity, particularly against serotypes like 3 and 19A, which are associated with higher disease severity.
Despite their effectiveness, conjugated vaccines are not without limitations. Serotype replacement remains a concern, as evidenced by the rise of non-vaccine serotypes like 22F and 33F in regions with high PCV13 uptake. Additionally, the cost and accessibility of these vaccines pose challenges in low-resource settings, where IPD burden is often highest. To address these issues, ongoing research focuses on developing broader-coverage vaccines, such as PCV20, which includes 20 serotypes, and exploring alternative delivery methods, such as nasal sprays, to improve accessibility and compliance.
In practice, healthcare providers must balance the benefits of conjugated vaccines with individual patient needs. For example, adults with conditions like chronic heart disease or diabetes should prioritize pneumococcal vaccination, as they are at higher risk for IPD complications. Parents should also be educated about the importance of completing the infant vaccination series, as partial immunity can leave children vulnerable to invasive disease. By understanding the targeted nature of these vaccines and their limitations, healthcare professionals can optimize their use, ensuring maximum protection against the most dangerous *Streptococcus pneumoniae* serotypes.
Vaccines and Gut Health: Exploring Potential Impacts on the Microbiome
You may want to see also
Explore related products

$39.99 $59.99





![]()
Efficacy and Duration: Provides long-term protection, reducing pneumonia incidence and disease severity
Conjugate vaccines for pneumonia, such as the pneumococcal conjugate vaccine (PCV), have revolutionized the prevention of this life-threatening infection by offering robust, long-term protection. Clinical trials and real-world data consistently demonstrate that PCV reduces pneumonia incidence by 20–50%, depending on the population and serotype coverage. For instance, PCV13, which targets 13 strains of *Streptococcus pneumoniae*, has been shown to lower invasive pneumococcal disease by up to 75% in children under 5 years old. This efficacy extends beyond the vaccinated individual, as herd immunity reduces disease transmission in unvaccinated populations, particularly among the elderly and immunocompromised.
The duration of protection provided by conjugate vaccines is a critical factor in their success. Unlike plain polysaccharide vaccines, which elicit a weaker immune response, conjugate vaccines stimulate T-cell-dependent immunity, leading to the production of high-affinity antibodies and immunological memory. This mechanism ensures protection lasts for at least 5–10 years, often without the need for frequent boosters. For example, a single series of PCV13 doses in infancy (at 2, 4, 6, and 12–15 months) provides sustained immunity through childhood, the period of highest pneumonia risk. Adults aged 65 and older, who receive a single dose of PCV20 or PCV15 followed by a pneumococcal polysaccharide vaccine (PPSV23) a year later, experience reduced pneumonia-related hospitalizations for up to 8 years.
Practical considerations for maximizing vaccine efficacy include adhering to age-specific dosing schedules and ensuring timely administration. For infants, delaying doses beyond the recommended intervals can reduce immune response, so healthcare providers should emphasize the importance of timely vaccination. In low-resource settings, where pneumonia is a leading cause of childhood mortality, initiatives like Gavi’s vaccine distribution programs have significantly improved access to PCV, demonstrating that long-term protection is achievable even in challenging environments. However, ongoing surveillance is necessary to monitor serotype replacement, where non-vaccine strains emerge as causes of disease, requiring periodic updates to vaccine formulations.
A comparative analysis highlights the superiority of conjugate vaccines over earlier pneumococcal vaccines. While PPSV23 covers 23 serotypes, its efficacy wanes within 5 years and does not induce immunological memory, making it less effective in young children. Conjugate vaccines, by contrast, offer durable protection across a broad age range, from infancy to old age. This distinction underscores the importance of prioritizing conjugate vaccines in national immunization programs, particularly in regions with high pneumonia burden. For travelers or individuals at increased risk, combining PCV with PPSV23 provides comprehensive serotype coverage, further reducing disease severity and complications.
In conclusion, the long-term efficacy of conjugate vaccines in reducing pneumonia incidence and severity is a testament to their innovative design and immunological advantages. By following recommended dosing schedules, leveraging herd immunity, and addressing challenges like serotype replacement, these vaccines remain a cornerstone of pneumonia prevention globally. Their ability to provide sustained protection across diverse populations underscores their value as a public health intervention, saving millions of lives annually.
Hep A Vaccine Copay on SilverScript: What You Need to Know
You may want to see also
Explore related products






![]()
Population Benefits: Recommended for infants, elderly, and immunocompromised individuals to prevent complications
Conjugated vaccines for pneumonia, such as the pneumococcal conjugate vaccine (PCV), are specifically recommended for infants, the elderly, and immunocompromised individuals due to their heightened vulnerability to pneumococcal infections. These populations face increased risks of complications like bacteremia, meningitis, and severe pneumonia, which can be life-threatening. For infants, the Centers for Disease Control and Prevention (CDC) advises a PCV13 or PCV15 series starting at 2 months of age, with doses administered at 2, 4, 6, and 12–15 months. This early immunization builds robust immunity during a critical developmental period when the immune system is still maturing.
The elderly, particularly those over 65, benefit from a dual approach: PCV15 or PCV20 followed by the pneumococcal polysaccharide vaccine (PPSV23) at least one year later. This sequential regimen addresses age-related immune decline, known as immunosenescence, which reduces the body’s ability to fight infections. Immunocompromised individuals, including those with HIV, cancer, or organ transplants, require tailored vaccination schedules. For example, HIV-positive adults may need additional doses or closer monitoring of antibody responses. Practical tips for caregivers include ensuring timely vaccination, tracking doses with immunization records, and consulting healthcare providers for personalized plans.
Analyzing the impact, conjugated vaccines significantly reduce pneumococcal disease burden in these populations. Studies show PCV13 reduces invasive pneumococcal disease by 75% in infants and 45% in adults over 65. For immunocompromised individuals, vaccination lowers hospitalization rates by up to 60%. However, challenges persist, such as vaccine hesitancy and access disparities. Addressing these requires public health campaigns emphasizing the vaccines’ safety and efficacy, coupled with initiatives to improve healthcare accessibility.
Persuasively, the case for vaccination is clear: it’s a cost-effective intervention with proven population-level benefits. For instance, PCV introduction in the U.S. infant immunization schedule led to a 90% decline in pneumococcal hospitalizations among children under 5. Similarly, elderly vaccination programs in Europe reduced pneumonia-related deaths by 20%. Immunocompromised individuals, despite potential suboptimal responses, still gain partial protection that can prevent severe outcomes. Prioritizing these groups not only saves lives but also reduces healthcare costs and alleviates strain on medical systems.
Comparatively, conjugated vaccines offer advantages over older polysaccharide vaccines by inducing T-cell-dependent immunity, leading to longer-lasting protection and immunologic memory. This is particularly crucial for infants and the elderly, whose immune systems respond differently to polysaccharide antigens. For immunocompromised individuals, conjugated vaccines’ ability to stimulate both humoral and cellular immunity provides a more comprehensive defense. While no vaccine is 100% effective, the substantial reduction in disease incidence and severity underscores their indispensable role in preventive care.
In conclusion, conjugated pneumococcal vaccines are a cornerstone of public health for infants, the elderly, and immunocompromised individuals. Adhering to recommended schedules, addressing barriers to access, and fostering awareness can maximize their population-level impact. By preventing complications and reducing mortality, these vaccines not only protect vulnerable groups but also contribute to broader community health and resilience.
New Zealand's Vaccination Policy: Are Mandatory Vaccinations Required?
You may want to see also
Frequently asked questions
Conjugated vaccines for pneumonia are vaccines that protect against *Streptococcus pneumoniae*, the bacteria responsible for pneumococcal diseases like pneumonia, meningitis, and sepsis. These vaccines combine a weak or inactive part of the bacteria (polysaccharide) with a protein carrier, enhancing the immune response, especially in young children and older adults.
Conjugated vaccines stimulate the immune system to produce antibodies against the polysaccharide capsule of *S. pneumoniae*. By linking the polysaccharide to a protein carrier, the vaccine triggers a stronger and longer-lasting immune response, enabling the body to recognize and fight the bacteria more effectively.
Conjugated vaccines are recommended for infants, young children, adults over 65, and individuals with certain medical conditions (e.g., weakened immune systems, chronic illnesses) who are at higher risk of pneumococcal infections. Specific recommendations vary by country and vaccine type (e.g., PCV13, PCV20).
Common side effects include mild pain, redness, or swelling at the injection site, fever, fatigue, and muscle aches. These symptoms are usually mild and resolve within a few days. Serious side effects are rare but can include severe allergic reactions. Always consult a healthcare provider if concerns arise.































