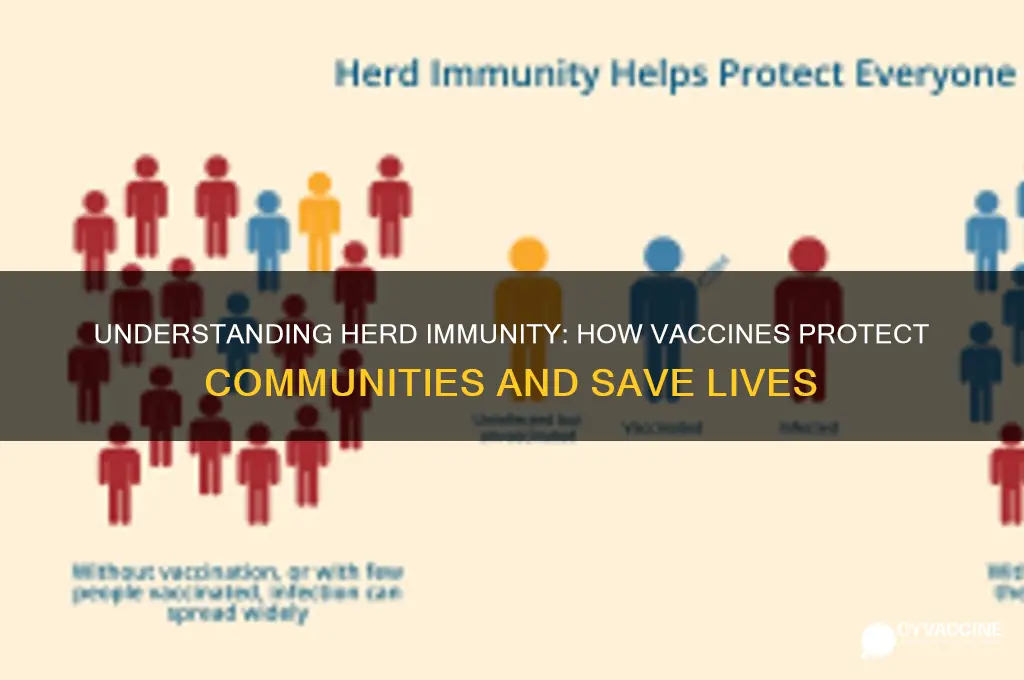
Vaccines achieve herd immunity by providing a critical level of protection within a population, reducing the spread of infectious diseases even among those who are not vaccinated. When a significant portion of the community is immunized, it becomes difficult for a disease to circulate, as the chain of infection is disrupted. This collective immunity shields vulnerable individuals who cannot receive vaccines due to medical reasons, such as infants, the elderly, or those with compromised immune systems. By lowering the overall prevalence of the disease, vaccines not only protect individuals but also minimize the likelihood of outbreaks, ultimately creating a safer environment for everyone. Herd immunity is a powerful public health tool, demonstrating the importance of widespread vaccination in preventing the resurgence of preventable diseases.
Explore related products






What You'll Learn
- Vaccine Coverage Rates: Percentage of population vaccinated needed to disrupt disease spread effectively
- Immunity Thresholds: Minimum immunity level required to protect unvaccinated individuals
- Disease Transmission Reduction: Vaccines lower infection rates, limiting opportunities for disease spread
- Protection of Vulnerable Groups: Herd immunity shields those unable to receive vaccines
- Vaccine Efficacy and Duration: How well and how long vaccines prevent disease transmission
![]()
Vaccine Coverage Rates: Percentage of population vaccinated needed to disrupt disease spread effectively
The threshold for herd immunity varies dramatically by disease, hinging on a metric called the *basic reproduction number (R₀)*. This represents the average number of people one infected individual would transmit to in an unvaccinated population. Measles, with an R₀ of 12-18, requires approximately 93-95% of the population vaccinated to disrupt spread. In contrast, diseases like pertussis (R₀ ~5-6) need roughly 85-92% coverage, while polio (R₀ ~5-7) historically required 80-86% before eradication efforts. Understanding these thresholds is critical for public health planning, as even small gaps in coverage can allow outbreaks to ignite.
Achieving these percentages isn’t just about numbers—it’s about strategy. For instance, measles vaccines are typically administered in two doses: the first at 12-15 months and the second at 4-6 years. Ensuring timely completion of this schedule is vital, as even a single missed dose can leave individuals susceptible. Public health campaigns must target not only children but also adults who may lack immunity, particularly in regions with historical vaccine hesitancy. Mobile clinics, school-based programs, and workplace initiatives can bridge gaps, but success relies on consistent messaging and accessible healthcare infrastructure.
A comparative analysis reveals that herd immunity thresholds are not static. Emerging variants can alter a disease’s R₀, necessitating higher coverage rates. For example, the Delta variant of COVID-19 had an R₀ of ~5-8, initially requiring 70-85% vaccination coverage. However, the more transmissible Omicron variant pushed this threshold closer to 90%, highlighting the need for adaptable strategies. Booster doses, tailored to evolving strains, become essential in maintaining herd immunity, particularly in populations with waning immunity or incomplete initial vaccination series.
Persuasively, the economic and social benefits of meeting these thresholds cannot be overstated. Every percentage point gained in vaccine coverage reduces healthcare costs, prevents productivity losses, and saves lives. For instance, the measles vaccine alone prevents an estimated 3-4 million deaths annually globally. Yet, achieving these rates demands addressing misinformation, improving healthcare access, and fostering community trust. Policymakers must prioritize evidence-based communication, incentivize vaccination, and ensure equitable distribution to turn theoretical thresholds into tangible public health victories.
Vaccine Misconceptions: Historical Instances of Proven Errors and Myths
You may want to see also
Explore related products






![]()
Immunity Thresholds: Minimum immunity level required to protect unvaccinated individuals
Vaccines don’t just protect individuals; they create a shield around communities by reaching immunity thresholds, the minimum percentage of a population that must be immune to interrupt disease spread. This threshold varies by pathogen. For measles, one of the most contagious diseases, 93–95% of the population must be immune to achieve herd immunity. In contrast, pertussis (whooping cough) requires around 92–94%, while polio needs 80–86%. These numbers aren’t arbitrary—they’re calculated using the basic reproduction number (R0), which measures how many people one infected individual can transmit the disease to in an unvaccinated population. The higher the R0, the higher the immunity threshold.
Achieving these thresholds isn’t just about vaccinating everyone; it’s about protecting the vulnerable. Infants too young for certain vaccines, immunocompromised individuals, and those with vaccine allergies rely on herd immunity to stay safe. For example, the MMR vaccine (measles, mumps, rubella) is typically given at 12–15 months, leaving younger children unprotected. Similarly, cancer patients undergoing chemotherapy may have weakened immune systems, making them dependent on community immunity. Even a small drop below the threshold can lead to outbreaks, as seen in measles resurgences in communities with vaccination rates below 93%.
Reaching immunity thresholds requires strategic planning. Vaccination campaigns must target specific age groups and geographic areas. For instance, during a measles outbreak, public health officials might prioritize vaccinating school-aged children, who are both highly susceptible and likely to spread the disease. Booster doses also play a critical role, as immunity can wane over time. For tetanus, adults need boosters every 10 years, while pertussis boosters are recommended during pregnancy to protect newborns. Practical tips include using reminder systems for vaccine appointments and offering vaccines in accessible locations like schools or workplaces.
However, maintaining these thresholds is challenging. Vaccine hesitancy, misinformation, and logistical barriers can hinder progress. In 2019, the WHO listed vaccine hesitancy as one of the top 10 global health threats. To counter this, public health initiatives must combine education with accessibility. For example, debunking myths about vaccine safety through trusted sources like pediatricians can build confidence. Additionally, offering vaccines at low or no cost removes financial barriers. Comparative data shows that countries with high vaccination rates, like Portugal (95% measles vaccination), have fewer outbreaks than those with lower rates, such as Ukraine (85% in 2019).
In conclusion, immunity thresholds are a delicate balance between biology, behavior, and policy. They require sustained effort, accurate data, and community engagement. By understanding these thresholds and taking targeted action, societies can protect not only the vaccinated but also those who cannot be immunized. The goal isn’t just to reach the threshold—it’s to stay above it, ensuring that herd immunity remains a shield, not a statistic.
Should Vaccinations Be Mandatory in the United States? A Debate
You may want to see also
Explore related products






![]()
Disease Transmission Reduction: Vaccines lower infection rates, limiting opportunities for disease spread
Vaccines act as a firewall against disease transmission by significantly lowering infection rates. When a critical portion of the population is immunized, the virus or bacteria encounters a series of immune roadblocks, making it difficult to find susceptible hosts. This disruption in the chain of infection is the cornerstone of herd immunity. For instance, measles, a highly contagious disease, requires approximately 95% vaccination coverage to achieve herd immunity. At this threshold, the virus struggles to sustain transmission, effectively protecting vulnerable individuals who cannot be vaccinated due to medical reasons.
Consider the mechanics of this process. Each vaccinated individual becomes a dead end for the pathogen, reducing the effective reproduction number (R0) of the disease. R0 represents the average number of people one infected person will infect in a fully susceptible population. For example, the R0 of measles is 12-18, meaning one person can infect 12-18 others without immunity. Vaccination lowers this number, and when R0 falls below 1, the disease begins to die out. This principle is evident in the near-eradication of polio, where global vaccination efforts reduced cases by 99% from 1988 to 2020, limiting transmission to just a few remaining regions.
Practical implementation of this strategy requires careful planning. Vaccination campaigns must target specific age groups and communities to maximize impact. For instance, influenza vaccines are annually administered to the elderly and healthcare workers, who are both at higher risk and more likely to spread the virus. Similarly, school-based vaccination programs for diseases like mumps and rubella not only protect children but also reduce community-wide transmission. Ensuring consistent vaccine uptake, even for diseases perceived as less threatening, is crucial to maintaining herd immunity.
However, challenges exist. Vaccine hesitancy and inequitable access can create gaps in immunity, allowing diseases to persist or re-emerge. For example, the 2019 measles outbreak in the U.S. was linked to declining vaccination rates in certain communities, highlighting the fragility of herd immunity. To counter this, public health initiatives must combine education, accessibility, and policy measures. Incentives like vaccine passports or school mandates, while controversial, have proven effective in boosting coverage. Ultimately, the success of herd immunity hinges on collective action, where each vaccinated individual contributes to a safer, healthier population.
Retrieve Your CVS Vaccination Proof: A Quick and Easy Guide
You may want to see also
Explore related products





![]()
Protection of Vulnerable Groups: Herd immunity shields those unable to receive vaccines
Vaccines are not a one-size-fits-all solution. For individuals with compromised immune systems, severe allergies, or certain medical conditions, vaccination may be impossible or risky. This includes people undergoing chemotherapy, organ transplant recipients, and those with specific genetic disorders. Herd immunity acts as a protective barrier for these vulnerable groups, reducing their exposure to pathogens and lowering the likelihood of outbreaks.
Without this collective shield, they face heightened risks of infection, severe illness, and even death.
Consider measles, a highly contagious virus. The measles vaccine, typically administered in two doses (the first at 12-15 months and the second at 4-6 years), provides robust immunity. When vaccination rates reach approximately 95%, herd immunity is achieved, effectively halting the virus's spread. This protects not only the vaccinated but also infants too young for vaccination, individuals with vaccine contraindications, and those with waning immunity. A real-world example is the 2019 measles outbreak in the US, where communities with lower vaccination rates saw a disproportionate number of cases among vulnerable populations.
This highlights the critical role herd immunity plays in safeguarding those who cannot directly benefit from vaccines.
Achieving herd immunity requires a multi-pronged approach. Firstly, maintaining high vaccination coverage is paramount. This involves addressing vaccine hesitancy through education, accessible healthcare, and transparent communication about vaccine safety and efficacy. Secondly, public health measures like contact tracing and isolation remain crucial during outbreaks, especially to protect vulnerable individuals. Finally, ongoing research into alternative protection methods, such as immunoglobulin therapy or targeted antiviral treatments, can provide additional layers of defense for those unable to receive vaccines.
It's important to remember that herd immunity is not a static state. New variants, waning immunity, and changing population demographics can all impact its effectiveness. Continuous monitoring of disease prevalence, vaccination rates, and immune status within communities is essential for identifying vulnerabilities and adapting strategies accordingly. By prioritizing herd immunity, we not only protect the majority but also extend a vital shield to those who rely on collective immunity for their survival.
Understanding India's Whooping Cough Vaccine: Name, Availability, and Importance
You may want to see also
Explore related products






![]()
Vaccine Efficacy and Duration: How well and how long vaccines prevent disease transmission
Vaccines are not just individual shields against disease; they are collective weapons that can halt the spread of pathogens in their tracks. But their power to achieve herd immunity hinges on two critical factors: efficacy and duration. Efficacy refers to how well a vaccine prevents disease transmission, while duration measures how long this protection lasts. Understanding these elements is crucial for designing vaccination strategies that not only protect individuals but also shield entire communities.
Consider the measles vaccine, a prime example of high efficacy. A single dose provides approximately 93% protection, while two doses boost this to 97%. This high efficacy, combined with widespread vaccination, has led to a dramatic decline in measles cases globally. However, efficacy varies by vaccine. For instance, the flu vaccine’s efficacy ranges from 40% to 60% annually, depending on the match between the vaccine strain and circulating viruses. This lower efficacy means herd immunity against influenza is harder to achieve, requiring higher vaccination rates and annual updates to the vaccine formulation.
Duration of protection is equally vital. Some vaccines, like the MMR (measles, mumps, rubella), offer lifelong immunity after a complete series, typically administered between 12 and 15 months of age, followed by a booster at 4 to 6 years. Others, such as the tetanus vaccine, require periodic boosters every 10 years to maintain immunity. COVID-19 vaccines present a unique challenge, as their duration of protection is still being studied. Initial data suggests that efficacy wanes over time, with protection against symptomatic infection dropping from around 95% to 60-70% after six months, necessitating booster doses for sustained herd immunity.
Practical considerations further complicate the picture. Age, underlying health conditions, and even geographic location can influence both efficacy and duration. For example, older adults may mount a weaker immune response to vaccines like the flu shot, prompting the development of high-dose formulations specifically for this demographic. Similarly, travelers to regions with high disease prevalence may require additional doses or earlier boosters to ensure continued protection.
To maximize the impact of vaccines on herd immunity, public health strategies must account for these nuances. This includes monitoring vaccine efficacy in real-world settings, adjusting dosing schedules as needed, and ensuring equitable access to vaccines globally. By understanding and addressing the complexities of vaccine efficacy and duration, we can build a more resilient defense against infectious diseases, one dose at a time.
Is Refusing Childhood Vaccinations in Vermont a Form of Maltreatment?
You may want to see also
Frequently asked questions
Herd immunity occurs when a large portion of a community becomes immune to a disease, making its spread unlikely. Vaccines contribute by providing immunity to individuals, reducing the number of susceptible hosts and slowing or stopping disease transmission.
The percentage of people needing vaccination for herd immunity varies by disease. For highly contagious diseases like measles, 90–95% of the population must be immune, while for less contagious diseases, the threshold may be lower, around 70–85%.
Herd immunity can occur naturally when enough people become immune after contracting and recovering from a disease. However, this approach often leads to widespread illness and deaths. Vaccines provide a safer and more controlled way to achieve herd immunity without the risks of natural infection.