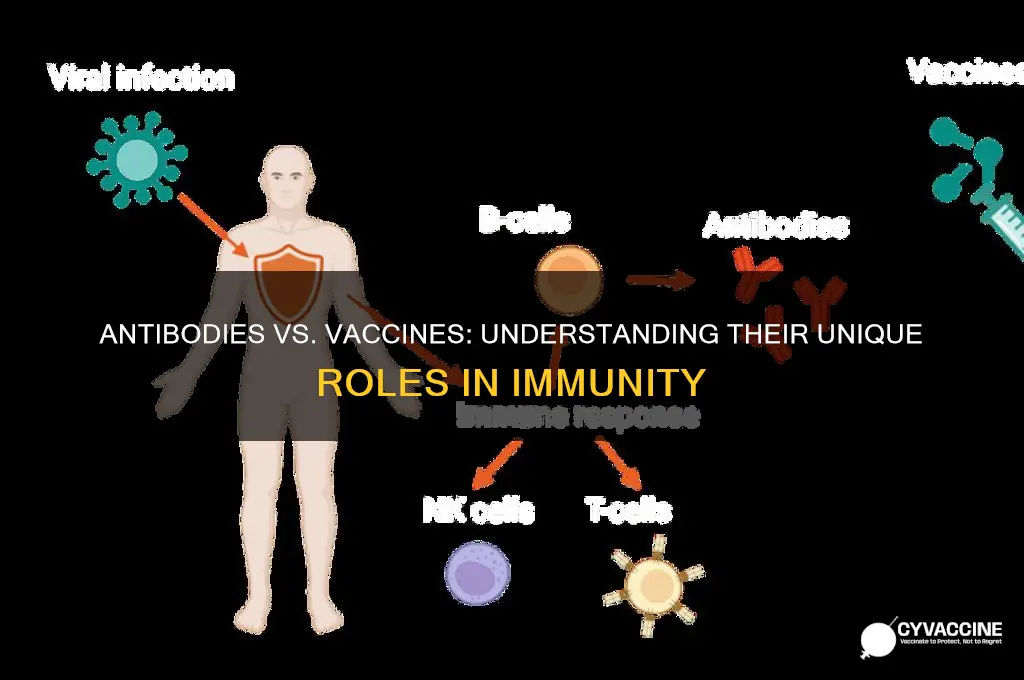
Antibodies and vaccines are both crucial components of the immune system, but they serve distinct roles in protecting the body against pathogens. Antibodies, also known as immunoglobulins, are Y-shaped proteins produced by the immune system in response to the presence of foreign substances, such as bacteria or viruses. They act as a targeted defense mechanism, binding to specific antigens on pathogens to neutralize them or mark them for destruction by other immune cells. In contrast, vaccines are biological preparations that stimulate the immune system to recognize and combat specific pathogens without causing the disease itself. Vaccines work by introducing a harmless form of the pathogen (or its components) to the body, prompting the immune system to produce memory cells and antibodies, thereby providing long-term immunity. While antibodies are a direct response to an existing infection, vaccines are a preventive measure designed to prepare the immune system for future encounters with pathogens.
Explore related products






What You'll Learn
- Origin: Antibodies are proteins produced by the body; vaccines are external substances administered to stimulate immunity
- Function: Antibodies neutralize pathogens directly; vaccines train the immune system to produce antibodies
- Duration: Antibodies provide immediate but temporary protection; vaccines offer long-term immunity
- Specificity: Antibodies target specific pathogens; vaccines prepare the body for multiple strains
- Administration: Antibodies are given as treatment; vaccines are preventive measures
![]()
Origin: Antibodies are proteins produced by the body; vaccines are external substances administered to stimulate immunity
Antibodies and vaccines, though both critical to immunity, originate from fundamentally different sources. Antibodies are the body’s homegrown defense team—proteins produced by B cells in response to a detected threat, such as a virus or bacteria. This process is part of the adaptive immune system, tailored to recognize and neutralize specific pathogens. Vaccines, on the other hand, are external interventions. They introduce a harmless piece of a pathogen (like a protein or weakened virus) to train the immune system to recognize and combat future threats. While antibodies are a reaction, vaccines are a proactive measure, priming the body for potential encounters.
Consider the timeline of their action. Antibodies typically appear days after an infection or vaccination, as the immune system identifies and responds to the invader. For instance, after a COVID-19 infection, detectable antibodies usually emerge within 1–3 weeks. Vaccines, however, operate on a preventive schedule. The CDC recommends a 2-dose mRNA COVID-19 vaccine series spaced 3–4 weeks apart, followed by boosters every 6–12 months for vulnerable populations. This deliberate timing allows the immune system to build memory cells, ensuring a faster, stronger response if the real pathogen appears.
The production of antibodies is a highly personalized process. Each individual’s immune system generates unique antibodies based on their genetic makeup and immune history. Vaccines, in contrast, are standardized formulations designed to elicit a broad immune response across diverse populations. For example, the influenza vaccine is updated annually to target the most prevalent strains, but its core mechanism—introducing viral proteins—remains consistent. This uniformity ensures widespread protection, whereas antibodies are as varied as the people who produce them.
A practical takeaway: while antibodies provide immediate defense (either naturally or post-vaccination), vaccines are a long-term investment in immunity. For instance, a single dose of the measles vaccine confers lifelong protection in 95% of recipients by stimulating the production of memory B cells. Antibodies from a natural measles infection also offer lifelong immunity but carry the risk of severe complications. Vaccines bypass this danger, offering the benefits of immunity without the risks of disease. Understanding this distinction empowers individuals to make informed decisions about their health, balancing immediate needs with future resilience.
Vaccination: Weighing Lifesaving Benefits Against Potential Risks and Concerns
You may want to see also
Explore related products






![]()
Function: Antibodies neutralize pathogens directly; vaccines train the immune system to produce antibodies
Antibodies and vaccines serve distinct roles in the body's defense against pathogens, each with a unique mechanism of action. Antibodies, also known as immunoglobulins, are Y-shaped proteins produced by plasma cells, a type of white blood cell. Their primary function is to neutralize pathogens directly by binding to specific antigens on the surface of bacteria, viruses, or other foreign substances. This binding process can block the pathogen's ability to infect cells, tag it for destruction by other immune cells, or activate the complement system, a cascade of immune responses that help eliminate the threat. For instance, monoclonal antibody treatments like those used for COVID-19 provide immediate, targeted protection by delivering lab-created antibodies directly into the bloodstream, offering rapid defense for high-risk individuals.
Vaccines, on the other hand, operate on a fundamentally different principle. Instead of directly neutralizing pathogens, vaccines train the immune system to recognize and respond to specific threats. They achieve this by introducing a harmless version or component of a pathogen, such as a weakened virus, inactivated pathogen, or a fragment of its protein. This exposure prompts the immune system to produce memory cells, which "remember" the pathogen and can quickly mobilize antibodies if the real threat appears in the future. For example, the mRNA vaccines for COVID-19, like Pfizer-BioNTech and Moderna, deliver genetic instructions for cells to produce a harmless piece of the virus’s spike protein, triggering antibody production without causing illness. This process typically requires a series of doses—often two or three—spaced weeks apart to build robust immunity.
The timing and duration of protection also highlight the functional differences between antibodies and vaccines. Antibodies, whether naturally produced or administered as treatments, provide immediate but temporary protection. For instance, monoclonal antibody treatments for COVID-19 are most effective when given within 10 days of symptom onset and offer protection for a few weeks. In contrast, vaccines build long-term immunity, often lasting years, by training the immune system to respond swiftly and effectively. Booster shots may be needed to maintain this immunity, as seen with the annual flu vaccine or COVID-19 boosters, which account for viral mutations and waning immunity.
Practical considerations further underscore these differences. Antibody treatments are typically reserved for specific scenarios, such as high-risk individuals exposed to a pathogen or those with compromised immune systems. They are administered via intravenous infusion or injection and require medical supervision. Vaccines, however, are designed for widespread use, often starting in childhood with schedules like the CDC’s recommended immunization timeline for ages 0–18. Vaccines are generally administered via intramuscular injection, are cost-effective for public health, and can be self-administered in some cases, such as nasal spray vaccines.
In summary, while antibodies act as the immune system’s immediate responders, directly neutralizing pathogens, vaccines function as trainers, preparing the body to produce antibodies efficiently upon future encounters. Understanding these distinctions is crucial for making informed decisions about when to use antibody treatments versus vaccines, ensuring optimal protection against infectious diseases. For instance, a healthy individual might prioritize vaccination for long-term immunity, while someone exposed to a high-risk pathogen could benefit from immediate antibody treatment as a stopgap measure.
Key Traits of Effective Vaccines: Safety, Efficacy, and Accessibility Explained
You may want to see also
Explore related products





![]()
Duration: Antibodies provide immediate but temporary protection; vaccines offer long-term immunity
Antibodies and vaccines both play critical roles in protecting the body from pathogens, but their timelines of action differ significantly. Antibodies, whether naturally produced or administered through treatments like monoclonal antibody therapies, act rapidly to neutralize threats. For instance, a COVID-19 monoclonal antibody infusion can start working within hours to combat the virus, providing immediate relief for high-risk individuals. However, this protection is fleeting, typically lasting only a few weeks to months, depending on the dosage and the body’s clearance rate. In contrast, vaccines operate on a longer horizon, training the immune system to recognize and combat pathogens over years or even decades. This fundamental difference in duration underscores their complementary roles in public health strategies.
Consider the practical implications of these timelines. For someone exposed to a virus like influenza, receiving antibody therapy could prevent severe illness in the short term, but it wouldn’t protect them from future infections. Vaccines, on the other hand, offer sustained defense. The measles vaccine, for example, provides immunity for a lifetime after two doses, administered at 12–15 months and 4–6 years of age. This long-term protection reduces the need for repeated interventions, making vaccines a cornerstone of preventive medicine. However, in emergencies or for immunocompromised individuals, the immediate but temporary shield of antibodies can be lifesaving, even if it doesn’t replace the enduring benefits of vaccination.
The mechanisms behind these duration differences highlight their distinct purposes. Antibodies are pre-formed proteins that directly target pathogens, a ready-made solution for urgent needs. Vaccines, however, introduce a weakened or inactivated pathogen (or its components) to stimulate the immune system’s memory. This process takes time—typically weeks—as the body produces its own antibodies and memory cells. For instance, the Pfizer-BioNTech COVID-19 vaccine requires two doses, spaced three weeks apart, to achieve full efficacy, with booster shots recommended every 6–12 months to maintain immunity. This phased approach contrasts sharply with the instant but transient action of antibody treatments.
From a public health perspective, understanding these timelines is crucial for tailoring interventions. During an outbreak, antibody treatments can be deployed to protect vulnerable populations immediately, while vaccination campaigns build long-term herd immunity. For example, during the 2014 Ebola outbreak, antibody-based therapies were used to treat infected individuals, while vaccine development focused on preventing future waves. Similarly, in managing seasonal flu, high-risk groups like the elderly or pregnant women might benefit from both annual vaccinations and antibody treatments if exposed. Balancing these tools requires careful consideration of their unique duration profiles.
In practice, individuals should weigh these differences when making health decisions. If traveling to an area with a high risk of mosquito-borne diseases like dengue, a vaccine (where available) would provide lasting protection, whereas antibody treatments would only offer temporary coverage. Parents should follow pediatric vaccination schedules rigorously to ensure children develop long-term immunity against diseases like mumps or rubella. Meanwhile, healthcare providers might recommend antibody therapies for patients with compromised immune systems who cannot mount a response to vaccines. By recognizing the distinct durations of antibodies and vaccines, we can deploy them more effectively to safeguard health across timeframes.
Novavax vs. mRNA Vaccines: Key Differences and Effectiveness Explained
You may want to see also
Explore related products




![]()
Specificity: Antibodies target specific pathogens; vaccines prepare the body for multiple strains
Antibodies are precision tools in the immune system's arsenal, each designed to recognize and neutralize a specific pathogen, such as a virus or bacterium. This specificity is their strength—a lock-and-key mechanism where the antibody binds to a unique antigen on the pathogen, marking it for destruction. For instance, if you’ve recovered from the flu, your body produces antibodies tailored to that particular strain of the influenza virus. However, this precision comes with a limitation: these antibodies are ineffective against even slightly different strains or other pathogens. This is why you can still catch the flu again if a new strain emerges.
Vaccines, on the other hand, operate on a broader scale. They train the immune system to recognize and combat multiple strains of a pathogen by introducing a weakened, inactivated, or fragment of the pathogen. For example, the seasonal flu vaccine contains antigens from four different flu strains predicted to be prevalent that year. This approach doesn’t rely on a single antibody but instead stimulates the production of a diverse array of immune cells and antibodies capable of responding to various threats. It’s like teaching the immune system to recognize a family of intruders rather than just one.
Consider the COVID-19 pandemic as a case study. Monoclonal antibody treatments, such as those developed by Regeneron, were highly effective against specific variants of the SARS-CoV-2 virus but became less useful as new variants like Delta and Omicron emerged. In contrast, vaccines like Pfizer-BioNTech and Moderna, which use mRNA technology, have been updated to target multiple variants, providing broader protection. This adaptability highlights the difference in specificity between antibodies and vaccines—one is a sniper, the other a well-trained army.
For practical application, understanding this difference is crucial. If you’re exposed to a specific pathogen, such as measles, receiving immunoglobulin (a concentrated antibody treatment) within 6 days can provide immediate protection. However, for long-term defense against measles and its various strains, the MMR vaccine is recommended, typically administered in two doses—the first at 12–15 months of age and the second at 4–6 years. This dual approach leverages the strengths of both antibodies and vaccines, offering both immediate and sustained immunity.
In summary, while antibodies excel at targeting specific pathogens with surgical precision, vaccines prepare the immune system to tackle a wider range of threats. This distinction underscores why vaccines are foundational to public health, while antibody treatments serve as targeted interventions. By combining both, we can address both immediate and long-term immune challenges effectively.
Hong Kong's Vaccination Rate: Current Status and Public Health Insights
You may want to see also
Explore related products






![]()
Administration: Antibodies are given as treatment; vaccines are preventive measures
Antibodies and vaccines serve distinct roles in the realm of medicine, primarily differentiated by their timing and purpose in addressing health threats. While vaccines are administered proactively to prevent infections, antibodies are deployed reactively to treat existing illnesses. This fundamental distinction in administration underscores their unique mechanisms and applications.
Consider the process of receiving a vaccine. Vaccines, such as the annual influenza shot or the childhood MMR (measles, mumps, rubella) vaccine, are typically given in standardized doses based on age and weight. For instance, the COVID-19 mRNA vaccines (Pfizer-BioNTech and Moderna) are administered in two doses, 3–4 weeks apart for adults, with a lower dosage for children aged 5–11. These doses stimulate the immune system to produce memory cells, preparing the body to recognize and combat the pathogen if exposed in the future. Vaccines are often given intramuscularly (e.g., deltoid muscle) or subcutaneously, with specific instructions to ensure proper absorption and efficacy.
In contrast, antibodies are administered as a treatment after an infection has occurred. Monoclonal antibody therapies, like those used for severe COVID-19 cases, are given intravenously in a single dose, typically ranging from 400 to 1,200 mg depending on the patient’s condition. These antibodies act immediately, neutralizing the pathogen without requiring the immune system to mount its own response. For example, the Regeneron antibody cocktail is administered in a one-time infusion over 20–30 minutes, often in a clinical setting to monitor for potential allergic reactions. This treatment is particularly critical for immunocompromised individuals who may not respond effectively to vaccines.
The timing of administration further highlights the difference. Vaccines are scheduled in advance, often as part of routine healthcare (e.g., childhood immunization schedules). Antibodies, however, are given on an as-needed basis, typically within a specific window after symptom onset or exposure. For instance, COVID-19 monoclonal antibodies are most effective when administered within 10 days of symptom onset. This urgency contrasts with the preventive, planned nature of vaccination campaigns.
Practically, this distinction influences patient care strategies. Vaccines are a cornerstone of public health, reducing disease prevalence through herd immunity. Antibodies, on the other hand, are a targeted intervention for individuals already affected, often serving as a bridge until the immune system can recover. For example, RSV (respiratory syncytial virus) prophylaxis with monoclonal antibodies is given monthly to high-risk infants during RSV season, illustrating how antibodies can also be used semi-preventively in specific populations.
In summary, the administration of antibodies and vaccines reflects their opposing roles: vaccines as a shield, antibodies as a sword. Understanding this difference is crucial for healthcare providers and patients alike, ensuring the right tool is used at the right time to maximize health outcomes.
Maryland's Vaccination Progress: Adult Coverage Rates and Insights
You may want to see also
Frequently asked questions
Antibodies are proteins produced by the immune system to neutralize or destroy specific pathogens, such as viruses or bacteria. They act directly against the pathogen once it enters the body. Vaccines, on the other hand, are biological preparations that stimulate the immune system to produce antibodies and memory cells, preparing the body to fight off future infections before exposure to the pathogen.
Yes, antibodies provide immediate protection by directly targeting and neutralizing pathogens already present in the body. This is often seen in treatments like monoclonal antibody therapies. Vaccines, however, take time to build immunity, typically weeks to months, as they train the immune system to recognize and respond to a pathogen. Once immunity is established, vaccines offer long-term protection against future infections.
No, antibodies cannot replace vaccines. While antibodies provide immediate protection, they are often short-lived and specific to the pathogen they target. Vaccines, however, induce the immune system to produce its own antibodies and memory cells, offering broader and more durable protection. Vaccines are a preventive measure, whereas antibodies are primarily used for treatment or short-term prevention in specific cases.