Polio, a highly infectious disease caused by the poliovirus, primarily affects the nervous system and can lead to paralysis or even death. While vaccination has drastically reduced its global prevalence, the risk of contracting polio without immunization remains a significant concern, particularly in regions with low vaccination rates or inadequate healthcare infrastructure. Unvaccinated individuals are highly susceptible to the virus, which spreads through contaminated food, water, or fecal-oral transmission. In areas where polio is still endemic or where vaccine coverage is insufficient, outbreaks can occur, posing a serious threat to public health. Understanding the likelihood of contracting polio without vaccination underscores the critical importance of global immunization efforts to eradicate this preventable disease.
Explore related products



$11.93 $21.99



What You'll Learn
![]()
Polio transmission rates in unvaccinated populations
Polio, caused by the poliovirus, is a highly contagious disease that primarily affects young children. Before the introduction of effective vaccines in the 1950s, polio was widespread, causing outbreaks that led to paralysis and death in significant numbers. In unvaccinated populations, the transmission rates of polio are alarmingly high due to the virus’s efficient spread through fecal-oral and oral-oral routes. Even a small amount of the virus shed in the feces of an infected person can contaminate water or food, leading to rapid transmission within communities, especially in areas with poor sanitation.
In regions where vaccination coverage is low or nonexistent, the risk of contracting polio increases dramatically. Historical data shows that in the absence of vaccination, nearly every person in a population would become infected with the poliovirus at some point during their lifetime. However, only about 5% of those infected develop symptoms, which can range from mild flu-like illness to severe paralysis. The asymptomatic nature of most infections means the virus can silently circulate in unvaccinated populations, making it difficult to control without immunization.
Transmission rates are particularly high in crowded settings, such as urban slums or refugee camps, where close contact and inadequate hygiene facilitate the virus’s spread. Children under five are the most vulnerable, as their immune systems are still developing, and they are more likely to come into contact with contaminated environments. In unvaccinated populations, the basic reproduction number (R0) of polio—the average number of people one infected person can infect—is estimated to be between 5 and 7, indicating its high transmissibility.
Efforts to eradicate polio globally have significantly reduced its incidence, but the disease remains a threat in areas with low vaccination coverage. Countries with ongoing transmission, such as Afghanistan and Pakistan, highlight the importance of maintaining high immunization rates. Without vaccination, polio can re-emerge rapidly, as seen in recent outbreaks in under-vaccinated communities. These outbreaks underscore the critical role of vaccines in preventing transmission and protecting populations from this debilitating disease.
Understanding the transmission dynamics in unvaccinated populations is essential for public health strategies. Polio’s ability to spread silently and cause severe outcomes in a small but significant proportion of cases makes vaccination the most effective tool for prevention. Global health initiatives, such as the Global Polio Eradication Initiative, emphasize the need for sustained vaccination campaigns to interrupt transmission and achieve eradication. Without these efforts, the high transmission rates observed historically would persist, posing a continued risk to global health.
Monkeypox Vaccine: Scar Concerns and Facts
You may want to see also
Explore related products






![]()
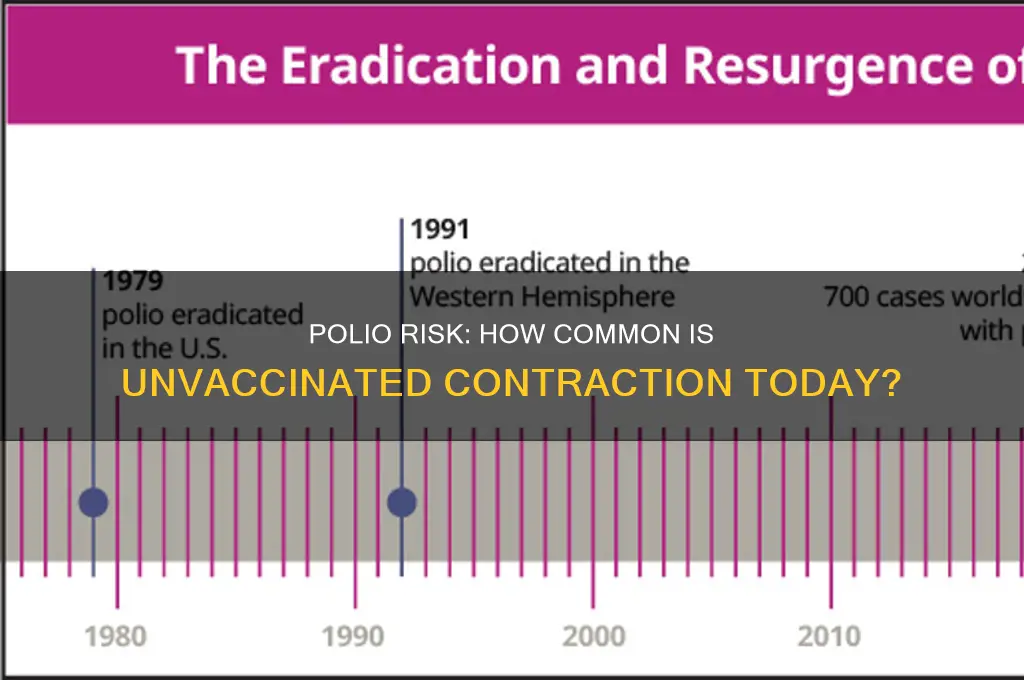
Global polio incidence before widespread vaccination
Before the introduction of widespread polio vaccination in the mid-20th century, poliomyelitis was a widespread and feared disease with devastating global incidence. Historical data indicates that polio was endemic in nearly every country, affecting both developed and developing nations alike. The virus, primarily transmitted through fecal-oral routes or contaminated water and food, thrived in areas with poor sanitation and crowded living conditions. In the early 20th century, polio epidemics were frequent, particularly during the summer and fall months, earning it the moniker "summer plague." Without vaccination, populations were highly susceptible to the virus, with children under the age of five being the most vulnerable.
The global incidence of polio before vaccination was alarmingly high, with millions of cases reported annually. In the United States alone, polio outbreaks in the 1940s and 1950s resulted in over 15,000 cases of paralysis each year. Globally, the World Health Organization (WHO) estimates that before vaccination, there were approximately 350,000 cases of paralytic polio annually. However, this number is likely an underestimation, as many cases went unreported, especially in regions with limited healthcare infrastructure. The disease's prevalence was so significant that it became a leading cause of disability worldwide, leaving survivors with lifelong physical impairments.
In regions with high population density and inadequate sanitation, the risk of contracting polio without vaccination was particularly acute. For instance, in India, Egypt, and other parts of Asia and Africa, polio was hyperendemic, meaning the virus circulated continuously, causing frequent outbreaks. In these areas, it was common for a significant portion of the population to be exposed to the virus during childhood, with a small percentage developing paralytic symptoms. The lack of immunity in unvaccinated populations allowed the virus to spread rapidly, making polio a constant threat to public health.
The severity of polio's impact before vaccination is further highlighted by its socioeconomic consequences. Families and communities bore the burden of caring for disabled individuals, often with limited resources. The disease also strained healthcare systems, as hospitals and clinics were overwhelmed during outbreaks. In many cases, entire communities lived in fear of polio, with public spaces like swimming pools and movie theaters being avoided during peak seasons. This pervasive fear underscored the urgent need for a preventive measure, which eventually came in the form of the polio vaccine.
Historically, the natural immunity to polio was low, as only a small fraction of infections resulted in paralysis or death, while the majority experienced mild or asymptomatic cases. However, this meant that a large portion of the population remained susceptible to the virus. Without vaccination, the cycle of transmission continued unabated, ensuring the disease's persistence. The development and distribution of the polio vaccine in the 1950s and 1960s marked a turning point, drastically reducing global incidence and paving the way for its near eradication in the 21st century. This contrast between the pre-vaccination era and the present day underscores the critical importance of immunization in controlling infectious diseases.
Oxford Vaccine: Effective Against New Variants?
You may want to see also
Explore related products






![]()
Risk factors for contracting polio without immunity
Polio, caused by the poliovirus, primarily spreads through person-to-person contact, contaminated food and water, and respiratory droplets. Without vaccination, the risk of contracting polio increases significantly, especially in regions where the virus is still endemic or where vaccination rates are low. The poliovirus is highly contagious, and individuals without immunity are particularly vulnerable. Understanding the risk factors for contracting polio without immunity is crucial for prevention and public health strategies.
One of the primary risk factors is living in or traveling to areas with ongoing polio transmission. Countries with low vaccination coverage, poor sanitation, and limited access to clean water are hotspots for polio outbreaks. In these regions, the virus can circulate freely, increasing the likelihood of exposure for unvaccinated individuals. Travelers to such areas, especially those who have not received the polio vaccine, are at a heightened risk of infection. Even brief visits can lead to exposure, as the virus can spread rapidly in crowded or unsanitary conditions.
Close contact with an infected person is another significant risk factor. The poliovirus is shed in the feces and can also be present in the throat of an infected individual. Direct contact with contaminated fecal matter or respiratory secretions can transmit the virus to unvaccinated individuals. This risk is particularly high in households or communities where someone has polio, as the virus can easily spread through shared utensils, food, or water. Children are especially susceptible due to their frequent hand-to-mouth activities and close interactions with peers.
Poor sanitation and hygiene practices exacerbate the risk of contracting polio without immunity. In areas where access to clean water and proper sewage disposal is limited, the poliovirus can contaminate water sources and food supplies. Consuming contaminated food or water is a direct route of infection. Additionally, lack of handwashing facilities and practices increases the likelihood of transferring the virus from contaminated surfaces to the mouth, particularly in children. Improving sanitation and hygiene is therefore a critical component of polio prevention in at-risk communities.
Finally, individuals with weakened immune systems face a higher risk of contracting polio if they are not vaccinated. Conditions such as HIV/AIDS, malnutrition, or certain medical treatments that suppress the immune system can make it easier for the poliovirus to establish an infection. These individuals may also experience more severe symptoms if they contract the disease. Ensuring that vulnerable populations have access to the polio vaccine is essential to reducing their risk of infection and preventing complications.
In summary, the risk factors for contracting polio without immunity include living in or traveling to endemic areas, close contact with infected individuals, poor sanitation and hygiene, and having a compromised immune system. Vaccination remains the most effective way to prevent polio, and addressing these risk factors through public health interventions is vital to eradicating the disease globally.
Vaccines: Autoimmune Families Face a Tough Choice
You may want to see also
Explore related products






![]()
Historical polio outbreaks in non-vaccinated communities
Before the introduction of the polio vaccine in the 1950s, poliomyelitis was a widespread and feared disease, particularly in non-vaccinated communities. Historical records show that polio outbreaks were common, especially during the summer and early autumn months, often referred to as the "polio season." In the early 20th century, polio epidemics swept through cities and towns, leaving thousands of children and adults paralyzed or dead. For instance, the United States experienced its largest polio outbreak in 1952, with over 57,000 cases reported, a significant portion of which occurred in non-vaccinated populations. This outbreak highlighted the devastating impact of the disease in the absence of immunization.
Non-vaccinated communities, particularly in developing countries or regions with limited access to healthcare, were disproportionately affected by polio. In the 1940s and 1950s, countries like India, China, and parts of Africa saw recurrent polio outbreaks that crippled entire communities. The lack of vaccination meant that the virus spread rapidly, especially in crowded urban areas with poor sanitation. Children under the age of five were the most vulnerable, with up to 1 in 200 infections leading to irreversible paralysis. These outbreaks underscored the critical need for a vaccine to control the disease.
Historical data from Europe also reveals the severity of polio in non-vaccinated populations. In the 1950s, countries like Sweden and the United Kingdom experienced significant outbreaks, with thousands of cases reported annually. For example, during the 1953 outbreak in the UK, over 5,000 people were paralyzed, and 300 died. These incidents were a stark reminder of how common and severe polio could be without the protection of vaccination. Public health campaigns often focused on isolation and quarantine measures, but these were largely ineffective in preventing widespread transmission.
In isolated or remote communities, polio outbreaks were particularly devastating due to the lack of medical infrastructure and access to vaccines. For instance, in the 1940s, rural areas of Australia and Canada experienced localized outbreaks that had long-lasting effects on small populations. Without vaccination, these communities relied on rudimentary containment strategies, which often failed to stop the virus from spreading. The introduction of the polio vaccine in the mid-20th century marked a turning point, drastically reducing the incidence of the disease in vaccinated populations and highlighting the stark contrast with non-vaccinated areas.
The history of polio outbreaks in non-vaccinated communities serves as a critical lesson in the importance of immunization. Before vaccination, contracting polio was relatively common, with global estimates suggesting millions of cases annually. The disease not only caused physical disability but also had profound social and economic impacts on affected communities. The success of polio eradication efforts in many parts of the world today is a direct result of widespread vaccination, making the disease rare in countries with high immunization rates. However, in regions where vaccination remains inaccessible or is refused, the risk of outbreaks persists, as evidenced by recent cases in under-vaccinated communities.
Vaccines: Stopping Omicron's Spread?
You may want to see also
Explore related products






![]()
Current polio cases in areas with low vaccination rates
Polio, a highly infectious disease caused by the poliovirus, has been nearly eradicated globally due to widespread vaccination efforts. However, in areas with low vaccination rates, the risk of contracting polio remains a significant concern. Current data indicates that regions with vaccination coverage below 80% are particularly vulnerable to outbreaks. These areas often face challenges such as limited access to healthcare, vaccine hesitancy, and political instability, which hinder immunization campaigns. As a result, polio continues to circulate in these communities, posing a threat not only to the unvaccinated but also to those with incomplete vaccination status.
In countries like Afghanistan and Pakistan, which are the last remaining endemic countries for polio, low vaccination rates have led to persistent cases. For instance, in 2023, Afghanistan reported several cases of wild poliovirus, primarily in regions where vaccine accessibility is compromised due to conflict and logistical barriers. Similarly, Pakistan has seen sporadic cases in areas with low immunization coverage, often linked to misinformation and mistrust of vaccination programs. These cases highlight the direct correlation between low vaccination rates and the prevalence of polio, emphasizing the need for targeted interventions to improve vaccine uptake.
Beyond endemic countries, polio outbreaks have also occurred in regions with previously low vaccination rates, such as parts of Africa and the Middle East. For example, in 2022, Malawi and Mozambique reported cases of wild poliovirus after decades of being polio-free, attributed to gaps in vaccination coverage. These outbreaks serve as a stark reminder that polio can resurface in any area where herd immunity is not maintained. The virus can spread rapidly among unvaccinated populations, particularly in densely populated or underserved communities, making it critical to address vaccination gaps promptly.
The risk of contracting polio without vaccination is alarmingly high in these low-coverage areas. Studies show that in populations with less than 70% vaccination coverage, the likelihood of polio transmission increases exponentially. Unvaccinated individuals are not only at risk of severe paralysis but also contribute to the virus's continued circulation, potentially leading to new outbreaks. This underscores the importance of achieving and sustaining high vaccination rates to interrupt polio transmission and prevent its resurgence.
Efforts to combat polio in low-vaccination regions include strengthening routine immunization, conducting targeted vaccination campaigns, and addressing community concerns through education and engagement. Global health organizations, such as the World Health Organization (WHO) and UNICEF, are working with local governments to improve vaccine accessibility and build trust in immunization programs. However, sustained political commitment and resources are essential to ensure that every child, regardless of their location, is protected from this preventable disease. Until global vaccination coverage is consistently high, the threat of polio in underserved areas will persist, making it a critical focus for public health initiatives.
Did Fetal Cells End Polio? Salk's Vaccine Legacy
You may want to see also
Frequently asked questions
In countries with high vaccination rates, contracting polio without vaccination is extremely rare due to herd immunity, which limits the virus's spread.
In areas with active polio outbreaks, the risk of contracting the virus without vaccination is significantly higher, especially among children and unvaccinated populations.
In developed countries with robust vaccination programs, polio transmission without vaccination is virtually nonexistent, as the disease has been eradicated or controlled.
Without vaccination, the likelihood of contracting polio if exposed to the virus is high, as the body lacks immunity to fight the infection effectively.