Vaccines undergo rigorous testing for efficacy through a multi-stage process to ensure safety and effectiveness before approval. This process begins with preclinical studies, where potential vaccines are tested in laboratory settings and animal models to assess their immune response and safety. If successful, the vaccine advances to clinical trials, which are conducted in three phases. Phase 1 trials focus on safety and dosage in a small group of healthy volunteers, while Phase 2 expands to a larger group to evaluate immunogenicity and side effects. Phase 3 involves thousands of participants to determine the vaccine’s efficacy in preventing disease and to monitor long-term safety. Regulatory agencies, such as the FDA or WHO, review the data from these trials to ensure the vaccine meets stringent standards before granting approval. Post-approval, ongoing surveillance through Phase 4 studies continues to monitor the vaccine’s performance in real-world populations, ensuring its safety and efficacy over time.
Explore related products

$59.84 $62.99

$137.51 $58.99




What You'll Learn
- Preclinical Testing: Animal studies assess safety, immunogenicity, and potential efficacy before human trials
- Phase 1 Trials: Small human trials evaluate safety, dosage, and immune response in healthy volunteers
- Phase 2 Trials: Expanded trials test vaccine efficacy, side effects, and optimal dosing in target groups
- Phase 3 Trials: Large-scale trials compare vaccinated vs. placebo groups to measure disease prevention rates
- Post-Approval Monitoring: Ongoing surveillance tracks long-term efficacy and rare side effects in real-world use
![]()
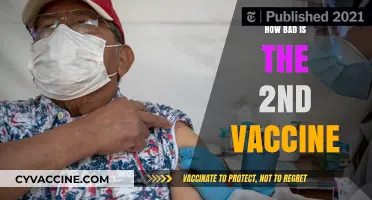
Preclinical Testing: Animal studies assess safety, immunogenicity, and potential efficacy before human trials
Before any vaccine candidate advances to human trials, it undergoes rigorous preclinical testing in animals to evaluate safety, immunogenicity, and potential efficacy. This critical phase serves as a safeguard, ensuring that only the most promising and least risky candidates proceed further. Animal models, ranging from mice and rats to non-human primates, are selected based on their biological similarity to humans and their ability to mimic the disease in question. For instance, in the development of the COVID-19 vaccine, researchers used rhesus macaques to study immune responses and protection against the SARS-CoV-2 virus. These studies are not just a formality; they are a cornerstone of vaccine development, providing essential data to predict how a vaccine might perform in humans.
The first step in preclinical testing is assessing safety. Animals are administered varying doses of the vaccine candidate—often starting with low doses (e.g., 0.1 μg) and escalating to higher levels (e.g., 100 μg)—to identify potential adverse effects, such as inflammation, toxicity, or systemic reactions. For example, in the case of the HPV vaccine, preclinical studies in rabbits and guinea pigs revealed no significant safety concerns, paving the way for human trials. This phase also includes monitoring for long-term effects, ensuring the vaccine does not cause harm over time. Safety data from animal studies are meticulously reviewed by regulatory agencies like the FDA before human trials are approved.
Immunogenicity—the ability of a vaccine to provoke an immune response—is another key focus. Researchers measure antibody production, T-cell activation, and other immune markers in the animal models. For the influenza vaccine, preclinical studies in ferrets demonstrated robust antibody responses, which correlated with protection against the virus. These findings are crucial because they help scientists determine the optimal dosage and formulation. For instance, a vaccine candidate might require adjuvants (substances that enhance immune response) if initial studies show weak immunogenicity. Practical tips for researchers include standardizing testing protocols and using control groups to ensure accurate comparisons.
Efficacy testing in animals aims to predict how well the vaccine will protect against the target disease. This often involves challenging vaccinated animals with the pathogen to see if they remain healthy. In the development of the Ebola vaccine, preclinical studies in non-human primates showed that vaccinated animals survived exposure to the virus, while unvaccinated controls did not. Such results provide a strong rationale for advancing to human trials. However, it’s important to note that animal models are not perfect predictors of human outcomes. Researchers must carefully interpret the data, considering species differences and the complexity of human immune systems.
In conclusion, preclinical testing in animals is a multifaceted process that balances scientific inquiry with ethical considerations. It requires precision, from selecting the right animal models to interpreting complex immunological data. While this phase is resource-intensive and time-consuming, it is indispensable for identifying safe and effective vaccine candidates. By thoroughly assessing safety, immunogenicity, and efficacy in animals, researchers can minimize risks and maximize the likelihood of success in subsequent human trials. This foundational step underscores the meticulous approach required in vaccine development, ensuring public health remains the ultimate priority.
Georgia's Vaccine Recall Management: Who Tracks and Oversees Safety?
You may want to see also
Explore related products






![]()
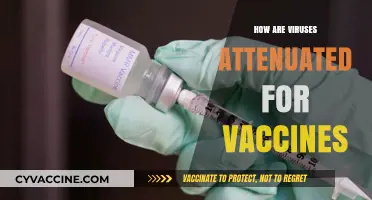
Phase 1 Trials: Small human trials evaluate safety, dosage, and immune response in healthy volunteers
Before a vaccine candidate advances to larger trials, it must prove its mettle in Phase 1, a critical juncture where safety and potential are scrutinized in a controlled, small-scale human setting. This phase typically involves 20 to 100 healthy volunteers, often aged 18 to 55, though specific age ranges may vary based on the vaccine's target population. The primary objectives are threefold: ensure the vaccine doesn't harm participants, determine the optimal dosage, and assess whether it elicits an immune response. Participants are closely monitored for adverse reactions, with dosages starting low and escalating only if the initial levels prove safe. For instance, a COVID-19 vaccine trial might begin with a 10-microgram dose, increasing to 50 micrograms in subsequent cohorts if no serious side effects are observed. This stepwise approach minimizes risk while gathering essential data on the vaccine's behavior in the human body.
Consider the logistical intricacies of Phase 1 trials: participants are often divided into groups, each receiving a different dose or a placebo. Blood samples are taken at regular intervals—sometimes weekly—to measure antibody levels and other immune markers. Researchers also document side effects, from mild soreness at the injection site to more severe systemic reactions like fever or fatigue. These trials are not just about identifying problems but also about understanding the vaccine's mechanism. For example, a vaccine targeting influenza might show a significant increase in neutralizing antibodies within 28 days of administration, a key indicator of its potential efficacy. Such data inform not only the vaccine's safety profile but also its likelihood of success in later phases.
A persuasive argument for the importance of Phase 1 trials lies in their role as a gatekeeper. Without rigorous evaluation at this stage, flawed or dangerous vaccines could advance, wasting resources and endangering lives. Take the case of a dengue vaccine candidate that showed promise in early animal studies but caused severe complications in humans when dosages were not carefully calibrated. Phase 1 trials could have identified these risks earlier, preventing broader harm. By prioritizing safety and immune response, this phase ensures that only the most viable candidates proceed, safeguarding public trust in the vaccination process.
Practical tips for participants in Phase 1 trials include maintaining a detailed symptom journal, as even minor changes can provide valuable insights. Volunteers should also be prepared for frequent clinic visits and blood draws, which, while inconvenient, are essential for comprehensive data collection. For researchers, transparency is key—clearly communicating risks and expectations fosters trust and ensures informed consent. Ultimately, Phase 1 trials are a delicate balance of caution and ambition, laying the groundwork for vaccines that could one day protect millions. Their meticulous design and execution underscore the scientific rigor behind every vaccine that reaches the market.
Does the COVID-19 Vaccine Protect Against the UK Strain?
You may want to see also
Explore related products


$48.53 $96.95




![]()
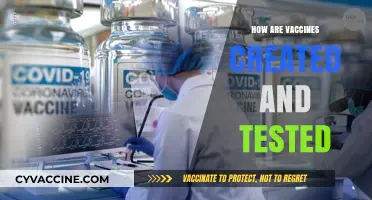
Phase 2 Trials: Expanded trials test vaccine efficacy, side effects, and optimal dosing in target groups
Phase 2 trials mark a critical juncture in vaccine development, expanding the scope of testing to include larger, more diverse populations. Here, the focus shifts from initial safety assessments to a deeper exploration of efficacy, side effects, and optimal dosing within specific target groups. This phase typically involves several hundred volunteers, often stratified by age, health status, or other relevant factors, to ensure the vaccine’s performance is thoroughly evaluated across different demographics. For instance, a vaccine targeting respiratory infections might include groups aged 18–40, 41–65, and over 65 to assess age-related variations in immune response.
One of the primary objectives of Phase 2 is to determine the optimal dosage—the balance between maximizing efficacy and minimizing adverse effects. Researchers test multiple dose levels, such as 25 µg, 50 µg, and 100 µg, to identify the lowest effective dose that triggers a robust immune response without causing undue side effects. This step is crucial for vaccines like the HPV vaccine, where dosing precision ensures long-term protection while avoiding unnecessary discomfort. Participants are closely monitored for reactions, with common side effects like mild fever, fatigue, or injection site pain documented to refine safety profiles.
Efficacy testing in Phase 2 goes beyond measuring antibody levels; it also evaluates how well the vaccine prevents infection or reduces disease severity in controlled settings. For example, in a trial for a flu vaccine, participants might be exposed to the virus in a challenge study, or their immune responses might be compared to those of a placebo group. This phase often employs randomized, double-blind designs to eliminate bias, ensuring that both researchers and participants are unaware of who receives the vaccine or placebo until the trial concludes.
Practical considerations for participants include adhering to strict trial protocols, such as maintaining a symptom diary, attending regular follow-up visits, and avoiding other vaccinations during the study period. For researchers, the challenge lies in balancing speed and rigor, as Phase 2 data must be robust enough to justify advancing to larger, more complex Phase 3 trials. The takeaway is clear: Phase 2 trials are not just about proving a vaccine works—they’re about fine-tuning its application to ensure it works safely and effectively for the people who need it most.
Janssen Vaccine Booster: Availability, Effectiveness, and What You Need to Know
You may want to see also
Explore related products






![]()
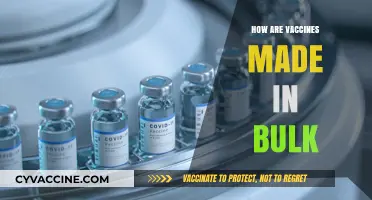
Phase 3 Trials: Large-scale trials compare vaccinated vs. placebo groups to measure disease prevention rates
Phase 3 trials are the crucible where a vaccine’s real-world potential is forged. Tens of thousands of volunteers, often spanning diverse age groups (e.g., 18–85 years), are randomly assigned to receive either the vaccine candidate or a placebo. This massive scale is deliberate: it’s designed to detect even modest differences in disease prevention rates between the two groups. For instance, in the COVID-19 vaccine trials, participants received two doses, 21–28 days apart, with researchers meticulously tracking who contracted the virus over months. The goal? To determine if the vaccine reduces disease incidence by a statistically significant margin, typically aiming for at least 50% efficacy as a regulatory threshold.
Consider the logistical ballet of these trials. Participants must adhere to strict protocols: maintaining health diaries, attending regular check-ups, and reporting any symptoms immediately. Placebo groups are given an inert substance (e.g., saline solution) to blind both participants and researchers, ensuring bias doesn’t skew results. For example, in the Pfizer-BioNTech trial, 43,000 participants were enrolled across six countries, with 170 COVID-19 cases analyzed to conclude 95% efficacy. Such trials aren’t just about numbers—they’re about proving a vaccine’s ability to protect under real-life conditions, from crowded cities to remote villages.
Yet, Phase 3 trials aren’t without challenges. Ensuring diverse representation is critical but difficult. Early COVID-19 trials struggled to enroll enough older adults and minorities, groups disproportionately affected by the virus. Practical tips for trial designers include partnering with community organizations to build trust and offering flexible participation options, such as mobile clinics. Another hurdle is maintaining the placebo group’s integrity. If a vaccine proves highly effective mid-trial, ethical guidelines often require offering the vaccine to placebo recipients, complicating long-term data collection.
The takeaway is clear: Phase 3 trials are the gold standard for measuring vaccine efficacy, but their success hinges on meticulous planning, inclusivity, and adaptability. They don’t just test a vaccine—they test the system’s ability to deliver it effectively. For anyone following vaccine development, understanding these trials demystifies the headlines and underscores why their scale and rigor are non-negotiable.
Debunking Myths: The Truth About Vaccines and Fetal Tissue Research
You may want to see also
Explore related products



$44.99 $59.99


![]()
Post-Approval Monitoring: Ongoing surveillance tracks long-term efficacy and rare side effects in real-world use
Vaccine approval marks not the end, but a new phase of scrutiny. Post-approval monitoring is the sentinel that stands guard, ensuring the vaccine’s promise holds true in the unpredictable theater of real-world use. Unlike clinical trials, which operate in controlled environments with preselected populations, this phase captures data from millions of individuals across diverse demographics, health statuses, and geographies. It’s here that rare side effects, too infrequent to surface in trials, may emerge, and long-term efficacy is rigorously tested against evolving pathogens and varying adherence to dosing schedules (e.g., a two-dose regimen spaced 3–4 weeks apart for mRNA vaccines).
Consider the COVID-19 vaccines, which underwent expedited approval but were swiftly subjected to post-approval surveillance. Systems like the CDC’s Vaccine Adverse Event Reporting System (VAERS) and the Vaccine Safety Datalink (VSD) played pivotal roles. For instance, the rare incidence of thrombosis with thrombocytopenia syndrome (TTS) following the Johnson & Johnson vaccine was identified through these channels, leading to updated guidelines restricting its use to specific age groups (e.g., adults over 50). Similarly, ongoing monitoring of mRNA vaccines (Pfizer-BioNTech and Moderna) continues to assess durability of immunity, with booster recommendations adjusted based on real-world data showing waning efficacy after 6–8 months.
The process isn’t passive; it’s proactive and adaptive. Pharmacovigilance teams analyze data streams in near real-time, flagging anomalies that warrant investigation. For example, if a cluster of myocarditis cases is reported in young males post-vaccination, as seen with mRNA vaccines, studies are initiated to confirm causality and refine risk-benefit profiles. This iterative approach ensures that safety protocols evolve—such as the recommendation to space doses by 8 weeks in younger populations to mitigate risk.
Practical tips for healthcare providers and recipients are integral to this system. Providers should report any adverse events, even if uncertain of causality, using platforms like VAERS. Patients, especially those in high-risk categories (e.g., immunocompromised individuals or pregnant women), should remain vigilant for symptoms post-vaccination and seek medical advice promptly. Public health campaigns must emphasize that post-approval monitoring is a feature, not a flaw, of the vaccine ecosystem—a testament to its commitment to transparency and continuous improvement.
In essence, post-approval monitoring is the bridge between clinical promise and public trust. It transforms static trial data into a living, breathing narrative of vaccine performance, ensuring that every dose administered is backed by the most current evidence. As pathogens evolve and populations shift, this surveillance remains our best tool to adapt, protect, and persevere.
Toxoid Vaccines: Unlocking Long-Term Immunity Against Deadly Bacterial Toxins
You may want to see also
Frequently asked questions
Vaccines are initially tested in preclinical trials using laboratory studies and animal models to assess safety and immune response before moving to human trials.
Vaccine efficacy is tested in three phases: Phase 1 (safety and dosage in small groups), Phase 2 (expanded safety and immune response in larger groups), and Phase 3 (large-scale trials to evaluate efficacy and side effects).
Vaccine efficacy is measured by comparing the number of infections in a vaccinated group versus a placebo or control group, expressed as a percentage reduction in disease risk.
Regulatory agencies like the FDA or EMA review clinical trial data to ensure vaccines meet safety, quality, and efficacy standards before approving them for public use.
Post-approval, vaccines are monitored through surveillance systems like the CDC’s VAERS and VSD to track long-term efficacy, rare side effects, and real-world performance.