Anaphylaxis, a severe and potentially life-threatening allergic reaction, is a rare but significant concern associated with vaccinations. While vaccines are generally safe and effective in preventing diseases, there is a small risk of anaphylactic reactions, typically occurring within minutes to hours after administration. The incidence of anaphylaxis from vaccines is estimated to be approximately 1.3 cases per million doses, with certain vaccines, such as those for influenza and COVID-19, having slightly higher reported rates. Understanding the prevalence and risk factors of vaccine-induced anaphylaxis is crucial for healthcare providers to ensure prompt recognition, management, and patient safety during immunization programs.
Explore related products





What You'll Learn
- Vaccine Types and Risk: Different vaccines have varying anaphylaxis risks; mRNA vaccines are closely monitored
- Prevalence Rates: Anaphylaxis occurs in 1.3 to 5 cases per million vaccine doses
- Risk Factors: History of allergies, asthma, or prior anaphylaxis increases vaccine reaction risk
- Symptoms and Timing: Symptoms typically appear within minutes to hours after vaccination
- Prevention and Management: Pre-vaccination screening and epinephrine availability reduce severe outcomes
![]()
Vaccine Types and Risk: Different vaccines have varying anaphylaxis risks; mRNA vaccines are closely monitored
Anaphylaxis from vaccines is a rare but serious concern, with incidence rates varying significantly across different vaccine types. For instance, mRNA vaccines like Pfizer-BioNTech and Moderna have reported anaphylaxis rates of approximately 2 to 5 cases per million doses administered, according to the Centers for Disease Control and Prevention (CDC). In contrast, traditional vaccines such as the influenza vaccine have an even lower risk, with anaphylaxis occurring in about 1.3 cases per million doses. These disparities highlight the importance of understanding the specific risks associated with each vaccine type.
Analyzing the mechanisms behind these differences reveals that vaccine components play a critical role. mRNA vaccines, for example, contain polyethylene glycol (PEG), a potential allergen that has been linked to anaphylactic reactions in some individuals. Traditional vaccines, on the other hand, often use different adjuvants and stabilizers, which may pose a lower risk for hypersensitivity reactions. Healthcare providers must remain vigilant, particularly when administering mRNA vaccines, as these are relatively new and their long-term effects are still under close monitoring.
Practical precautions can mitigate the risk of anaphylaxis during vaccination. For mRNA vaccines, the CDC recommends observing recipients for 15–30 minutes post-injection, with a 30-minute wait advised for individuals with a history of severe allergic reactions. Epinephrine auto-injectors should be readily available at vaccination sites to manage any immediate adverse events. Additionally, individuals with known PEG allergies should consult an allergist before receiving an mRNA vaccine, as alternative options may be more suitable.
Comparatively, the risk-benefit analysis strongly favors vaccination across all age groups, despite the rare occurrence of anaphylaxis. For example, the risk of severe COVID-19 complications in adults over 65 far outweighs the minimal anaphylaxis risk from mRNA vaccines. Similarly, childhood vaccines, such as those for measles or mumps, have anaphylaxis rates below 1 case per million doses, making them essential for public health. Understanding these risks empowers individuals and healthcare providers to make informed decisions while ensuring safety.
In conclusion, while anaphylaxis from vaccines is rare, the risk varies by vaccine type, with mRNA vaccines warranting closer monitoring due to their unique components. By implementing targeted precautions and staying informed, both providers and recipients can navigate vaccination safely, maximizing benefits while minimizing risks. This tailored approach underscores the importance of individualized care in public health initiatives.
Salmonella Vaccination Practices on US Poultry Farms: A Comprehensive Overview
You may want to see also
Explore related products






![]()
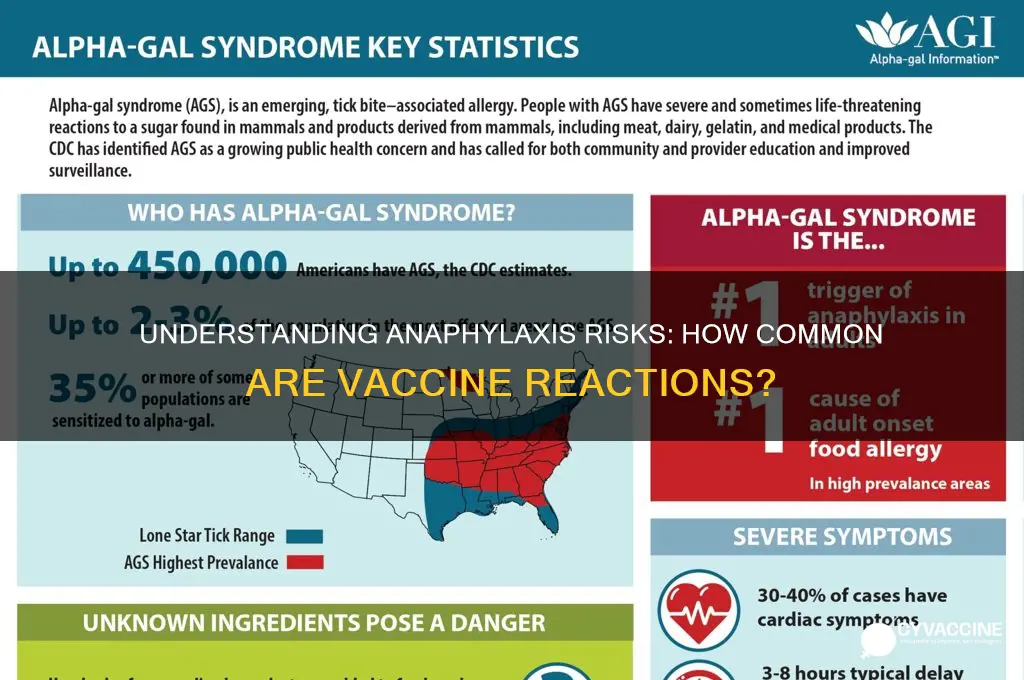
Prevalence Rates: Anaphylaxis occurs in 1.3 to 5 cases per million vaccine doses
Anaphylaxis from vaccines is a rare but serious event, with prevalence rates estimated at 1.3 to 5 cases per million doses administered. To put this in perspective, if a city of one million people were vaccinated, only a handful—between 1.3 and 5 individuals—would experience this severe allergic reaction. These numbers are derived from extensive monitoring systems, such as the Vaccine Adverse Event Reporting System (VAERS) in the United States and similar programs globally, which track vaccine safety in real time. Understanding these rates is crucial for both healthcare providers and the public to weigh the benefits of vaccination against the minimal risk of anaphylaxis.
Analyzing these figures reveals that anaphylaxis is not a common occurrence but remains a critical consideration in vaccine administration. The risk varies slightly depending on the vaccine type; for instance, mRNA COVID-19 vaccines have shown a higher rate of anaphylaxis (around 2-5 cases per million doses) compared to influenza vaccines (roughly 1.3 cases per million doses). Age and medical history also play a role—younger adults, particularly females, are more frequently reported to experience anaphylaxis. Healthcare providers are trained to screen for risk factors, such as a history of severe allergies, and to have emergency protocols in place, including the availability of epinephrine, to manage any reactions promptly.
For individuals concerned about anaphylaxis, practical steps can mitigate risk. First, disclose any history of severe allergies to your healthcare provider before vaccination. Second, plan to remain at the vaccination site for 15–30 minutes post-vaccination, as most anaphylactic reactions occur within this window. If you experience symptoms like difficulty breathing, swelling, or a rapid heartbeat, seek immediate medical attention. While the risk is low, awareness and preparedness are key to ensuring safe vaccination experiences for everyone.
Comparatively, the risk of anaphylaxis from vaccines is significantly lower than from common allergens like peanuts or bee stings, which occur in approximately 1 in 50,000 to 1 in 100,000 exposures. This highlights the relative safety of vaccines while underscoring the importance of not dismissing the rare cases that do occur. Public health messaging should balance transparency about risks with reassurance about the overwhelming safety profile of vaccines, fostering trust without alarmism.
In conclusion, the prevalence of anaphylaxis from vaccines—1.3 to 5 cases per million doses—is a testament to the rigorous safety standards in vaccine development and administration. While rare, these reactions remind us of the need for vigilance and preparedness in healthcare settings. By understanding the data, following pre-vaccination screening protocols, and staying informed, individuals and providers can navigate vaccination with confidence, ensuring the benefits far outweigh the minimal risks.
Early Hib Vaccination: Potential Risks and What Parents Should Know
You may want to see also
Explore related products




$44.97 $49.99

![]()
Risk Factors: History of allergies, asthma, or prior anaphylaxis increases vaccine reaction risk
Anaphylaxis from vaccines is rare, occurring in approximately 1.3 cases per million doses administered. However, certain individuals face a higher risk due to specific health histories. A documented history of allergies, asthma, or prior anaphylaxis significantly elevates the likelihood of an adverse vaccine reaction. Understanding these risk factors is crucial for healthcare providers and patients alike to ensure safe vaccination practices.
For those with a history of allergies, particularly to vaccine components like egg protein (common in influenza vaccines) or latex, the risk of anaphylaxis increases. Even trace amounts of allergens can trigger a severe reaction. For example, individuals with egg allergies should receive the influenza vaccine in a medical setting where immediate treatment is available. Similarly, asthma patients, especially those with poorly controlled symptoms, may experience heightened sensitivity to vaccine ingredients, though the exact mechanism remains under study.
Prior anaphylaxis to any cause—whether from food, medications, or insect stings—is a red flag. Such individuals are at a 5 to 10 times greater risk of vaccine-induced anaphylaxis compared to the general population. This heightened risk necessitates careful pre-vaccination screening and, in some cases, consultation with an allergist. For instance, the mRNA COVID-19 vaccines (Pfizer-BioNTech and Moderna) have a reported anaphylaxis rate of 2.5 to 4.7 cases per million doses, with prior anaphylaxis being a key predictor.
Practical steps can mitigate risk. Patients with these histories should inform their healthcare provider before vaccination. Extended observation periods (30 minutes post-vaccination) are recommended for high-risk individuals. In some cases, skin testing or graded dosing (administering the vaccine in small, incremental amounts) may be considered under specialist supervision. Carrying an epinephrine auto-injector (e.g., EpiPen) is advisable for those at elevated risk, ensuring immediate response if symptoms occur.
While the overall risk remains low, awareness of these factors empowers individuals and healthcare providers to make informed decisions. Balancing the benefits of vaccination against potential risks is essential, particularly for those with a history of allergies, asthma, or prior anaphylaxis. Proactive measures and personalized care can ensure safe immunization for even the most vulnerable populations.
Vaccinated vs. Unvaccinated: Analyzing Hospitalization Rates and Trends
You may want to see also
Explore related products


$7.99 $8.49



![]()
Symptoms and Timing: Symptoms typically appear within minutes to hours after vaccination
Anaphylaxis following vaccination is a rare but critical event, with symptoms typically emerging within minutes to hours after the injection. This rapid onset is a hallmark of the body’s hypersensitivity reaction, often triggered by components in the vaccine such as stabilizers, preservatives, or the antigen itself. For instance, the mRNA COVID-19 vaccines have been associated with anaphylaxis rates of approximately 2 to 5 cases per million doses, with symptoms usually appearing within 15 to 30 minutes post-vaccination. Recognizing this narrow window is crucial for healthcare providers and recipients alike, as prompt intervention can prevent severe outcomes.
The symptoms of vaccine-induced anaphylaxis are distinct and require immediate attention. Initial signs may include rapid onset of skin reactions like hives or itching, swelling of the face or throat, and respiratory distress, such as wheezing or difficulty breathing. In severe cases, a drop in blood pressure leading to dizziness or loss of consciousness can occur. For children and adults, monitoring for these symptoms during the 30-minute observation period recommended post-vaccination is essential. Parents should be particularly vigilant with younger age groups, as they may struggle to articulate discomfort.
Understanding the timing of anaphylaxis is not just about recognizing symptoms but also about preparedness. Healthcare facilities administering vaccines must be equipped with epinephrine autoinjectors (e.g., EpiPens) and trained staff to manage reactions swiftly. For individuals with a history of severe allergies, pre-medication with antihistamines or consultation with an allergist before vaccination may be advised, though this should be tailored to the specific vaccine and individual risk profile. Practical tips include scheduling vaccinations during clinic hours when medical assistance is readily available and avoiding strenuous activity immediately afterward.
Comparatively, the timing of anaphylaxis from vaccines contrasts with other adverse reactions, which may take days or weeks to manifest. For example, delayed local reactions to the COVID-19 vaccine, such as injection site swelling or lymphadenopathy, typically occur 2–10 days post-vaccination. This distinction underscores the importance of differentiating between immediate hypersensitivity reactions and other vaccine-related side effects. Public health messaging should emphasize the need for vigilance in the first hour post-vaccination, ensuring that recipients know when and how to seek help if symptoms arise.
In conclusion, the rapid onset of anaphylaxis post-vaccination demands awareness, preparedness, and swift action. By understanding the symptoms and timing, individuals and healthcare providers can mitigate risks effectively. While rare, the potential severity of anaphylaxis highlights the importance of adhering to post-vaccination observation protocols and ensuring access to emergency treatment. This knowledge empowers both recipients and caregivers to navigate vaccination safely, balancing the benefits of immunization with the need for caution.
Does Fox News Support the Vaccine? Analyzing Their Stance and Impact
You may want to see also
Explore related products






![]()
Prevention and Management: Pre-vaccination screening and epinephrine availability reduce severe outcomes
Anaphylaxis from vaccines is a rare but potentially life-threatening event, occurring in approximately 1.31 cases per million vaccine doses administered. While this incidence is low, the severity of anaphylactic reactions underscores the importance of proactive prevention and management strategies. Pre-vaccination screening and ensuring the availability of epinephrine are critical measures that can significantly reduce the risk of severe outcomes.
Step 1: Pre-Vaccination Screening
Before administering any vaccine, healthcare providers should conduct a thorough patient history to identify risk factors for anaphylaxis. Key questions include inquiring about previous allergic reactions to vaccines, components (e.g., gelatin, egg protein, or latex), or medications. Patients with a history of severe allergies, particularly to vaccine components, may require additional evaluation. For example, individuals with egg allergies can safely receive most vaccines, including influenza and COVID-19 vaccines, but consultation with an allergist may be warranted for high-risk cases. Similarly, those with a history of anaphylaxis to a specific vaccine should avoid subsequent doses unless under specialist supervision.
Step 2: Epinephrine Availability
Epinephrine is the first-line treatment for anaphylaxis, and its prompt administration is essential to prevent fatal outcomes. Vaccination sites must be equipped with age-appropriate epinephrine auto-injectors, such as EpiPen (0.3 mg for adults and 0.15 mg for children weighing 15–30 kg). Staff should be trained in recognizing anaphylaxis symptoms—including hives, swelling, difficulty breathing, and hypotension—and in using epinephrine devices. After injection, patients should be monitored for at least 30 minutes post-vaccination, as symptoms can recur.
Cautions and Considerations
While pre-vaccination screening is vital, it is not foolproof, as some individuals may experience anaphylaxis without prior risk factors. Healthcare providers should remain vigilant and prepared for immediate intervention. Additionally, delays in epinephrine administration are associated with poorer outcomes, so accessibility and staff training are non-negotiable. For children, caregivers should be educated on anaphylaxis signs and provided with emergency contact information.
By implementing rigorous pre-vaccination screening and ensuring epinephrine readiness, healthcare systems can minimize the risks associated with vaccine-induced anaphylaxis. These measures not only save lives but also foster public confidence in vaccination programs. As vaccination campaigns continue to evolve, prioritizing these preventive strategies remains paramount.
How to Verify Patient's Pneumococcal Vaccination Status: A Quick Guide
You may want to see also
Frequently asked questions
Anaphylaxis from vaccines is very rare. The estimated rate is approximately 1.3 cases per 1 million vaccine doses administered.
The flu vaccine and COVID-19 vaccines have been most frequently linked to anaphylaxis, though the risk remains extremely low for all vaccines.
Individuals with a history of severe allergies, especially to vaccine components like polyethylene glycol (PEG) or polysorbate, may be at slightly higher risk.
Seek immediate medical attention. Symptoms include difficulty breathing, swelling of the face or throat, rapid heartbeat, and dizziness. Anaphylaxis is a medical emergency and requires prompt treatment.